Nutrition rehabilitation programs and cachexia clinics for anorexia–cachexia syndrome in patients with cancer
Rony Dev, Kunal C Kadakia, Jegy M Tennison, Koji Amano, Michele Szafranski, Eduardo Bruera, Tateaki Naito, Egidio Del Fabbro

TL;DR
This paper discusses how specialized clinics and rehabilitation programs can help manage weight loss and poor nutrition in cancer patients with anorexia–cachexia syndrome.
Contribution
The paper emphasizes the need for interdisciplinary clinics to address the complex nature of anorexia–cachexia syndrome in cancer patients.
Findings
ACS is driven by complex metabolic and inflammatory mechanisms that cannot be reversed by standard nutrition alone.
Interdisciplinary teams are essential to manage nutrition impact symptoms and improve outcomes in ACS patients.
Specialized clinics can help integrate new treatments into the management of anorexia–cachexia syndrome.
Abstract
The anorexia–cachexia syndrome (ACS) is characterized by loss of appetite and unintentional weight loss. Important clinical outcomes are associated with ACS including increased risk of chemotherapy side effects, decreased survival, and quality of life. Because ACS is driven by complex metabolic mechanisms and a chronic pro-inflammatory response, the weight loss and muscle wasting cannot be reversed by conventional nutritional supplementation alone. However, insufficient intake of calories and protein exacerbate weight loss experienced by patients with ACS, while physical inactivity accelerate muscle wasting. In addition, uncontrolled symptoms, such as pain, mucositis, nausea, early satiety, and depression aggravate poor nutritional intake and are known as nutrition impact symptoms. Addressing these potentially reversible contributors to ACS requires an interdisciplinary team (IDT)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
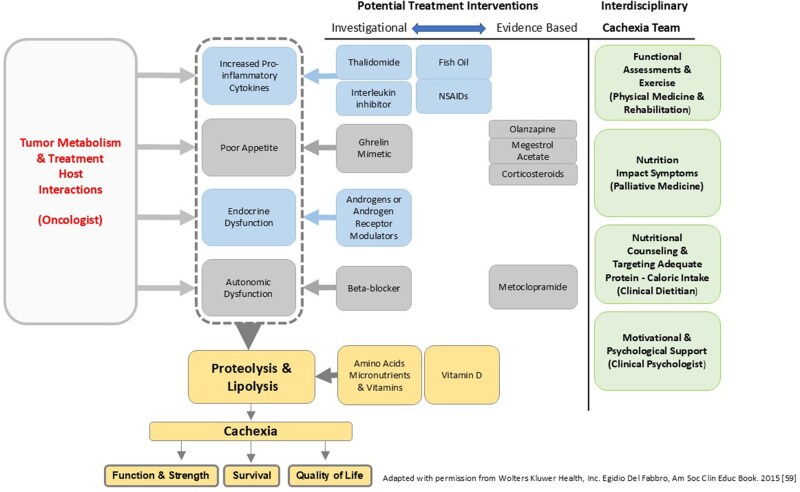 Figure 1
Figure 1| Author and year/intervention/aim(s) | Participants/setting | Outcome measures (time points) | Main findings and effects | Strengths/limitations |
|---|---|---|---|---|
|
| ||||
|
|
Outpatient clinic (Zurich, Switzerland) |
Symptoms: EORTC QLQ-C30 Functional: HGS, 30-second chair sit-to-stand test, 6MWT, 1 repetition maximum leg press, ECOG PS Nutrition: 3-day food diary, NRS-2002, bioelectrical impedance analysis Psychosocial: Nil Labs: Nil (Pre and at 3 and 6 months) |
Feasibility: Median adherence to the supervised exercise program was 75%, however, poor accrual led to early closure. Symptoms: No difference in global health status/quality of life was observed (change in EORTC QLQ-C30 was 4.5 ± 3.4 [intervention] vs 2.7 ± 4.0 [control], p = 0.72). Intervention arm had greater improvement in nausea and vomiting subscale. Functional: No statistical differences observed for any measure of physical performance. Nutrition: Intervention arm had greater protein intake but no difference in overall nutritional status by BIA or weight |
Strengths: Randomized trial of a combined nutrition and exercise program with multiple functional and nutritional endpoints. Confirmed feasibility of trial components in study population. Though no statistically significant differences, intervention group had numerical improvements in nearly all endpoints. Limitations: Poor accrual led to early closure and was under powered for primary endpoint (447 screened, 161 met inclusion, and 101 refused to participate). |
|
|
Outpatient clinic (Beijing, China) |
Symptoms: EORTC QLQ-C30, NCI-CTCAE 4.0 Functional: HGS, 30-second chair sit-to-stand test, 6MWT, 1 repetition maximum leg press, ECOG PS Nutrition: NRS-2002, PG-SGA Psychosocial: DT, HADS-A, HADS-D, PHQ-9 Labs: Nil (pre and throughout study period) |
Primary endpoint: Median overall survival was improved with ESC than usual care, 14.8 (95% CI 13.3-16.3) vs 11.9 (9.6-13.6) months, Symptoms: From baseline to week 9, ESC group had a significant improvement in emotional and cognitive functioning. Nutrition: From baseline to week 9, ESC group had a significant improvement in NRS 2002 and PG-SGA scores. Less patients had weight loss in ESC grout (45vs 58%, Psychosocial: From baseline to week 9, ESC group had a significant improvement in DT, HADS-A, HADS-D, and PHQ-9. |
Strengths: Primary endpoint was overall survival. Large randomized controlled trial in homogenous advanced cancer population. A simple ESC model for further study Limitations: Limited external validity as conducted at single intuition in China. Not blinded. Moderate drop-out in both nutrition (33%) and psychological (28%) interventions over 9-week study period. |
|
| ||||
|
|
Outpatient clinic (Pennsylvania, USA) |
Symptoms: ESAS Functional: KPS Nutrition: Weight, body cell mass, caloric goal Psychosocial: Nil Labs: CBC, renal/liver function, albumin, pre-albumin, testosterone level, and Vitamin D (Pre and Post) |
Feasibility: “Overall, most patients felt that the CARE Clinic was a worthwhile experience and all patients said they would recommend the clinic to a friend” Nutrition and Symptoms (no data provided): “Although not statistically significant, a trend for improvement was observed between visit 1 and visit 4 (12 weeks) in weight, body cell mass, and appetite levels” |
Strengths: Comprehensive description of the interdisciplinary assessment and treatment goals conducted by the medical, nursing, nutrition, physical therapy, and speech and swallowing teams. Limitations: Small sample size of the evaluable population ( |
|
|
Outpatient clinic, (Montreal, Canada) |
Symptoms: ESAS, BFI Functional: 6MWT Nutrition: PG-SGA Psychosocial: DT Lab: Nil (Pre and Post) |
Symptoms: Improvements in ESAS of appetite, strength, nervousness, depression, pain, constipation, and nausea (all Functional: Median 6MWT (range) improved from 384 m (173-570) to 435 m (203-630), Nutrition: Median PG-SGA (range) improved from 12 (2-24) to 9 (1-18) Psychosocial: Median DT (range) improved from 4 (1-7) to 2 (0-6), |
Strengths: Single cancer type. Use of validated tools. Limitations: High dropout rate (58%) due to disease progression and inability to attend regularly. No control group. |
|
|
Outpatient clinic (Sydney, Australia) |
Symptoms: ESAS Functional: KPS, 6MWT, HGS Nutrition: PG-SGA, Body composition analysis Psychosocial: Nil Labs: Albumin, CRP (Pre and at 1, 2, 3, and 6 months) | Feasibility: 68%, 58%, 44%, and 12% compliance at 1, 2, 3, and 6 months. >90% patient reported CNRP as important. Likelihood for returning at the 2-month follow-up were higher 6MWT, lower ESAS score, active anticancer therapy, better KPS, less weight loss, male gender, low CRP, low GPS, low PG-SGA, and higher albumin |
Strengths: Provided predictors of compliance to a CNRP program at a high-volume cancer center Limitations: No formal statistical testing on effect of CNRP on outcomes. Despite collection of body composition data, no data provided of CNRP effect on body composition. No control group. |
|
|
Outpatient clinic (Ottawa, Canada) |
Symptoms: ESAS, MFI Functional: ECOG PS, MDASI-Impact on Function Subscale, Berg Balance Scale, Functional Reach Test, Timed Up and Go, HGS, 6MWT Nutrition: PG-SGA Psychosocial: Nil Labs: CBC, electrolytes, CRP, albumin, TSH, glucose, and LDH (pre and post) |
Feasibility: 58% completed the 8-week program. Reasons for non-completion included disease progression, personal, death, or too well. Likelihood to completing program was higher if baseline CRP <10. Symptoms: Moderate-to-large effects were observed in anxiety, depression, overall well-being, feeling tired, and fatigue (effect size = 0.38-0.55) Functional: Improvement in 6MWT (effect size = 0.80), Time up and Go (effect size =0.65), and Functional Reach Test (effect size = 0.44). No statistical difference in Berg Balance scale or HGS. ECOG PS improved (effect size = 0.9) Nutrition: Significant improvement in overall nutritional risk (effect size = 0.46). |
Strengths: Exhaustive use of validated functional assessments. Limitations: No results on weight change. No control group. |
|
|
Outpatient clinic (Montreal, Canada) |
Symptoms: ESAS, MFI Functional: 6MWT and 5-m Walk Test, ECOG PS Nutrition: Weight history Psychosocial: DT and CT Labs: CRP, albumin (pre and post) |
Feasibility: 70% completed the 10-12-week CNR. Reasons for non-completion included disease progression, dropped out, and death. Likelihood of non-completion was higher if baseline ECOG PS was poor, elevated CRP >20, poor nutritional status, and worse anorexia. Symptoms: Moderate reduction in weakness, depression, nervousness, and shortness of breath as well as reduced activity, physical and general fatigue (effect sizes = 0.5-1.1). Functional: Mean 6MWT at baseline was 395 ± 111 m, increased by 41 m (95% CI, 29-52, effect size, 0.7). Maximal gait speed at baseline was 1.5 ± 0.44 m/s, increased by 0.15 m/s (95% CI, 0.09-0.21, effect size, 0.6). Nutrition: 77% gained or maintained weight. Psychosocial: Moderate reduction in distress and coping (effect sizes = 0.5-0.7) |
Strengths: Large multi-year experience with high program completion rates. Detailed description of interventions provided by each cancer nutrition-rehabilitation health professional (Physician, RN, Dietician, OT) Limitations: No long-term results. No control group. |
|
|
Outpatient clinic (Ottawa, Canada) |
Symptoms: Nil Functional: 6MWT Nutrition: Nil Psychosocial: GSE, HADS Labs: CRP (pre and post) |
Functional: Mean 6MWT at baseline was 372.55 m ( Psychosocial: Self-efficacy (GSE) significantly increased from 27.86 ( Lab: Inflammation, as measured by CRP, did not significantly change. |
Strengths: Analyzed pre-specified factors felt to be contribute to depression and observed self-efficacy as largest contributor. Limitations: No nutritional data. No control group. |
|
| ||||
|
|
Outpatient clinic (Texas, USA) |
Symptoms: ESAS and S-NIS Functional: Nil Nutrition: PG-SGA and bedside indirect calorimetry Psychosocial: Nil Labs: Vitamin B12, TSH, total testosterone, and serum cortisol at baseline. (Pre and at follow-up) |
Symptoms: Median S-NIS was 3 and 15% experienced ≥5 S-NIS (most commonly, early satiety, constipation, N/V, and mood changes). Most common interventions were metoclopramide, laxatives, antidepressants, and zinc. Nutrition: Significant improvements of appetite between visits with 34% gaining weight. 42% were hypermetabolic as measured by indirect calorimetry. Labs: Adrenal insufficiency, hypothyroidism, and B12 deficiency were infrequently observed, however, hypogonadism was present in 73% of men. |
Strengths: Detailed description of secondary nutritional impact symptoms and corresponding intervention Limitations: Moderate drop out (39%) due to death or hospice, severe symptoms, noncompliance, or residence out of state. No functional evaluation. No control group |
|
|
Outpatient clinic (Montreal, Canada) |
Symptoms: ESAS Functional: MDASI-Impact on Function Subscale, 6MWT Nutrition: Body weight and presence of PEG feeding tube Psychosocial: DT Lab: Nil (pre and post) |
Symptoms: Improvement in pain, quality of life, weakness, shortness of breath, anorexia, insomnia, depression (effect sizes = 0.6-0.9) Functional: No significant effect on MDASI-Function Subscale. Mean 6MWT at baseline was 421 ± 99 m, increased by 59 m (95% CI, 27-91, effect size, 0.8). Nutrition: 78% either gained or maintained weight. Of 11 patients who needed PEG feeding, 8 continued at end of program. Psychosocial: Mean change in DT (95% CI) improved 1.6 (0.7-2.5), effect size = 0.7. |
Strengths: Single cancer type. Detailed description of interventions provided by each cancer nutrition-rehabilitation health professional (physician, RN, dietician, OT) Limitations: Minimal objective assessment of nutritional status. Although taste/smell alterations and xerostomia were collected at baseline, not collected at follow-up. No control group. |
|
|
Outpatient clinic (Montreal, Canada) |
Symptoms: FAACT Functional: 6MWT, ECOG PS Nutrition: Weight history Psychosocial: Nil Labs: CRP, albumin (pre and post) |
Feasibility: 42% of the original cohort remained at the third visit. Likelihood for completion of 3 visits was non-lung cancer type, lower baseline CRP, and better baseline quality of life scores. Symptoms: Statistically significant improvements in FAACT total and specific subscales (physical well-being, anorexia-cachexia. No difference in emotional or social well-being subscales. Functional: Patients who increased 6MWT had greatest improvements in quality of life. Nutrition: Patients who gained weight had greatest improvements in quality of life. Labs: Baseline CRP was not associated with quality of life. |
Strengths: Large cohort to identify characteristics associated with quality-of-life improvement during a multimodal rehabilitation program for cancer cachexia. Limitations: No specific details on change in functional and nutritional provided (only correlations with quality-of-life survey was provider). No control group |
|
|
Outpatient clinic (Victoria, Australia) |
Symptoms: Nil Functional: HGS, 30-second chair sit-to-stand test Nutrition: Weights Psychosocial: Nil Labs: CRP, albumin, hemoglobin, testosterone |
Feasibility: 236 patients referred, 61 excluded from analysis primarily due to insufficient data and nonattendance. Of the 175 patients, 46% referred by oncologist, 39% by local medical office, and 11% from palliative care professional with median time-to-referral from initial cancer diagnosis of 12.9 months (0.4-304 months). 42% did not return for follow-up with most common reasons being death. Functional: 4% had increase in HGS and 38% had increase in Sit-to-Stand score. Nutrition: 78% had stabilization and 31% increased weight. Labs: 29% had increase in albumin. |
Strengths: Detailed description of pharmacologic interventions provided by palliative care physician. Limitations: Nutritional and functional results are biased by significant attrition of participants. Labs changes beyond albumin not provided. No control group |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutrition and Health in Aging · Therapeutic Uses of Natural Elements · Vitamin C and Antioxidants Research
Introduction
The anorexia–cachexia syndrome (ACS) is characterized by loss of appetite and unintentional weight loss and is associated with increased risk of chemotherapy side-effects, poor survival, diminished function, and decreased quality of life (QOL).1 Because ACS is driven by complex metabolic alterations and a chronic pro-inflammatory response, the weight loss and muscle wasting cannot be reversed by conventional nutritional supplementation alone. However, insufficient intake of calories and protein may exacerbate the weight loss experienced by patients with ACS.
Improving nutrition intake is possible by addressing symptoms that contribute to anorexia and muscle wasting. Symptoms commonly encountered in patients with cancer, such as nausea, depressed mood, early satiety, or pain, may decrease oral intake and are referred to as nutrition impact symptoms (NIS). The ASCO guidelines for cancer cachexia support the concept of addressing NIS, stating “uncontrolled symptoms of cancer or its treatments” “can be detrimental to food intake.”1 By improving nutritional intake and promoting physical activity, the muscle wasting, and adverse outcomes associated with ACS may be mitigated.
Although managing NIS is a key component, other factors such as physical inactivity, eating-related conflict between patients and family members or inadequate access to high-quality nutrition may play an important role in exacerbating ACS. Additional non-symptom barriers can also impede dietary intake (even after nutritional counselling), such as conflicting advice and personal food restrictions.2 Managing these potentially reversible clinical and psychosocial domains requires a collaborative, interdisciplinary team (IDT) involving physicians, nurses, dietitians, physical therapists, and clinical psychologists. This multimodal approach to ACS is especially important given current ASCO guidelines are unable to recommend a specific pharmacological intervention for cachexia as standard of care.
The primary aim of this narrative review is to provide an overview of pragmatic strategies for managing ACS, such as exercise and nutrition, malnutrition screening, and the assessment of NIS and other contributors and treatment opportunities. In addition, research on nutrition rehabilitation programs and cachexia clinics will be summarized.
Assessments
In patients with cancer, the ideal assessments for ACS include malnutrition screening and measuring protein and caloric intake, monitoring weight, body composition and performance status (PS), and assessing NIS.3 The feasibility of completing all these assessments depends on institutional support and team resources.
Malnutrition screening
Several validated4 screening tools are available for malnutrition in patients with cancer, including the Patient-Generated Subjective Global Assessment Short Form (PG-SGA SF),5 Malnutrition Screening Tool,6 and the Malnutrition Universal Screening Tool (MUST).7 There is no consensus on the best tool for screening, since each tool has merit but also some limitations.8 The PG-SGA SF for example, has predictive value for survival, and can be used as a screening, assessment or monitoring instrument. However, the PG-SGA-SF does not include an assessment of body mass index (BMI), a simple, yet important measure that should be done at each visit. The initial BMI and the rate of weight loss predict survival in patients with solid tumors independently of conventional factors such as cancer site, stage, and PS.9 Additional measures of anorexia severity may be useful to measure longitudinally—these include an appetite score of ≥3/10 on the Edmonton Symptom Assessment System (ESAS) or ≤37 on the Anorexia/Cachexia Subscale of the Functional Assessment of Anorexia/Cachexia Therapy (FAACT-A/CS).4
Nutrition impact symptoms
Studies of patients across various tumor types and treatments show individual NIS and/or their aggregate number are associated with adverse clinical outcomes. While the treatment of an individual NIS may not reverse weight loss or modulate the mechanisms driving ACS, managing NIS may slow wasting and improve QOL.
More severe anorexia is associated with greater weight loss, poorer performance status and higher prevalence of NIS such as early satiety, constipation, and vomiting.10 A systematic review of 30 anti-neoplastic treatment trials found more severe anorexia or pain scores at baseline were associated with decreased survival.11 A multi-center study from Japan reported taste and smell disturbances were associated with worse dietary intake and QOL scores, independent of performance status and degree of ACS.12 A cross-sectional study of outpatients at high risk for malnutrition showed the combination of anorexia and early satiety compared to anorexia alone was associated with significantly worse weight loss, worse overall health perception, and fatigue.13 In surgical patients with cancer, the number of NIS is associated with higher prevalence of malnutrition,14 and a longitudinal study of patients with esophageal cancer found more NIS were associated with worse QOL and physical function at 6 months after surgery, regardless of the pre-operative BMI or post-operative weight loss.15 Similarly, aggregate burden of symptoms prior to radiation and/or chemotherapy was a significant independent predictor of reduced intake, weight loss, and survival in patients with head and neck cancer.16
Constipation is common in patients receiving opioids or ondansetron and underappreciated as a NIS. In patients with early-stage head and neck cancer receiving radiation therapy, constipation was associated with significantly greater weight loss,17 while a prospective study of patients with newly diagnosed esophageal cancer found symptoms of anorexia and constipation at the start of chemoradiation persisted 4-6 weeks after completion of therapy. Long-term survivors are also at risk of adverse effects that correlate with NIS burden. In a population-based prospective study found symptoms of pain, fatigue, nausea and vomiting, and appetite loss were associated with a > 15% weight loss 5 years after surgery for esophageal cancer.18
Assessment
Brief (<5 minutes) questionnaires to assess NIS include the PG-SGA SF and the ESAS. ESAS has the advantage of providing a numeric rating scale (0-10) for individual symptoms but evaluates fewer ACS symptoms than the PG-SGA SF. A questionnaire derived from both ESAS and PG-SGA evaluated NIS and eating-related distress in Japanese patients with advanced cancer and their families. Patients with ACS had significantly increased eating-related distress, tiredness, drowsiness, lack of appetite, early satiety, diarrhea, abnormal taste, and difficulty swallowing compared to patients without ACS.19^,^20
Management
Few studies characterize the medical management of individual NIS in patients with cancer. Some medications may be effective for multiple symptoms, for example, duloxetine (neuropathic pain + depression), mirtazapine (depression + non-CINV nausea), and olanzapine (CINV and non-CINV nausea + resistant depression).21 Observational studies indicate that prokinetic metoclopramide may be useful for early satiety/gastroparesis and non-CINV. An early study using the PG-SGA identified multiple unmanaged symptoms in patients with cancer, including loss of appetite, nausea, early satiety, dry mouth, and altered taste, which resulted in the incorporation of dietary counseling, prescriptions for artificial saliva, and the addition of metoclopramide.22 Laxatives and metoclopramide were the most common medications used in 151 patients with advanced cancer seen by the MD Anderson Cancer Cachexia Clinic.23 Notably, conventional appetite stimulants such as corticosteroids or megestrol acetate were not prescribed, yet one third of patients experienced weight gain.
Body composition
Body composition (lean mass and fat mass) assessments may be useful for diagnosis, prognosis and for monitoring the efficacy of interventions. Decreased muscle mass (sarcopenia) is associated with a poor prognosis in patients with solid tumors and highly prevalent in patients admitted to the ICU with hematological malignancies.24 The combination of reduced lean body mass and excess adiposity (sarcopenic obesity) is associated with a particularly poor prognosis in patients with solid tumors and is difficult to identify without imaging.25 Computed tomography scans offer an accurate, opportunistic evaluation of body composition at diagnosis or re-staging. However, dual-energy-x-ray absorptiometry (DXA) is still considered the gold standard, although lower-cost evaluations with bio-electrical impedance analysis (BIA) and anthropometrics may be more practical for routine clinical use. DXA is most accurate, but multi-frequency BIA is a convenient, relatively lower-cost body composition assessment tool that can be used longitudinally to measure fat-free mass and fat mass.26
Laboratory tests
A limited set of labs should be considered based on clinical history and possible co-morbid conditions contributing to wasting including C-reactive protein, albumin, vitamin B12 and D, thyroid function, and testosterone.
Physical performance
Muscle wasting and a decline in muscle quality and performance are features of most patients with ACS. A systematic review27 of functional assessments in cachexia trials included 5 objective outcomes: Hand grip strength (HGS), stair climb power, timed up and go test, 6-minute walking test, Short Physical Performance Battery (SPPB) and chair stand test (time needed to rise 5 times from a seated position without a patient using their arms). HGS (with a dynamometer) was the most used physical function endpoint; however, the authors could not comment on which tool was optimal. In older patients with cancer, higher symptom burden is associated with functional impairment. For example, in 359 patients (median age 81 years), each unit increase in a composite symptom score was associated with greater activity of daily living impairment, physical activity limitations, falls, and SPPB ≤9 (P < .05).28 The SPPB is predictive of clinical outcomes, including mortality and health care utilization and includes a composite test of gait speed, balance, and a chair stand test (approximately 10 minutes to complete). A SPPB ≤9 score is predictive of decreased overall survival in older patients with leukemia,29 increased mortality in older women with gynecological cancer,30 and lower chemotherapy completion in non-small cell lung cancer.31
Patient and caregiver distress
Physical signs of wasting and loss of appetite can lead to conflict among patient and family over caloric and food intake, body image dissatisfaction, and existential distress or anticipatory grief.32 Family caregivers’ eating-related distress may be greater than patient eating-related distress.33 A qualitative study involving 31 patient-spouse/partner dyads using semi-structured interviews found interactions between patient and family caregivers can either sustain or ameliorate eating-related distress.34 A recent scoping review found 3 ways a psychosocial component of multimodal management could help patients with ACS. These include behavioral counseling to promote treatment adherence, adaptive coping to emotional stress, and managing anxiety and depression.35
Key components of nutrition rehabilitation programs and cachexia clinics
Nutrition rehabilitation programs and cachexia clinics should ideally incorporate key components of nutritional counseling, exercise, pharmacological interventions, and psychosocial support. The team composition may vary depending on resources; however, a dietitian is usually a core member of the IDT. The inclusion of physical therapists and psychologists with expertise in oncology is desirable.36 A single visit with a multidisciplinary team would be preferable, so as not to place an undue burden on patients. If interdisciplinary members are not “embedded” within the clinic, patients could be seen in tandem.
The composition and leadership of the IDT will depend on institutional resources and strengths, coupled with patient needs. For example, patients with high symptom burden and advanced disease would benefit from a palliative medicine specialist with expertise in symptom management and opioid use, while an older patient may best be served by a team with expertise in aging (eg, Geriatric oncology or Endocrinology). Nutritional rehabilitation programs may serve a broader patient population than cachexia clinics, by including patients preparing for surgery with “prehabilitation” programs and long-term survivors of serious illness who may have completed disease directed therapy. Integration of clinics within an already established supportive/palliative care centers, rehabilitation medicine clinics, subspecialty oncology program, or a collaborative effort within specific cancer types at greater risk for cachexia can potentially provide more rapid access, streamline referrals, and identify motivated patients who can adhere to multi-modality treatment interventions.
Challenges
Despite promising data and an intuitive appreciation of nutrition and exercise health benefits, challenges remain in establishing and sustaining cachexia clinics and nutrition rehabilitation programs. Early inclusion of dietitians, physiotherapists and psychologists during the planning and pilot phase should be considered to reinforce shared vision and goals for the specialty clinic and provide consistency of information and treatment recommendations. Educating colleagues about the impact of ACS on functional outcomes and adopting screening tools for malnutrition and ACS to facilitate referral to specialty clinics is necessary. An international survey of healthcare professionals noted only 29.1% recognized >5% weight loss from baseline as a key criterion for cancer cachexia, and only 47.4% reported weighing patients at each visit.37 Care pathways adopting simple referral criteria that include weight loss (eg, ≥ 5% within past 6 months or ≥2.5% in patients with BMI < 20) or symptoms (ESAS appetite score ≥3) or PG-SGA SF scores ≤37 may increase awareness among clinicians and encourage referrals. A Japanese survey found healthcare professional did not regularly provide education and emotional support to either patients suffering from cancer cachexia or their families.38 These studies highlight the need for more education regarding assessment and treatment of ACS and the need for specialty clinics. However, the burden of clinic evaluations, such as patient-reported outcomes, body composition, diet intake diaries, and functional assessments, should not overwhelm patients.
Nutrition rehabilitation and cachexia clinics in cancer centers
Cachexia clinics and combined exercise and nutrition rehabilitation programs have been established within outpatient oncology centers for over a decade. The goals of these programs are to focus on the complex needs of patients with cancer who have ACS with a systematic multimodal approach utilizing an IDT. Table 1 provides an overview of 12 published studies combining nutrition + exercise along with medications (either targeting NIS or selected mechanisms of ACS). Some of the studies are from nutritional rehabilitation programs or cachexia clinics. Their design, number of participants, methods, outcome measured, and main findings are outlined. Retrospective (n = 4) and non-randomized prospective (n = 6) studies evaluating the impact of these specialty clinics suggest variable benefits in improved symptom control,23^,^39–44 increased functional capacity,39–41^,^42^,^44^,^45 enhanced nutritional status,23^,^39–44 and less psychosocial distress.39^,^41^,^42^,^45
Evidence for combined interventions
While prospective randomized controlled trials (RCTs) on the impact of cachexia clinics and nutrition rehabilitation programs are limited, a few trials have tested the effects of a combined nutrition and physical exercise interventions.46^,^47 A systematic review examined the effect of exercise and nutritional interventions on body composition in patients with advanced or metastatic cancer (*n *= 8). The authors concluded that both intervention approaches preserve lean mass, while only combined interventions may lead to alterations in fat mass.48 No RCTs include NIS in their multimodal treatment; however, 2 components of the multimodal approach (dietitian and psychologist) were used to compare early interdisciplinary supportive care (ESC) vs usual care in 328 patients with metastatic esophagogastric cancer.47 Nutritional risk screening included the PG-SGA and interventions were daily targets of 20 kcal-30kcal/kg, daily protein intake at 1 g-1.5 g/kg of body weight, and enteral or parenteral nutrition as indicated. Psychologists conducted depression and anxiety screening and provided individual and family psychotherapy. ESC vs usual care showed improved overall survival and better PG-SGA and depression scores, and fewer patients had weight loss.
Additional studies are worth noting. A RCT determining the effect of multimodal prehabilitation vs postoperative rehabilitation for Frail Patients Undergoing Resection of Colorectal Cancer found no benefit in the Prehabilitation group despite a personalized, supervised, and home-based multimodal program prescribed by a kinesiologist, a nutritionist, and a psychology-trained nurse. The authors speculate that the limited duration of the intervention (4-5 weeks) may be one reason for the result.49 Another preliminary study of early prehabilitation in patients with lung cancer demonstrated feasibility and incorporates a palliative medicine physician plus registered dietitian and rehabilitation physiotherapist into the IDT.50
Two preliminary trials in patients with advanced cancer, from Japan (single arm)51 and the United Kingdom (randomized)52 using a combination of exercise and nutritional support reported feasibility and improved outcomes. A guideline-directed, physician-led Cancer Nutrition Program at a Comprehensive cancer center in France, improved clinical outcomes and decreased costs in patients with advanced cancer. Over a 3-year period, the investment in developing a team that included cancer-specific training of dieticians, decreased the number of patients receiving parenteral nutrition from 157 to 67, significantly increased the enteral/parenteral patient ratio, and reduced costs for nutritional care by 54%.53
Future directions
Trials combining exercise and nutrition plus an agent targeting one of the mechanisms of ACS, for example, NSAID for inflammation, have demonstrated feasibility and safety (Figure 1).54 Trials underway include a Korean RCT comparing multimodal intervention care (MIC) vs conventional palliative care. MIC includes ibuprofen, omega-3-fatty acid, oral nutritional supplement, weekly physical, psychiatric assessment, nutritional counseling, and complementary and alternative medicine.55 More trials evaluating anti-cachexia agents in combination with a multimodal approach are needed.56 Individualizing management of patients based on their symptom burden, function, pathophysiological drivers of cachexia, and cancer stage should be the aspirational model of care.
Multi-modality treatment for anorexia-cachexia syndrome in patients with cancer.
Conclusion
ACS in patients with cancer is associated with increased physical and psychological symptom burden, loss of function, decreased QOL, and increased morbidity and mortality. To effectively treat ACS in patients with cancer, providers need to screen for malnutrition, evaluate body composition and functional status, and provide a thorough assessment and treatment of NIS. Given that multi-modality treatment is necessary to address all the clinical domains of ACS, the development of specialty clinics is desirable in cancer centers with adequate resources and expertise in treating ACS obtained from these pilot programs may be disseminated to other healthcare providers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roeland EJ , Bohlke K, Baracos VE, et al Management of cancer cachexia: ASCO guideline. J Clin Oncol. 2020;38:2438-2453. 10.1200/JCO.20.0061132432946 · doi ↗ · pubmed ↗
- 2Nasrah R , Van Der Borch C, Kanbalian M, Jagoe RT. Defining barriers to implementation of nutritional advice in patients with cachexia. J Cachexia Sarcopenia Muscle. 2020;11:69-78. https://doi: 10.1002/jcsm.1249031436033 10.1002/jcsm.12490 PMC 7015253 · doi ↗ · pubmed ↗
- 3Dev R. Measuring cachexia-diagnostic criteria. Ann Palliat Med. 2019;8:24-32. 10.21037/apm.2018.08.0730525765 · doi ↗ · pubmed ↗
- 4Blauwhoff-Buskermolen S , Ruijgrok C, Ostelo RW, et al The assessment of anorexia in patients with cancer: cut-off values for the FAACT-A/CS and the VAS for appetite. Support Care Cancer. 2016;24:661-666. https://doi: 10.1007/s 00520-015-2826-226160463 10.1007/s 00520-015-2826-2PMC 4689771 · doi ↗ · pubmed ↗
- 5Bauer J , Capra S, Ferguson M. Use of the scored patient-generated subjective global assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr. 2002;56:779-785. 10.1016/j.clnesp.2022.09.02912122555 · doi ↗ · pubmed ↗
- 6Paur I , Smedshaug GB, Haugum B, et al The Norwegian Directorate of health recommends malnutrition screening tool (MST) for all adults. Clin Nutr ESPEN. 2022;52:28-31. https://doi: 10.1016/j.clnesp.2022.09.02936513467 10.1016/j.clnesp.2022.09.029 · doi ↗ · pubmed ↗
- 7Boleo-Tome C , Chaves M, Monterio-Grillo I, et al Teaching nutrition integration: MUST screening in cancer. Oncologist. 2011;16:239-245. 10.1634/theoncologist.2010-020321273515 PMC 3228088 · doi ↗ · pubmed ↗
- 8Molfino A , Imbimbo G, Laviano A. Current screening methods for the risk or presence of malnutrition in cancer patients. Cancer Manag Res. 2022;14:561-567. https://doi: 10.2147/CMAR.S 29410535210853 10.2147/CMAR.S 294105 PMC 8857947 · doi ↗ · pubmed ↗