Population reach, feasibility and acceptability of digital therapeutics for smoking cessation among people living with HIV: Results of the Quitting Matters pilot trial
R. Vilardaga, F.J. McClernon, O. Akingbule, P. Mannelli, S.M. Thomas, J.M. Davis, M.F. Gray, C. Arnold, I. Chow Kai Reyes, R. Ashare, M. Paukner, L.R. Pacek

TL;DR
A digital smoking cessation tool tailored for people living with HIV showed higher engagement and promising outcomes compared to a standard tool in a pilot trial.
Contribution
The study introduces and evaluates a novel digital therapeutic (LTQ-H) tailored for people living with HIV.
Findings
LTQ-H users had significantly more device interactions and engagement with smoking cessation content compared to QuitGuide users.
Despite higher baseline challenges (e.g., cannabis use), LTQ-H showed numerically better cessation outcomes at week 12.
The study suggests LTQ-H has potential for population reach and engagement in smoking cessation for people with HIV.
Abstract
Tobacco use is disproportionately prevalent among people living with HIV (PWH) and is a significant contributor to morbidity and mortality in this population. Reaching communities of PWH to facilitate smoking cessation is challenging. Digital Therapeutics (DTx) can facilitate widespread implementation and adoption of smoking cessation treatments for PWH. We compared the feasibility and acceptability (primary outcomes) and preliminary efficacy (secondary outcome) of a DTx tailored to PWH – Learn to Quit-HIV (LTQ-H) – versus a gold standard smoking cessation DTx (QuitGuide) in a remote pilot randomized controlled trial. All participants received nicotine replacement therapy and were assessed at weeks 4, 8, and 12. During a 13-month period, we remotely recruited a sample of PWH (n = 41) across the United States, with randomization leading to a higher proportion of LTQ-H users with high…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
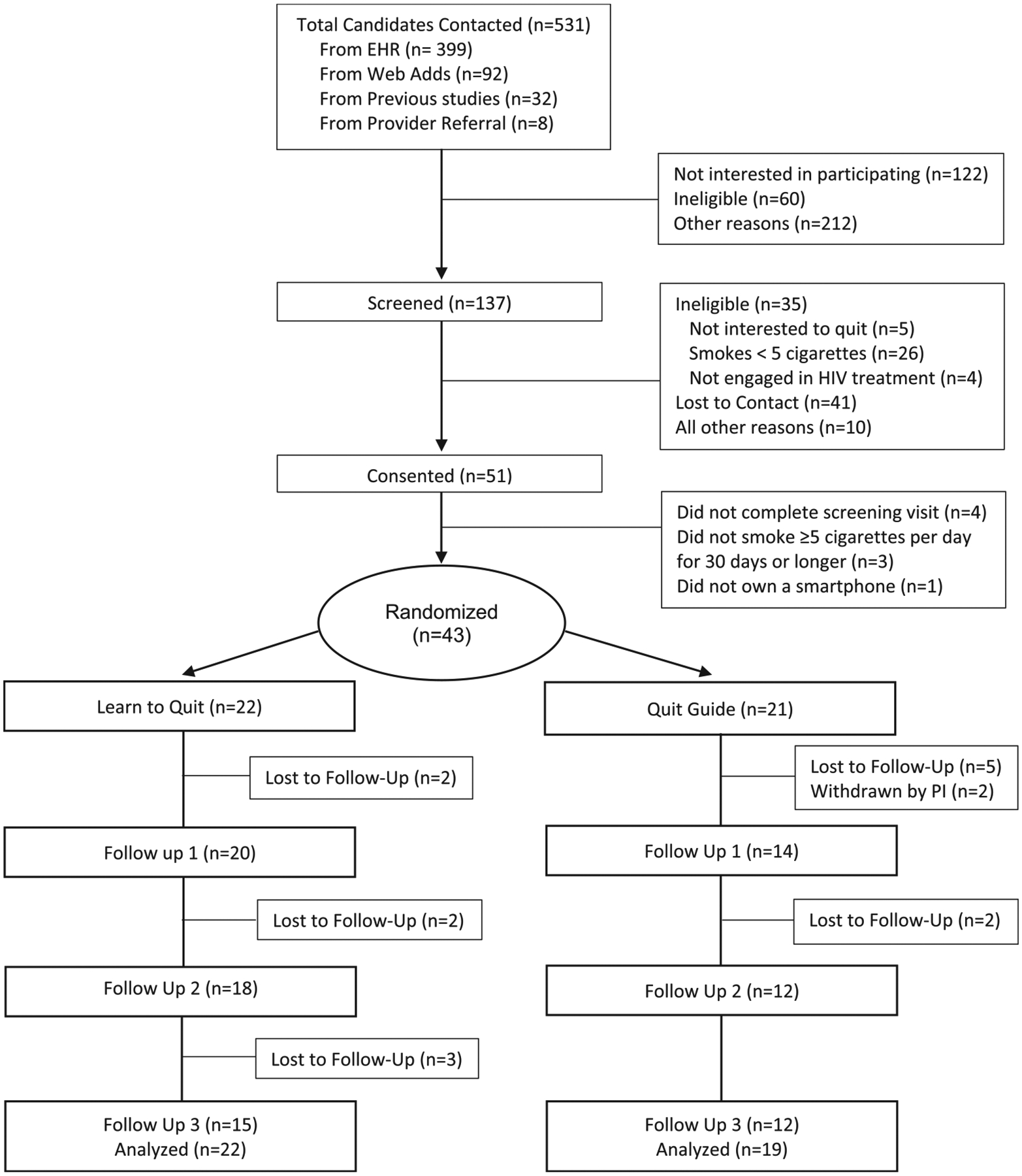 Figure 1
Figure 1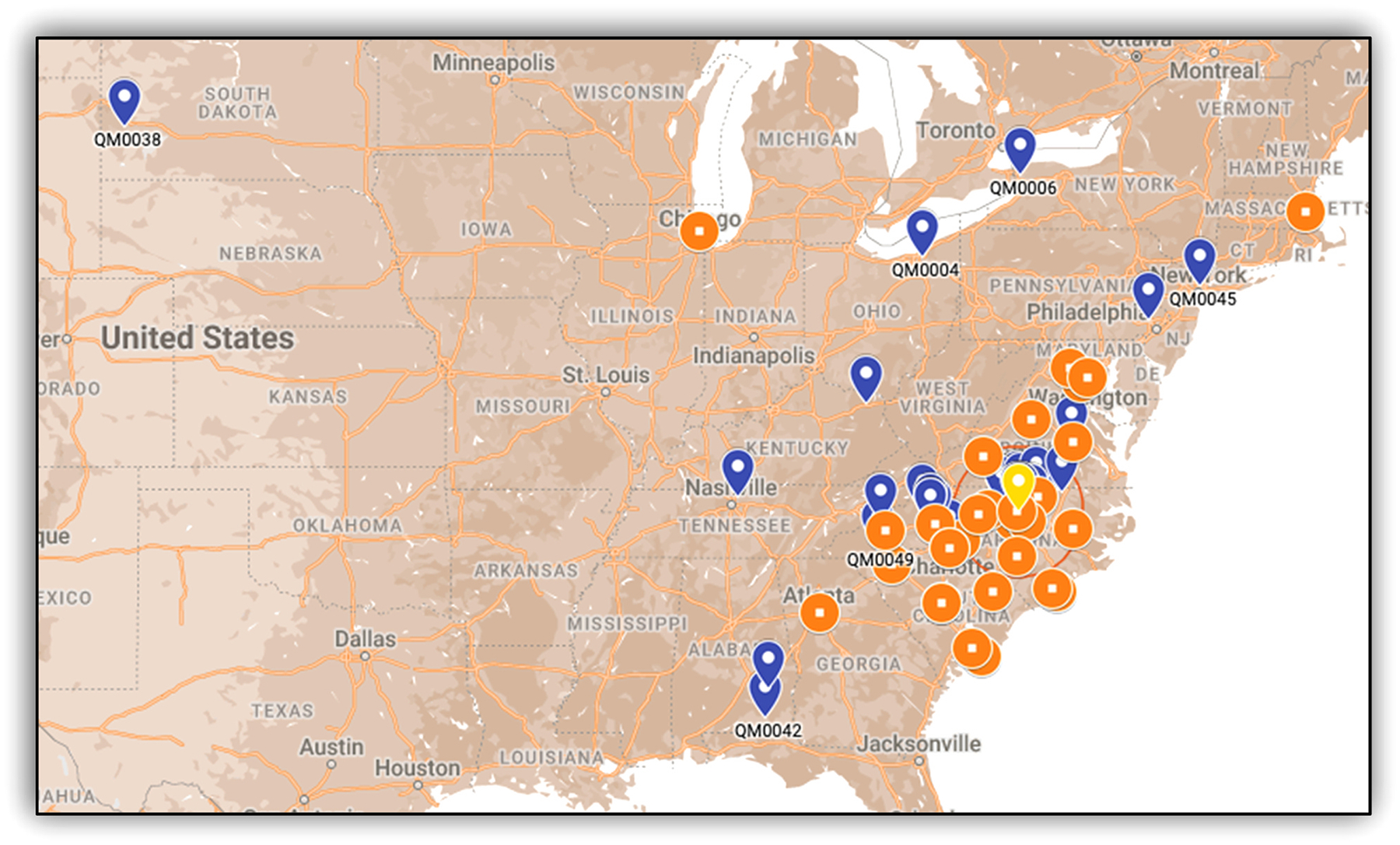 Figure 2
Figure 2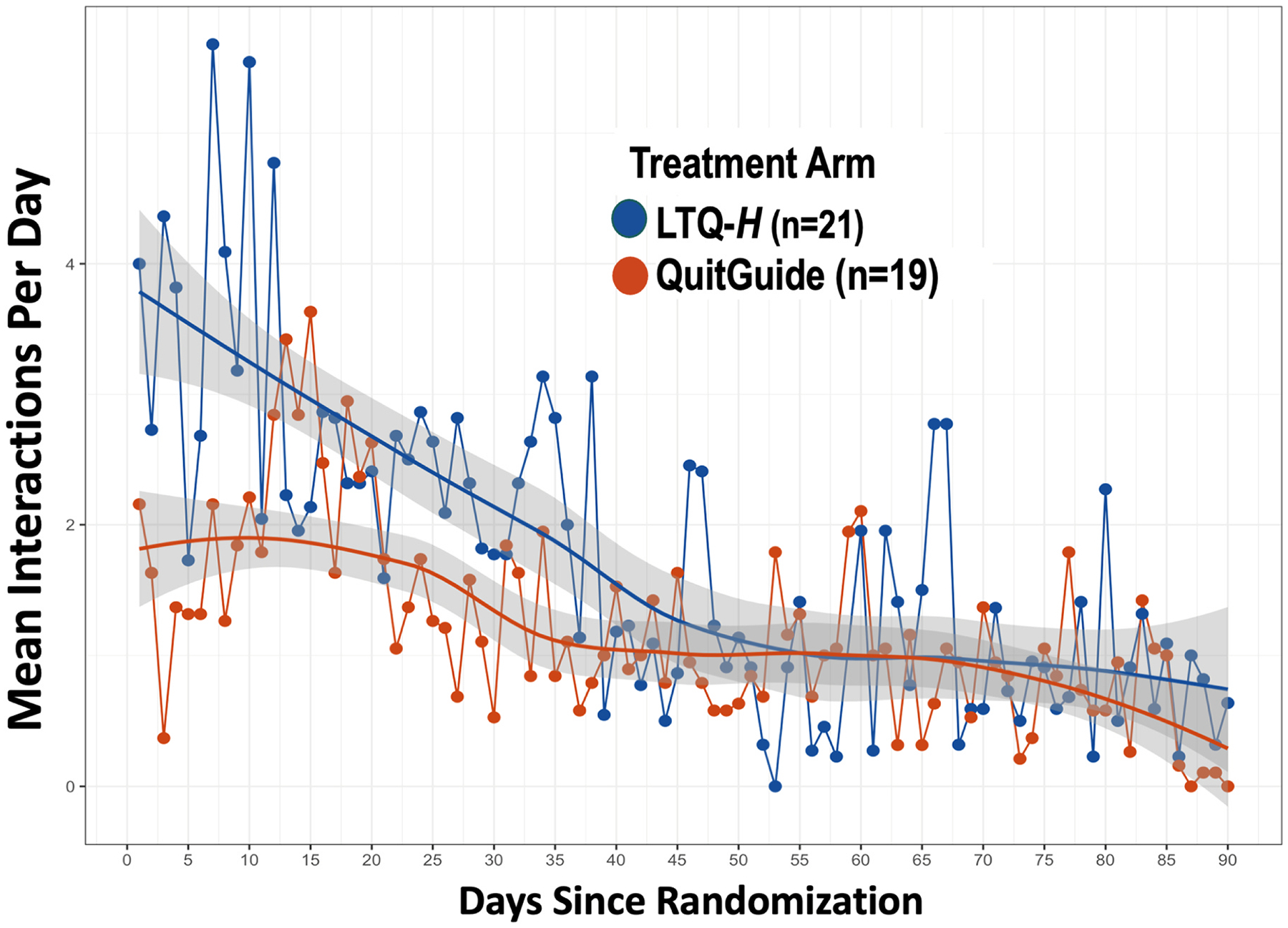 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSmoking Behavior and Cessation · Focus Groups and Qualitative Methods · Diabetes Management and Education
Introduction
The prevalence of cigarette smoking among people living with HIV (PWH) is disproportionately high (47 %) (Asfar et al., 2021) compared to the United States (U.S.) general population (11.5 % in 2021) (Cornelius, 2023). Due to the development of highly effective treatments for HIV and the resulting increased longevity, smoking among PWH is now a greater cause of mortality than HIV itself (Reddy et al., 2016; Altekruse et al., 2018). An analysis of the North American AIDS Cohort Collaboration on Research and Design study (NA-ACCORD) indicated that among PWH, approximately half of smoking-related cancer and 94 % of lung cancer diagnoses could be prevented by eliminating smoking (Altekruse et al., 2018).
While a significant proportion of PWH who smoke are interested in quitting (49 %-74 %), (Pacek et al., 2017, 2014) these patients have historically had lower quit rates compared to people without HIV who smoke (Mdodo et al., 2015). Evidence suggests that traditional cessation interventions based on U.S. Clinical Practice Guidelines (USCPG) (Fiore, 2008) alone have limited effectiveness among PWH (Browning et al., 2013; Niaura et al., 2000). In a recent clinical trial, even with the use of varenicline – a first-line pharmacotherapy for smoking cessation – PWH had lower cessation rates and took longer to recover after a lapse compared to those without HIV (Ashare et al., 2021). In addition, studies show that PWH express lower interest in conventional smoking cessation modalities than non-HIV populations. In one survey, only 24.8–42.3 % of PWH who were interested in quitting smoking were interested in using various forms of nicotine replacement therapy (NRT), and less than one-third were interested in using medications like bupropion or varenicline (Pacek et al., 2017). Suboptimal cessation outcomes among PWH and relative lack of interest in conventional smoking cessation approaches (Pacek et al., 2017, 2014; Edwards et al., 2021) suggest the need for innovative, engaging, and tailored interventions for PWH (Kaufman et al., 2021; Shuter et al., 2012).
Mobile interventions range from cellphone-based interventions (e.g., text message-delivered treatments) to digital therapeutics (DTx), in which software designed to prevent or treat diseases is installed on smartphone devices (Digital Therapeutics Alliance, 2019). Mobile interventions represent a promising option to facilitate widespread implementation and adoption of smoking cessation interventions for PWH. Relative to face-to-face interventions, mobile interventions have several advantages including lower cost and greater potential to reach large numbers of PWH (Uthman et al., 2019). Additionally, mobile interventions can be advantageous from an adoption standpoint, as many HIV providers report limited training regarding smoking cessation interventions and limited confidence in their ability to impact smoking behavior (Crothers et al., 2007). Prior work indicates the feasibility and acceptability of smoking cessation interventions delivered via cellphone, (Vidrine et al., 2006, 2012; Aigner et al., 2017) text message, (Tseng et al., 2017) and smartphone (Shuter et al., 2018; McClure et al., 2024) among PWH. Moreover, a meta-analysis concluded that mobile interventions may be more efficacious than face-to-face interventions for smoking cessation among PWH in the short term, but that new approaches may be needed to sustain long-term effects (Uthman et al., 2019). In addition to the promising evidence offered by cessation interventions delivered via this modality, it is important to consider the substantial data supporting tailored behavior change interventions, (Noar et al., 2007; Lustria et al., 2013) suggesting the need to develop mobile smoking cessation interventions that address the unique needs of PWH.
Co-morbid psychological disorders, HIV-related, and cognitive deficits (Nanni et al., 2015; Babel et al., 2021; Deng et al., 2021). represent potential barriers to cessation among PWH. Therefore, we conducted a user-centered design study (manuscript in preparation) to adapt and tailor an existing evidence-based DTx for smoking cessation called Learn to Quit (Vilardaga et al., 2018) to address these three specific factors. The resulting digital intervention, Learn to Quit-HIV (LTQ-H), combines USCPG (Fiore, 2008) and Acceptance and Commitment Therapy (ACT) (Hayes et al., 2011). ACT is a behavioral intervention originally designed to treat psychological disorders that has been shown effective for smoking cessation in previous trials (Gifford et al., 2011; Bricker et al., 2020, 2018). Adapting ACT to help PWH who smoke offers several advantages and opportunities for this population. Negative affect, stress, and mental health symptoms are established predictors of smoking relapse, (Kinnunen et al., 1996; Lerman et al., 1996; Niaura et al., 1999) all of which are common experiences in PWH (Bing et al., 2001; Miles et al., 2019). ACT has theory-based components (i.e., psychological flexibility) that predict cessation (Vilardaga et al., 2014; Heffner et al., 2015; Browne et al., 2021; Bricker et al., 2021) and works by targeting two core skills: (a) acceptance (vs control) of the cognitive, emotional, and physical sensations associated with urges to smoke, and (b) commitment to engage in behaviors that are consistent with stated goals and values (Vilardaga et al., 2014). These core skills of ACT predict both proximal (Vilardaga et al., 2014) and distal cessation outcomes (Heffner et al., 2015). LTQ-H modified six of the fourteen core modules of LTQ to include HIV-relevant content (e.g., psychoeducation about the health impact of HIV and smoking, HIV stigma), added weekly and monthly summary screens, and a new library of notifications.
The present paper reports the results of a pilot randomized controlled trial (i.e., Quitting Matters Pilot; NCT04609514) to evaluate the feasibility, acceptability, and smoking outcomes of LTQ-H compared to an active control app (i.e., QuitGuide). The Quitting Matters Pilot also evaluated the implementation and potential reach of offering smoking cessation treatment in this modality by recruiting PWH in a fully remote trial. We hypothesized that conducting a remote trial testing a DTx among PWH would be feasible and acceptable, and that LTQ-H would result in higher levels of usability and DTx engagement compared to QuitGuide. Secondary outcomes included number of cigarettes smoked per day, quit attempts, and biochemically verified smoking abstinence. No specific benchmarks were originally proposed for these hypotheses.
Methods
Design
2.1.
This study was a 12-week parallel 2-arm randomized controlled trial with virtual follow-up assessments at 4-, 8-, and 12-weeks post-randomization comparing LTQ-H to QuitGuide, a digital intervention matched to LTQ-H in terms of length and means of delivery to control for the effects of time and attention (NCT04609514).
Participants
2.2.
Eligibility criteria included: (1) self-reported HIV-positive status, (2) currently under the care of an HIV provider, (3) self-reported smoking of ≥ 5 cigarettes per day during the past 30 days, (4) ≥ 18 years of age, (5) current interest in quitting smoking, (6) current ownership of an Apple or Android smartphone. Exclusion criteria were: (1) concerns about participant safety by study physician, participant physician, or study Principal Investigators, or inability to provide informed consent, (2) contraindication or prior side effects associated with nicotine patch, (3) current use of NRT or other smoking cessation medication, (4) being pregnant, planning to become pregnant, nursing, or becoming pregnant during the study, and (5) untreated and unstable diagnosis of substance use disorder within the last 30 days.
All participants signed a release of information form with the contact information of their current physician or clinical provider to address potential concerns about eligibility prior to randomization and/or clinical safety during participation in the trial.
Interventions
2.3.
LTQ-H
2.3.1.
LTQ-H is a DTx that can be installed on both Android and Apple iOS operating systems. LTQ-H consists of 324 screens of content divided into: (a) HIV-tailored smoking cessation ACT skills, (b) education about tobacco dependence and treatment, and (c) psychoeducation about NRT and adherence. Content is gradually presented across 28 modules (14 education and 14 skills) that can be completed in no less than 14 days. The modules encourage the learning and practice of three processes of change (i.e., awareness of urges to smoke, openness to experiencing urges, commitment to specific values for quitting). The DTx also includes a self-tracking feature of mood, NRT use, cravings to smoke, acceptance of cravings, and cigarettes smoked daily (CPD). These assessments are not incentivized or necessary to complete the other DTx content or modules. A more detailed description about the design and adaptation of LTQ-H is currently under review.
QuitGuide
2.3.2.
QuitGuide is a DTx based on USCPG for smoking cessation developed for the general population by the Smokefree.gov initiative of the Division of Cancer Control and Population Sciences of the National Cancer Institute (National Cancer Institute, 2022). The intervention includes the following components: (a) psychoeducation about the impact of smoking on health, (b) setting up a quit date and a quit plan, (c) selecting reasons for quitting, (d) tracking of mood, triggers, smoking habits, and (e) tips for quitting. It also contains a journaling feature and the option to opt-in to location- or time-based notifications. More information about QuitGuide’s rationale and content can be found at www.smokefree.gov.
Nicotine replacement therapy
2.3.3.
All participants received an 8-week course of transdermal nicotine patches starting at 21 mg/24 h, and tapered following recommendations contained in the USCPG (Fiore, 2008).
Procedures
2.4.
Participants were recruited through patient referrals from other HIV research studies, infectious disease clinics, and the electronic health record at Duke University School of Medicine, as well as through community clinics in the Durham, N.C. area. Due to national guidelines in response to the COVID-19 pandemic, our trial included procedures to conduct a fully remote pilot trial with expanded recruitment nationwide through online advertisements (e.g. Facebook, Craigslist).
Interested participants were instructed to contact the lab by phone or email to learn more about the study. A phone screening was conducted to assess initial eligibility, followed by a remote video screening visit (week - 1) during which informed e-consent was obtained and additional eligibility for the study were evaluated. Final eligibility was confirmed by the study physician and/or principal investigators. Eligible participants were randomized 1:1 to either LTQ-H or QuitGuide (week 0). This two-step procedure of participant enrollment was designed to allow verification of inclusion criteria and mitigate participant deception (e.g., online professional participants). Research staff guided the randomized participants to install the assigned DTx on their smartphone device. Participants were given instructions to set a quit date within their assigned DTx as well as complete modules and track cigarette use. To protect participants’s privacy, LTQ-H’s notifications excluded any HIV-related messaging as a safeguard to prevent potential disclosure of HIV status. Participant onboarding for each DTx was limited to providing a download link and installation code, consistent with the standalone nature of this digital intervention and to maximize scalability and implementation potential.
Participants continued to receive HIV care as provided by their usual healthcare provider. Virtual visits occurred at 4-, 8-, and 12-weeks post-randomization. Among participants who self-reported abstinence at 12-weeks post randomization, study staff conducted remote (i.e., via Zoom video call) biochemical verification of smoking abstinence using Covita’s iCOquit Smokerlyzers (Bedfont Scientific Ltd). Participants received $130 compensation for participation in all study activities. All study procedures were approved by the Institutional Review Board at Duke University School of Medicine.
Measures
2.5.
Baseline characteristics
2.5.1.
Tobacco Use Behavior.
At baseline, we collected self-reported years of smoking, nicotine dependence, (Heatherton et al., 1991) CPD, frequency of e-cigarettes use, and past 30-day use of other tobacco products.
HIV-Related Characteristics, Social Determinants of Health, and
Mental Health Factors.
We collected information regarding the duration (in years) of HIV diagnosis, and self-reported current CD4 (T-Cell) counts. Other HIV-related measures included internalized HIV stigma using a subscale of the HIV Stigma Mechanisms Scale, (Earnshaw et al., 2013) with scores ranging from 6 to 30 for which high scores indicate greater stigma. Self-perceived discrimination was measured with the Everyday Discrimination Scale, (Krieger et al., 2005) with responses ranging from 5 through 30 and with lower scores indicating higher levels of discrimination.
At baseline we administered the Depression Anxiety Stress Scale (DASS-21) (Lovibond and Lovibond, 1995) and the Brief Symptom Inventory (BSI) (Derogatis, 1992). DASS-21 is a self-report measure of symptoms of depression, anxiety, and stress. Scores for each subscale are categorized into normal, mild, moderate, severe and extremely severe categories. The Global Severity Index is a subscale of the BSI that captures a wider range of psychiatric symptoms, with scores ranging from 0 to 4 and with higher scores indicating more psychiatric severity.
Digital Divide and Familiarity with Technology.
All participants completed a questionnaire internally developed by our team in prior research assessing technology access, familiarity, and use. This survey asked about previous experiences with smartphones, internet availability, range of activities for internet use, and concerns about the use of technology as a health resource or tool.
Substance Use.
Substance use behaviors were examined via self-report surveys including the Drug Abuse Screening Test-10 (DAST-10) and the Alcohol Use Disorders Identification Test (AUDIT), (Skinner, 1982) two widely used and reliable measures with clinical cut-offs of 3 and 8 respectively (Saunders et al., 1993; Yudko et al., 2007). Self-reported daily cannabis use (yes/no), number of days of cannabis use within the last 30 days, and mixing cannabis and tobacco products (yes/no) were collected at baseline with three single items.
Primary outcomes
2.5.2.
Recruitment rate, participant attrition, and population
reach.
2.5.2.1.
Recruitment and participant retention rates were monitored and recorded throughout the study duration. The demographic characteristics of participants and their state of residence were collected at baseline. The pilot trial also tracked the number and geographic location of HIV clinics reached for the purpose of trial advertisement and participant recruitment.
Digital markers of DTx use.
2.5.2.2.
Based on user interactions defined in prior work (see Supplementary Table 1 (Vilardaga et al., 2019)), we used Google Analytics to collect digital markers of LTQ-H use from device metadata. For QuitGuide, metadata was obtained directly from the NCI’s smokefree.gov program via a Data Transfer Agreement. Intensive longitudinal data from each device was grouped and organized to evaluate different metrics of device engagement as shown in Table 2. Specifically, interactions with active smoking cessation content for LTQ-H were extracted from unique counts of any smoking cessation module completed (i.e., 28 modules), which included ACT content in combination with USCPG. For QuitGuide, we extracted unique counts of any new engagement with the following USCPG content: setting up quit date, setting up a quit plan, selecting reasons for quitting, reviewing ‘How to Quit’ guide, or smoking trigger-based tips and feedback.
DTx usability.
2.5.2.3.
DTx’s usability was measured with the Systems Usability Scale (SUS), a 10-item questionnaire with a 5-point Likert scale from strongly agree to strongly disagree and with possible total scores ranging from 0 to 100 (Brooke, 1996). A mean score of 68 is considered a useful benchmark for assessing usability, where 50 % of devices fall below the benchmark of 68 (Hyzy et al., 2022).
Secondary outcomes
2.5.3.
Smoking outcomes.
2.5.3.1.
Secondary outcomes for this pilot trial included quit attempts defined as self-reported no smoking at all for 24 h from baseline to Week 12, change in CPD from baseline to Week 12, and biochemically verified 7-day point prevalence abstinence (i.e., not smoking even a puff of a cigarette within the last 7 days, and less than 5 parts per million of carbon monoxide on a breath test at week 12) (Perkins et al., 2013; Cropsey et al., 2014; Hughes et al., 2003). Adherence to NRT was measured daily with a brief interviewer-administered questionnaire at Weeks 4, 8, and 12 to assess the overall proportion of dispensed NRT used as directed, measured as a continuous variable. Participant safety was assessed by monitoring all adverse events during the 12-week period and in close collaboration with their medical providers.
Data analytic strategy
2.6.
Descriptive statistics were used to report recruitment and participant retention rates. Trajectories of DTx engagement were plotted to examine ongoing interactions with each device. Acceptability outcomes were evaluated descriptively with summary scores of the SUS. Group differences in secondary outcomes were assessed via t-tests, logistic regression, or linear regression, as appropriate. To appropriately account for negatively skewed count distributions and the nested nature of the intensive longitudinal count data we conducted zero inflated negative binomial multilevel models that compared the trajectories of DTx engagement across treatment arms. T-tests were used to evaluate utilization of active smoking cessation content within each DTx. Logistic regression was used to evaluate the differences in biochemically verified 7-day point prevalence abstinence using the full intent to treat sample (missing = smoking). Logistic regression models were adjusted for baseline variables with an observed imbalance across arms (i.e., baseline levels of psychological stress, daily cannabis use, mixed cannabis and tobacco use, and number of cigarettes per day). T-tests and linear regression were used to evaluate the differences in change in cigarettes per day, quit attempts, adherence to NRT and participant safety. No alpha corrections were conducted for this analysis given the pilot nature of this study (Leon et al., 2011). All statistical analyses were conducted with R version 4.4.2.
Results
Pilot trial recruitment and retention
3.1.
Recruitment of participants took place between February 22, 2021 and March 2, 2022 at a rate of 3.5 participants per month. The last participant completed the study on June 3, 2022. A total of 531 potentially eligible individuals (i.e., self-reported smoking and HIV) were contacted for an initial phone screening. Among the 51 PWH who completed informed consent procedures, 8 were not randomized due to failing screening procedures or not completing the screening visit. Forty-three participants were randomized to a treatment condition, and 2 were withdrawn by the PI due to new information obtained after randomization indicating that these participants did not meet the eligibility criteria (see CONSORT chart in Fig. 1). The pilot trial had a retention rate of 78 %, defined as all randomized participants who responded to our last follow-up survey.
To obtain preliminary data about the potential reach of DTx for smoking cessation among PWH populations, we contacted 31 HIV clinics and two smoking cessation centers across the U.S. (i.e., orange dots in Fig. 2) to introduce our study and provide recruitment materials. Sixteen clinic administrators responded to our initial email, and among those, ten clinics expressed interest in a 10-minute introductory session to their team to discuss the study. Finally, we presented our study to the clinical and administrative leadership of nine clinics; all agreed to post our flyers at their clinic locations and/or refer their patients to our study line. In sum, 30 % of the clinics we contacted formally or informally advertised the study to their patient pool.
Participant characteristics
3.2.
The final sample (n = 41) was racially diverse with approximately equal proportions of White and Black participants (Table 1). More than 75 % of participants reported having high school or fewer years of education, and having lived with a diagnosis of HIV for almost two decades. Randomization to treatment arms rendered comparable participant characteristics across basic demographics, HIV medical history, drug and alcohol use, HIV stigma, experiences of discrimination, and familiarity with technology. However, relative to QuitGuide, LTQ-H arm participants were more likely to have above normal levels of psychological stress (36 % vs 11 %), higher prevalence of any cannabis use in the past 12 months (54 % vs 10 %), more days of cannabis use in the past 30 days (mean 16 days vs 8 days), higher percentage of self-reported mixing cannabis and combustible tobacco products (18 % vs 5 %), more baseline cigarettes use per day (mean 16.05 vs 12.22), higher prevalence of e-cigarettes use (9 % vs 0 %), and higher prevalence of other tobacco products (27 % vs 5 %). Scores on the DAST-10 and the AUDIT were also similar across arms. Across arms, participants reported low levels of perceived discrimination and internalized HIV stigma (see Table 1).
Digital markers of device engagement
3.3.
Seven participants in the LTQ-H arm (33 %) generated only partial digital markers due to mechanical error caused by a software upgrade. When partial digital markers were included, participants in the LTQ-H arm had 1524 more interactions with LTQ-H than QuitGuide (3610 vs 2086), with an average of interactions per day of 1.82 (SD=2.11) compared to 1.21 (SD=4.28) for QuitGuide. During the first 30 days of DTx use, the average was of 2.89 (SD=2.98) for LTQ-H versus 1.82 (SD=6.48) for QuitGuide. A zero-inflated negative binomial multilevel count model indicated that these differences were statistically significant. The LTQ-H arm also had a significant and larger effect than QuitGuide on the count of days of device use using the same statistical model. LTQ-H users completed close to four times as much active smoking cessation content as QuitGuide users. Only 5 participants in the QuitGuide arm (26 %) versus 22 (100 %) participants in the LTQ-H engaged with active smoking cessation content. See Table 2 for all results and Fig. 3 for raw interaction data.
Device usability
3.4.
LTQ-H and QuitGuide had scores on the SUS above the standard cut-off (i.e., 68; See Table 2) that were not statistically different between arms.
Smoking reductions, quit attempts, and smoking abstinence
3.5.
There were no differences in absolute reductions in CPD in LTQ-H vs QuitGuide. QuitGuide participants, compared to LTQ-H participants, made a larger but not significantly different mean number of quit attempts. Biochemically verified 7-day point prevalence abstinence at week 12 for the intent-to-treat sample was 18.2 % (4/22) for LTQ-H vs 15.8 % (3/19) for QuitGuide. Our statistical model adjusted for baseline levels of cigarettes smoked per day, days of cannabis use in the past 30 days, mixed cannabis and combustible tobacco use, and psychological stress. In completer’s analysis (n = 32) adjusted for the same variables, biochemically verified 7-day PPA was 23.5 % for LTQ-H versus 20.0 % for QuitGuide (see Table 2 for all statistical values).
Nicotine replacement patch adherence and participant’s safety
3.6.
Adherence to the nicotine patch was similar across treatment arms (31.0 % for LTQ-H vs 31.6 % for QuitGuide) and not statistically different. Similarly, no serious adverse events were reported during the study, and no statistical differences in number of adverse events were identified by study arm (see Table 2).
Discussion
The Quitting Matters Pilot demonstrated that it is feasible to reach a demographically and geographically diverse sample of PWH for the purpose of remotely delivering smoking cessation interventions for this population using a mobile digital device (e.g., DTx). Furthermore, it demonstrates that DTx can lead to high levels of treatment engagement and utilization with these technologies in this population. Our remote trial was able to reach PWH from 10 US states, as well as HIV clinics across the Eastern US and engage with a sizeable portion of contacted clinics. Relative to QuitGuide, a standard of care DTx for smoking cessation developed by the National Cancer Institute that has shown efficacy in prior trials, (Bricker et al., 2020) our tailored DTx for PWH (LTQ-H) achieved comparable levels of device usability, but significantly higher rates of days of use, total amount of device engagement, and targeted interactions with active smoking cessation content. These levels of engagement were assessed during a 90-day period using state-of-the-art statistical approaches for intensive longitudinal data. This finding is important, since in a previous DTx study, we demonstrated that device engagement with LTQ, and not QuitGuide, causally mediated smoking outcomes at trial endpoint (Browne et al., 2021). Further, more than 75 % of PWH recruited in this study had high school or fewer years of education which demonstrates that the LTQ-H device engaged a population traditionally underrepresented in technology-based interventions (Mackert et al., 2016; Kontos et al., 2014). Individuals with lower educational attainment often face barriers to accessing and benefiting from digital health tools (Berkman et al., 2011). Therefore, successfully engaging this group suggests that the LTQ-H device is both usable and engaging across diverse educational backgrounds, ensuring that digital innovations do not exacerbate existing health disparities (Latulippe et al., 2017).
While the Quitting Matters Pilot trial was not powered to detect statistical differences between arms in smoking outcomes, LTQ-H had descriptively higher rates of biochemically confirmed smoking abstinence, and larger smoking reductions from baseline to trial endpoint. It is important to note that our randomization procedure failed to equally distribute participants across baseline features known from previous research to predict low quit rates, such as cannabis use, mental health symptoms, and smoking intensity (Ni et al., 2020; Streck et al., 2020; Rogers et al., 2020). More specifically, participants randomized to LTQ-H used cannabis on twice the number of days in the prior thirty days compared to participants randomized to QuitGuide, had three times greater levels of psychological stress than QuitGuide participants, and smoked more CPD at baseline. Moreover, biochemical verification of one participant assigned to the LTQ-H arm failed likely due to self-reported combustible cannabis use prior to the verification test, which is consistent with the fact that 18 % of LTQ-H participants (vs 5 % for QuitGuide) reported at baseline mixing cannabis and combustible tobacco products.
The results of this pilot trial suggested that conducting a remote clinical trial of digital interventions for smoking cessation in this population was acceptable but may require a more robust recruitment strategy (e.g., higher incentives and/or clinic involvement). Further, the use of biochemical verification improved the accuracy of our outcomes. However, combustible cannabis use limits this approach to biochemical verification, which may have reduced our overall quit rate for the LTQ-H arm. The Quitting Matters pilot suggests that future studies should use a combination of CO and cotinine samples to minimize false positives, which has been tested in remote studies (Raiff et al., 2022; Kong et al., 2017) and is consistent with recent guidelines (Benowitz et al., 2020).
The largest study examining the use of a digital intervention for smoking cessation in this patient population found quit rates of 14.9 % (Shuter et al., 2022). Other pilot studies like the one reported here found quit rates ranging from 15 % to 40 %, (Schnall et al., 2022; Poudel et al., 2023; Bui et al., 2022) yet those studies used different endpoints (e.g., 2-month follow-up), (Bui et al., 2022) international populations (e.g., Cambodia) (Poudel et al., 2023; Bui et al., 2022) or reported different primary smoking outcomes (e.g., smoking reductions) (McClure et al., 2024). Together with the fact that LTQ-H demonstrated high levels of device engagement during the three months trial period, these smoking outcomes suggest that LTQ-H holds great promise for the remote delivery of smoking cessation interventions among PWH.
From an implementation science standpoint, the levels of HIV clinic outreach of the Quitting Matters Pilot are particularly significant in the context of the COVID-19 pandemic. One of the clinic directors stated that, “My professional life has been completely overtaken by COVID.” We believe this statement represented the experience of many infectious disease clinics in the U.S. at the time we recruited for this pilot study. In that context, the proportion of clinics that expressed interest in our study provides preliminary support for the implementation of LTQ-H in HIV clinics throughout the country.
Our pilot trial had several limitations. First, our recruitment rates were slightly low relative to the total number of candidates that were initially contacted, which is typical of trials recruiting patients for cancer treatment and low prevalence diseases or conditions such as HIV (Lara et al., 2001; Haider, 2022). However, these low recruitment rates call for a more robust national recruitment strategy in this patient population. Our two-step procedure of participant enrollment and verification (i.e., one screening visit followed by a randomization visit) may have reduced our final enrollment rates, but this procedure also mitigated participant deception, a common occurrence in online clinical trials (Heffner et al., 2021). Low recruitment rates can also be expected from pilot studies with a moderate budget for personnel and advertisement such as this pilot. Overall, one year of recruitment generated a sample size that was fully adequate for the goals of a pilot trial (Eldridge et al., 2016a). Second, our biochemical verification relied solely on expired breath CO, which has inherent limitations (e.g., it cannot confirm abstinence beyond 3–5 days) and may have been inappropriate for a population with high levels of combustible cannabis use. Rogers et al., (2020); Rice et al., (2022). Data from this pilot study also suggests a more adaptable biomarker collection procedure (both CO and cotinine) to avoid sample contamination from e-cigarettes, or NRT use, as conducted in prior remote trials (Vilardaga et al., 2019; Brooke, 1996). The use of anatabine/anabasine to capture combustible tobacco products could also be considered. A more adaptable biomarker collection approach is consistent with most recent SRNT taskforce guidelines (Benowitz et al., 2020). Third, notable imbalances between treatment arms in patient characteristics known to predict low quit smoking rates may have biased our study in favor of the QuitGuide app. Larger trials may consider stratified randomization to account for the strong influence of these patient characteristics. Fourth, both LTQ-H and QuitGuide directly encouraged the use of NRT. However, adherence to the NRT patch was low (<32 %), and did not differ between arms. These low adherence rates were consistent with prior literature, (Pacek et al., 2018) and in this study could also be explained by the lack of in-person contact with a provider (low-touch medical oversight), a clinical tradeoff between more intensive treatment modalities and remote digital trials that ultimately favors scalability and high reach. Finally, while the study was able to collect a significant number of device interactions with LTQ-H and QuitGuide, an unexpected software upgrade led to a loss of 32 % of device interactions in the LTQ-H arm. However, the statistical approach we chose to analyze this data provided robust parameter estimates to account for individual and group variability in intensive longitudinal datasets and ample statistical power to evaluate our device engagement hypotheses.
In conclusion, the Quitting Matters Pilot trial demonstrated that LTQ-H, a novel digital intervention, has the potential to engage a racially and demographically diverse population of PWH with low literacy, may achieve higher user engagement and acceptability than a DTx designed for the general population, and shows promising smoking cessation outcomes. This pilot also established the feasibility of conducting a fully remote trial with biochemical verification in this population and fostered community partnerships with HIV clinics. Building on these findings, a fully powered, nationwide remote hybrid Type 1 effectiveness-implementation trial is currently underway to evaluate the effectiveness and implementation potential of LTQ-H among a larger sample of PWH across the U.S. (NCT06883097).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aigner CJ, Gritz ER, Tamí-Maury I, Baum GP, Arduino RC, Vidrine DJ, 2017. The role of pain in quitting among human immunodeficiency virus (HIV)-positive smokers enrolled in a smoking cessation trial. Subst. Abus 38 (3), 249–252. 10.1080/08897077.2017.1291466.28328303 PMC 6691496 · doi ↗ · pubmed ↗
- 2Altekruse SF, Shiels MS, Modur SP, Land SR, Crothers KA, Kitahata MM, Thorne JE, Mathews WC, Fernández-Santos DM, Mayor AM, Gill JM, Horberg MA, Brooks JT, Moore RD, Silverberg MJ, Althoff KN, Engels EA, 2018. Cancer burden attributable to cigarette smoking among HIV-infected people in North America. AIDS 32 (4), 513–521. 10.1097/QAD.0000000000001721.29239891 PMC 5797998 · doi ↗ · pubmed ↗
- 3Asfar T, Perez A, Shipman P, Carrico AW, Lee DJ, Alcaide ML, Jones DL, Brewer J, Koru-Sengul T, 2021. National estimates of prevalence, time-trend, and correlates of smoking in US people living with HIV (NHANES 1999–2016). Nicotine Tob. Res 23 (8), 1308–1317. 10.1093/ntr/ntaa 277.33856483 PMC 8517967 · doi ↗ · pubmed ↗
- 4Ashare RL, Wileyto EP, Logue-Chamberlain E, Gross R, Tyndale RF, Lerman C, Hawk LW, Cinciripini P, George TP, Lubitz SF, Schnoll R, 2021. Patterns of lapses and recoveries during a quit attempt using varenicline and behavioral counseling among smokers with and without HIV. Psychol. Addict. Behav 35 (7), 788–796. 10.1037/adb 0000619.32686950 PMC 7855008 · doi ↗ · pubmed ↗
- 5Babel RA, Wang P, Alessi EJ, Raymond HF, Wei C, 2021. Stigma, HIV risk, and access to HIV prevention and treatment services among men who have sex with men (MSM) in the United States: a scoping review. AIDS Behav 25 (11), 3574–3604. 10.1007/s 10461-021-03262-4.33866444 PMC 8053369 · doi ↗ · pubmed ↗
- 6Benowitz NL, Bernert JT, Foulds J, Hecht SS, Jacob P, Jarvis MJ, Joseph A, Oncken C, Piper ME, 2020. Biochemical verification of tobacco use and abstinence: 2019 update. Nicotine Tob. Res 22 (7), 1086–1097. 10.1093/ntr/ntz 132.31570931 PMC 7882145 · doi ↗ · pubmed ↗
- 7Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K, 2011. Low health literacy and health outcomes: an updated systematic review. Ann. Intern Med 155 (2), 97–107. 10.7326/0003-4819-155-2-201107190-00005.21768583 · doi ↗ · pubmed ↗
- 8Bing EG, Burnam MA, Longshore D, Fleishman JA, Sherbourne CD, London AS, Turner BJ, Eggan F, Beckman R, Vitiello B, Morton SC, Orlando M, Bozzette SA, Ortiz-Barron L, Shapiro M, 2001. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch. Gen. Psychiatry 58 (8), 721–728. 10.1001/archpsyc.58.8.721.11483137 · doi ↗ · pubmed ↗