Capitellum Fractures in the Pediatric Population: A Case Report
Luís B Pinto, Rita F Castro, Luís Fabião, Nuno V Ferreira, Tânia Freitas

TL;DR
This paper presents a rare case of a pediatric capitellum fracture and highlights the importance of advanced imaging and timely surgical treatment for successful recovery.
Contribution
The case emphasizes the diagnostic challenges and effective surgical management of a rare pediatric elbow fracture.
Findings
Capitellum fractures in children are often missed on initial radiographs and require advanced imaging for diagnosis.
Surgical treatment with anatomical reduction and bioabsorbable fixation led to excellent recovery in this case.
Early recognition and intervention are crucial for favorable outcomes in pediatric capitellum fractures.
Abstract
Capitellum fractures are rare injuries in the pediatric population. Their diagnosis is particularly challenging due to the predominantly cartilaginous nature of the pediatric elbow, which often limits the sensitivity of conventional radiographs. Consequently, these fractures are frequently overlooked at initial presentation. We present the case of a nine-year-old boy who sustained indirect trauma to the left elbow after a fall from standing height. On clinical examination, the patient complained of pain, mainly in the lateral aspect of the elbow, with refusal to actively mobilize the joint and marked discomfort during passive motion. Initial plain radiographs were inconclusive. Given the high index of clinical suspicion, further evaluation with computed tomography (CT) was performed, which revealed a Kocher-Lorenz fracture of the capitellum (Bryan and Morrey type II). Surgical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
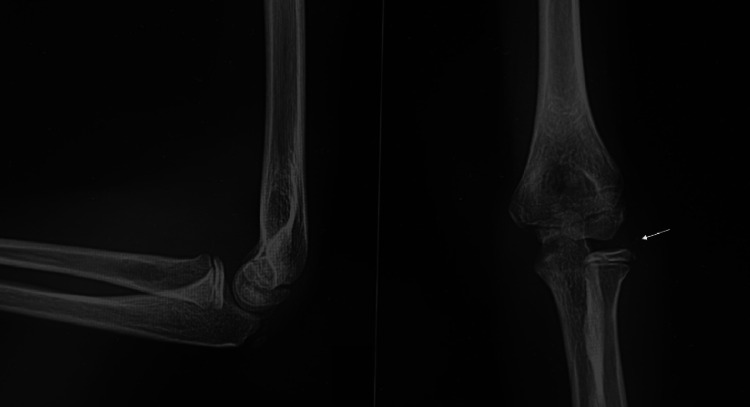 Figure 1
Figure 1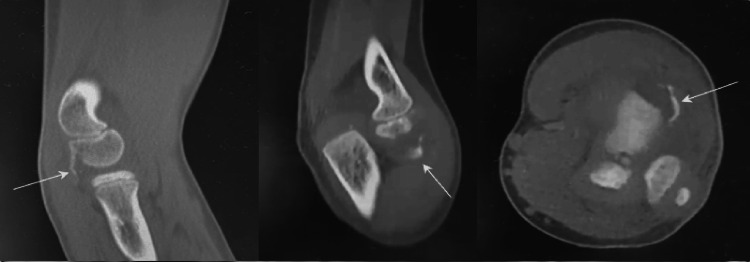 Figure 2
Figure 2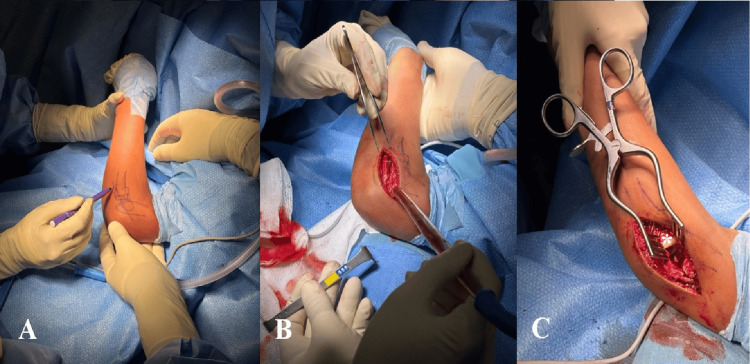 Figure 3
Figure 3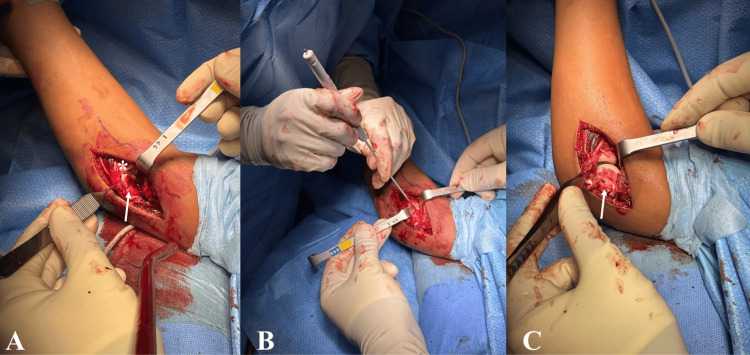 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Shoulder Injury and Treatment · Ear Surgery and Otitis Media
Introduction
Isolated capitellum fractures are an extremely rare entity in the pediatric population, accounting for less than 1% of fractures in children and being even rarer in patients younger than 12 years of age [1-4].
From a mechanical standpoint, capitellum fractures most commonly result from an axial load transmitted through the elbow in extension or slight flexion following a fall onto an outstretched hand (FOOSH). These injuries frequently occur in association with radial head fractures and/or lateral ulnar collateral ligament injuries [1,2,5].
Currently, the most widely used classification system is the Bryan and Morrey classification, which describes these fractures in four types: Type I, or Hahn-Steinthal fracture, characterized by a large osseous fragment of the capitellum that often includes an adjacent portion of the trochlea; Type II, or Kocher-Lorenz fracture, consisting of a smaller fragment composed predominantly of cartilage with minimal subchondral bone; Type III, which includes comminuted capitellum fractures; and Type IV, described by McKee, referring to fractures with a coronal shear pattern involving the capitellum and trochlea [6].
The rarity of these injuries, combined with the anatomical complexity of the growing elbow and the presence of unfused ossification centers, makes diagnosis particularly challenging. Consequently, these fractures are frequently overlooked on initial radiographs. Clinical findings such as ecchymosis, swelling, lateral elbow pain with localized tenderness over the radiocapitellar joint, painful limitation of elbow range of motion, and mechanical block to flexion/extension and/or pronation/supination should raise suspicion of a capitellar fracture. A high index of suspicion and careful clinical evaluation are therefore essential; in selected cases, additional imaging studies with computed tomography (CT) may be required to confirm the diagnosis and accurately define the fracture pattern [1,5,7,8]. For this reason, they have been included among TRASH (The Radiographic Appearance Seemed Harmless) lesions [9].
Surgical treatment is required in the vast majority of cases; the primary goals are anatomical reduction of the articular surface and stable fixation to allow early mobilization and minimize the risk of late complications such as stiffness, osteochondritis, or post-traumatic osteoarthritis [1,2,8,10,11]. Given the rarity of this injury, there is a lack of sufficiently robust studies in the literature to establish well-founded treatment guidelines for capitellum fractures in the pediatric population, particularly in younger children (<12 years). To the best of the authors’ knowledge, at the time of writing, there have been no reported cases of this fracture pattern in such a young patient (nine years old). Therefore, the purpose of this case report is to contribute to the growing body of evidence and knowledge regarding this traumatic pathology, with particular emphasis on diagnostic challenges and surgical management.
Case presentation
A nine-year-old male patient sustained a fall from standing height, resulting in indirect trauma to the left elbow. He had no relevant past medical history. On physical examination, the patient had swelling and pain over the lateral aspect of the elbow, with refusal to actively mobilize the elbow and guarding during attempted passive motion, particularly with attempted passive forearm pronation and supination.
Conventional radiographs were obtained and did not reveal clear acute traumatic changes, except for the presence of a positive fat pad sign and small osseous fragments within the radiocapitellar joint. Given the high index of clinical suspicion, a CT scan was performed, which demonstrated a Kocher-Lorenz fracture (Bryan-Morrey type II) (Figures 1-2).
Left elbow radiographs: lateral and anteroposterior viewsBony fragments in the radiocapitellar joint (white arrow).
CT scanFrom left to right: lateral view, posteroanterior view, and axial view showing a Kocher-Lorenz fracture with posterolateral displacement (white arrows).
The patient underwent surgical treatment under general anesthesia, in the supine position with the use of a tourniquet. Perioperative antibiotic prophylaxis with cefazolin for 24 hours was administered. The surgical approach chosen was a lateral elbow approach using the Kocher interval, with open reduction and internal fixation (ORIF) of the fragment using bioabsorbable darts from Arthrex® (Arthrex, Inc., Naples, Florida, United States). The patient was discharged the day after surgery. Postoperatively, the patient was immobilized in an above-elbow cast for three weeks. After this period, rehabilitation was initiated with good clinical progression, and the patient returned to sports activities three months after surgery (Figures 3-4).
*Lateral approach to the elbow through the Kocher intervalA: Anatomical landmarks; B: Opening of the Kocher interval; C: Radiocapitellar joint exposed (radial head is marked with ).
*Open reduction and internal fixation A: Osteochondral fragment (white arrow, radial head is marked with ). B: Reduction and fixation with chondral darts (Arthrex®). C: Osteochondral fragment (white arrow).
At one-year post-operative follow-up, the patient remains asymptomatic, with a full range of motion and radiographic evidence of fracture consolidation. No complications have been reported (Figure 5).
Left elbow radiographs: one-year postoperative follow-upAnteroposterior and lateral views of the elbow.
Discussion
Capitellum fractures in the pediatric population represent a rare and frequently underdiagnosed entity, particularly in younger children, in whom a large portion of the distal humeral epiphysis remains cartilaginous, thereby limiting the diagnostic value of initial radiographic evaluation. As illustrated in our case, plain radiographs often fail to clearly demonstrate the fracture line, revealing only indirect signs such as a positive fat pad sign or small intra-articular fragments; this reinforces the need for a high index of clinical suspicion. This fracture pattern has been widely recognized in the literature and is included among TRASH lesions, as described by Waters et al. [1,9].
In recent years, multiple case reports and case series have emphasized CT scan and magnetic resonance imaging (MRI) as the most useful adjunctive imaging modalities to confirm the diagnosis and accurately characterize the fracture pattern in cases with a high index of suspicion [1,2,7,8]. In our hospital setting, a CT scan is particularly invaluable since it is more easily and readily available in the emergency department setting than an MRI. CT scans play an important role in fractures where the fragment is predominantly cartilaginous with a variable amount of subchondral bone, such as Kocher-Lorenz fractures [2,7,8].
In our patient, a Kocher-Lorenz fracture was identified, characterized by an osteochondral fragment with a thin layer of subchondral bone. This fracture pattern represents one of the most challenging lesions to detect on initial radiographic evaluation and to stabilize due to the limited amount of subchondral bone available for fixation. Regarding surgical technique, as reported in other recent studies, the preferred method is ORIF through a lateral approach using the Kocher interval, which allows adequate exposure of the capitellum while minimizing the risk of iatrogenic injury to neurovascular structures [1,8,10,12].
Regarding fixation methods, several options are available, including headless compression screws, absorbable Kirschner wires, and chondral darts [4,8,12]. Kang et al. retrospectively analyzed a cohort of 26 pediatric patients with Dubberley type IIA fractures and demonstrated that achieving stable fixation, whether using headless screws, absorbable wires, or compression darts, results in excellent functional outcomes with low complication rates and a rapid return to daily activities [13]. In our case, the use of bioabsorbable darts (Arthrex®) allowed for anatomical reduction and adequate stabilization of the fragment while avoiding the need for an additional surgical procedure for implant removal.
The postoperative evolution of our patient, characterized by complete fracture consolidation, full recovery of range of motion, and return to sports activities by the third postoperative month, is consistent with the outcomes reported in other studies. Late complications, such as stiffness or growth plate disturbances, are rare; even in Kocher-Lorenz fractures, traditionally associated with a higher risk of nonunion or fragment fragmentation, current literature supports that the prognosis is generally excellent when the diagnosis is made early and appropriate treatment with anatomical reduction is performed [4,8,10,11,14].
Conclusions
Capitellum fractures in the pediatric population are rare injuries and may be easily underdiagnosed. Our case report highlights the importance of maintaining a high index of clinical suspicion in the emergency department setting, particularly when initial radiographs are inconclusive. In such cases, additional imaging modalities, including CT scan and MRI, may be helpful in establishing the diagnosis.
In our experience, early surgical management with anatomical reduction and stable fixation was associated with excellent clinical and functional outcomes, even in a challenging fracture pattern such as a Kocher-Lorenz fracture. While larger studies are required to define standardized treatment guidelines, timely diagnosis and careful surgical technique remain important considerations in the management of pediatric capitellum fractures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shear fractures of the capitellum in children: a case report and narrative review Front Surg Pilotto JM Valisena S De Marco G 14075771120243902791710.3389/fsurg.2024.1407577 PMC 11254701 · doi ↗ · pubmed ↗
- 2Management and outcomes of capitellum fractures in adolescents: a case series and review of the literature Int J Surg Case Rep Zouirech Y Manni A Aqqaoui L Oubejja H Hosni S Ettayebi F 11129513120254027357610.1016/j.ijscr.2025.111295 PMC 12051655 · doi ↗ · pubmed ↗
- 3Type IV capitellum fractures in children BMJ Case Rep Papamerkouriou YM Tsoumpos P Tagaris G Christodoulou G 124201910.1136/bcr-2019-229957 PMC 668536831383681 · doi ↗ · pubmed ↗
- 4Management of pediatric capitellar fractures Univ Pennsylvania Orthop J Haghverdian JC Shah AS Arkader A 119125292019 https://www.upoj.org/wp-content/uploads/v 29/119_Haghverdian.pdf
- 5Posterolateral shear fracture of the capitellum associated with elbow dislocation in an adolescent: a case report SAS J Surg Zouirech Y Manni A Rouije B 629634102024
- 6Coronal shear fractures of the distal end of the humerus J Bone Joint Surg Am Mc Kee MD Jupiter JB Bamberger HB 4954781996855067910.2106/00004623-199601000-00007 · doi ↗ · pubmed ↗
- 7Articular shear fracture of the capitellum in a child: a case report J Orthop Case Rep Tajika T Hatori Y Kuboi T Saida R Chikuda H 545832024
- 8Chondral shear fracture of the capitellum in adolescents-a report of two late diagnosed cases and a review of literature Indian J Orthop Nagda TV Vaidya SV Pinto DA 4034075420203319411110.1007/s 43465-020-00197-1PMC 7609598 · doi ↗ · pubmed ↗