Concurrent Vascular and Pelvic Anomalies of the Kidney: A Rare Cadaveric Observation
Amartya Mishra, Vaishaali TM, Muhamed Faizal PA, Khursheed Raza, Ajay Patel, Ruchi Ratnesh, Neelam Kumari, Suyashi Sharma, Himel Mondal

TL;DR
This case report describes rare anatomical variations in the kidney's blood vessels and pelvis found during a cadaver dissection in India.
Contribution
The paper presents a rare concurrent occurrence of multiple renal vascular and pelvic anomalies in a single cadaver.
Findings
The right kidney had three arteries, including one from the right common iliac artery.
Bilateral venous variations were observed, with complex tributary patterns into the inferior vena cava.
A trifid renal pelvis was found on the right side, with three distinct infundibula draining separate calyces.
Abstract
This case report describes the concurrent occurrence of rare renal vascular and pericalyceal variations and highlights their surgical significance. The renal vasculature and pelvis exhibit a wide spectrum of anatomical variations, many of which are clinically and surgically significant. Awareness of these deviations is of immense importance during retroperitoneal and renal surgeries and interventions. This report presents concurrent variations in both renal arteries and veins, as well as the renal pelvis, observed in a cadaver during routine dissection at the All India Institute of Medical Sciences, Deoghar, Jharkhand, India. Standard retroperitoneal dissection techniques were employed to expose and examine the structures. Observations were based on direct anatomical inspection and morphometric measurements. Variations were noted in the arterial supply, where at least three arteries…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1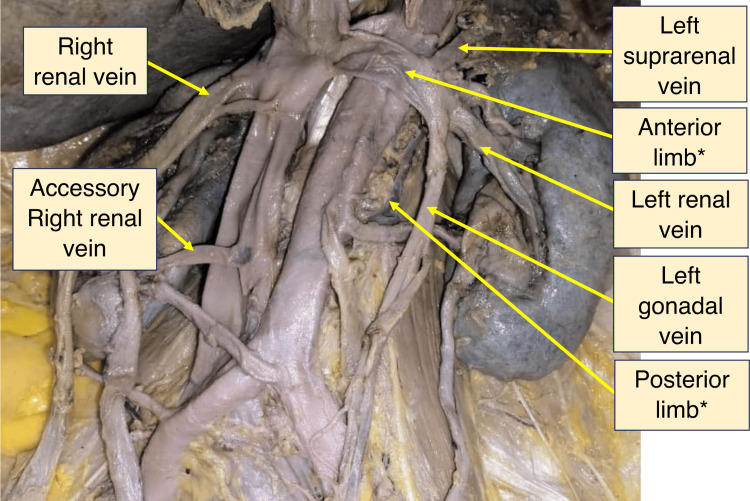 Figure 2
Figure 2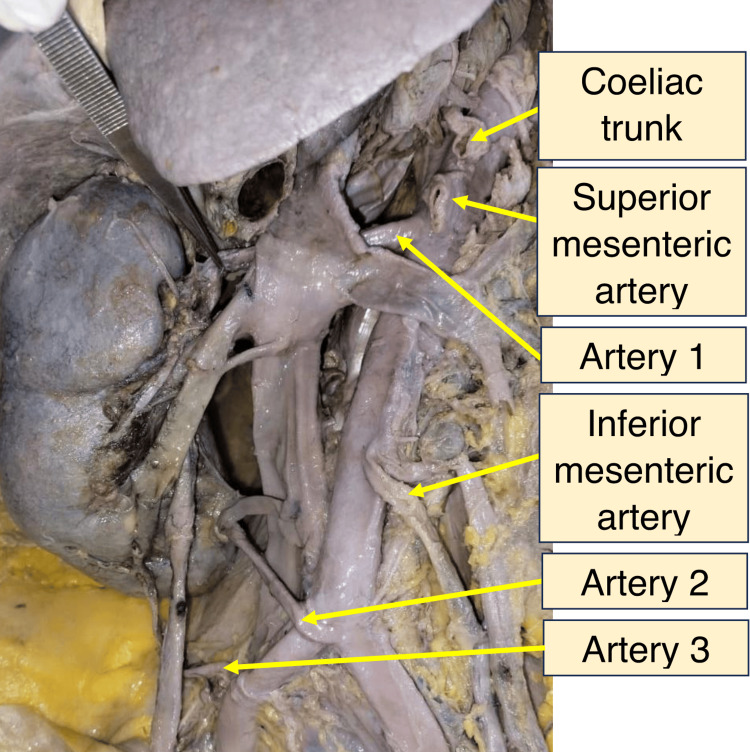 Figure 3
Figure 3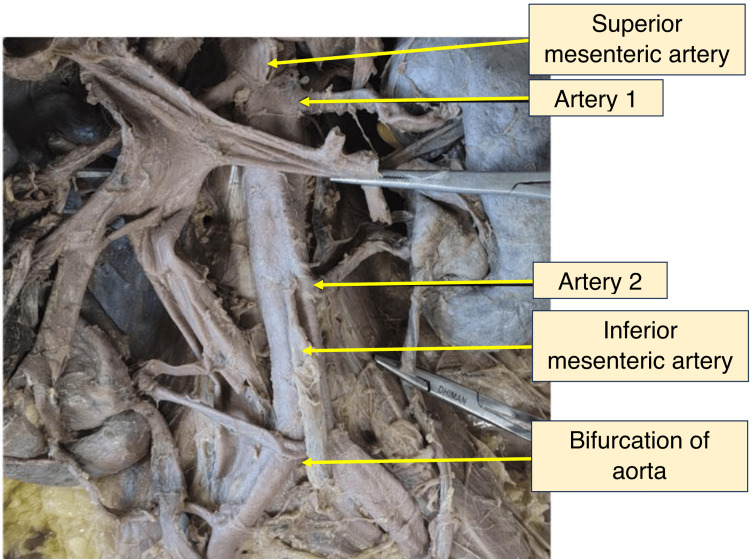 Figure 4
Figure 4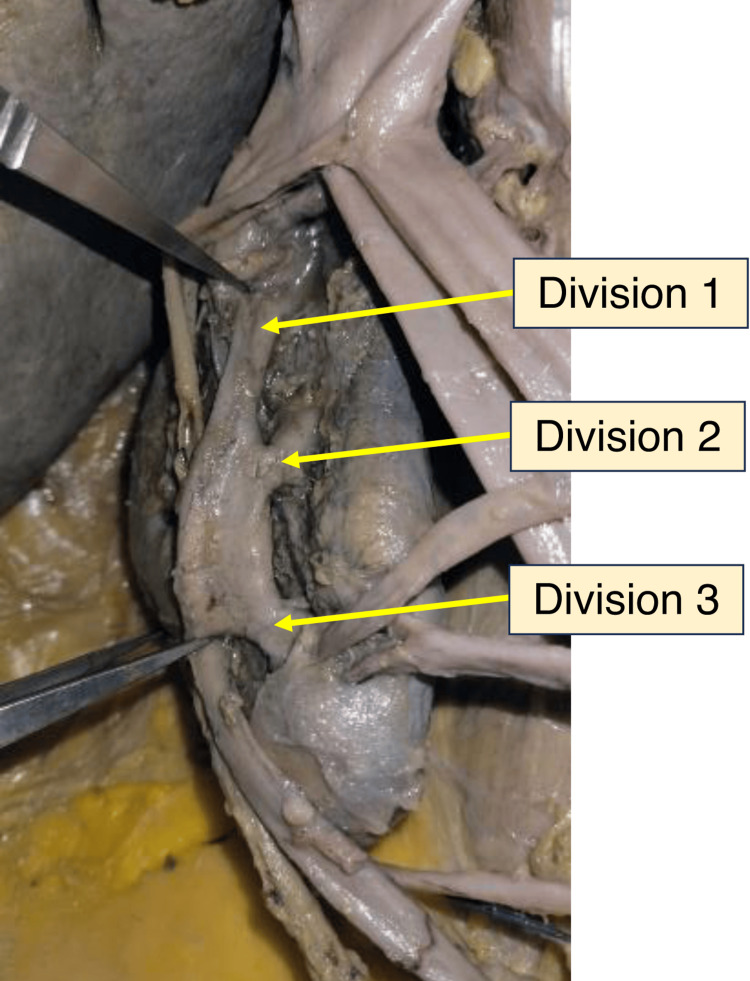 Figure 5
Figure 5 Figure 6
Figure 6| Dimensions | Right kidney | Left kidney | |
| Length | 134.8 mm | 135.2 mm | |
| Breadth | At hilum | 62.9 mm | 69.2 mm |
| At the upper pole | 29.4 mm | 32.8 mm | |
| At the inferior renal pole | 34.1 mm | 31.9 mm | |
| Thickness | 43.9 mm | 47.2 mm | |
| Length of the hilum | 67.9 mm | 71.3 mm | |
| Parameter | Artery 1 | Artery 2 | Artery 3 | |
| Origin | Just beneath the superior mesenteric artery (122.2 mm proximal to the bifurcation of the abdominal aorta) | At the bifurcation of the aorta | Right common iliac artery (42.23 mm from the bifurcation of the abdominal aorta) | |
| Distance (from the inferior renal pole) | 100.3 mm | 26.1 mm | 27.1 mm | |
| Length (from aorta to entry point) | 96.2 mm | 71.2 mm | 98.4 mm | |
| Diameter | At origin | 7.1 mm | 4.9 mm | 3.8 mm |
| At the entry site | 4.7 mm | 3.7 mm | 2.9 mm | |
| Parameter | Artery 1 | Artery 2 | |
| Origin | 123.5 mm proximal to the bifurcation of the aorta | 64.2 mm proximal to the bifurcation of the aorta | |
| Distance (from the inferior renal pole) | 96.2 mm | 55.1 mm | |
| Length (from aorta to entry point) | 61.2 mm | 75.3 mm | |
| Diameter | At origin | 4.8 mm | 5.4 mm |
| At the entry site | 3.9 mm | 4.2 mm | |
| Division of the renal pelvis | Distance from the inferior pole of the kidney |
| Division 1 | 10.4 cm |
| Division 2 | 6.5 cm |
| Division 3 | 3.5 cm |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Renal and Vascular Pathologies · Pediatric Urology and Nephrology Studies
Introduction
The kidney is supplied by a renal artery and drained by a renal vein, both of which show significant anatomical variations. Usually, a single renal artery arises from the abdominal aorta opposite the intervertebral disc between L1 and L2, while a renal vein drains into the inferior vena cava (IVC) [1]. According to Soares et al., one or more renal arteries may be present in 25-30% of individuals [2]. While isolated variations of renal artery variants are relatively common, there are very few documented cases of bilateral complex arterial configurations such as the crossed arterial pattern and differing branching types, which are relatively rare, highlighting the novelty of concurrent vascular deviations when studied anatomically [3].
Similarly, veins and the renal pelvis also show deviations from the usual configuration. The persistence or regression of embryonic vessels, along with rotation and ascent of the kidneys, gives rise to such variations [4]. These hold critical significance when viewed from a clinical and surgical perspective. Recognition of such variations in the vasculature and pelvis, especially when present in the same individual, is essential for accurate anatomical interpretation, effective surgeries, and prevention of intraoperative complications [5].
This case report describes concurrent variations observed during routine dissection, their clinical implications, and embryological basis, and provides future research recommendations.
Case presentation
The dissection was performed on a formalin-embalmed 70-year-old female cadaver. The cadaver used in this study was donated to the Department of Anatomy, All India Institute of Medical Sciences, Deoghar, for educational and research purposes. The dissection was conducted in accordance with institutional ethical guidelines. Donor anonymity and dignity were strictly maintained. Variations were identified as deviations from standard anatomical descriptions. Multiple renal arteries or veins, anomalous origins or terminations, and atypical pelvicalyceal configurations were classified as variations. All structures were traced from origin to termination to confirm the findings.
A midline incision from the xiphoid process to the pubic symphysis provided access to the abdominal cavity. The anterior abdominal wall was reflected, and selected viscera were removed to expose the retroperitoneal structures. The peritoneum was stripped, and branches of the aorta between the superior mesenteric artery and the aortic bifurcation were traced [6] and finely dissected. Renal veins and their tributaries were traced from the renal hilum to their termination at the IVC. The renal pelvis and ureter were also traced from the hilum to the urinary bladder. Measurements were taken using a standard 150 mm (6”) digital caliper (AMAZINGs GmbH, Stuttgart, Germany) and a flexible measuring tape. All dissections and measurements were performed independently by two experienced observers. Each renal artery, vein, and pelvicalyceal structure was traced from origin to termination and examined carefully. While the observations were not conducted in a blinded manner, both observers cross-checked findings and repeated measurements to ensure accuracy and consistency. All measurements were taken from the inferior renal pole to the described structure along the external surface of the kidney using the digital vernier caliper.
During dissection, the gross renal anatomy and measurements of both kidneys were recorded. Table 1 presents the dimensions of the right and left kidneys as measured by the digital vernier caliper. Figure 1 illustrates the measurement of the right kidney’s width at the hilum.
Measurement of the width of the right kidney at the level of the hilum
Multiple renal arteries and veins supplying both kidneys were observed. Figure 2 shows the venous drainage of both kidneys in situ, while Figure 3 shows multiple right renal arteries (arteries 1, 2, 3) in situ.
Venous drainage of both kidneys as seen in situof circumaortic renal collar*
Photograph of the right side of the dissected abdomen showing multiple renal arteries as seen in situ (arteries 1, 2, 3)
On the right, the highest renal artery originated laterally from the abdominal aorta just below the superior mesenteric artery and entered the hilum. The second artery arose abnormally at the aortic bifurcation and entered the inferior part of the medial margin. The third artery originated from the right common iliac artery and entered the inferior pole of the kidney. On the left, two arteries arose from the abdominal aorta at different levels proximal to its bifurcation and entered the hilum. Their specifications are shown in Figure 4 (arteries 1, 2). Measurements of the arteries to both kidneys are provided in Tables 2-3.
Photograph of the left side of the dissected abdomen showing multiple renal arteries as seen in situ (arteries 1, 2)
The left renal vein (LRV) displayed a circumaortic variation with two distinct limbs: anterior (preaortic) and posterior (retroaortic). The anterior limb was formed from the union of two venous channels that drained the left kidney and received the left suprarenal and left gonadal vein, the former being proximal to the latter (concerning termination of LRV at IVC). The posterior limb (retroaortic) independently drained a portion of the kidney and joined the IVC posterior to the aorta. The anterior and posterior limbs originated from separate tributaries at the renal hilum, creating a venous collar around the abdominal aorta. The anterior limb measured 8.2 cm in length and originated approximately 8.2 cm from the inferior renal pole. The posterior limb was 10.53 cm long and originated about 5.3 cm from the inferior renal pole.
In the right kidney, the right renal vein (RRV) had three discrete tributaries. Vein 1 originated 9.1 cm from the inferior renal pole and was 2.3 cm long. Vein 2 was 2.8 cm long and originated 6.4 cm from the inferior renal pole. Vein 3 measured 3.5 cm and originated 3.5 cm from the inferior renal pole. An independent venous channel branched from the RRV and drained into the IVC proximal to the primary renal vein termination. Another channel, 4.4 cm long, drained separately into the IVC from a point 3.4 cm above the inferior renal pole. The right gonadal vein also drained into the RRV.
An unusual formation of the right renal pelvis was observed. The pelvis displayed a trifid arrangement, branching into three divisions, each directing flow to a separate major calyx. These divisions merged to form a single ureteric channel, as shown in Figures 5-6. Measurements of each division from the inferior pole of the kidney are provided in Table 4. The left kidney was drained by a single pelvis that continued into a single ureter. Measurements along the intrarenal collecting system were not performed.
Renal pelvis reflected to show a trifid configuration
In situ dissection of the kidneys showing a trifid pelvis on the right, with no variations observed on the left
Discussion
These findings are important as they demonstrate the coexisting anomalies in the vasculature and pelvis, rather than isolated anomalies, depicting the degree of synchronicity required during embryogenesis. There are previously reported cases of multiple renal arteries occurring in roughly 29% of kidneys [7], multiple renal veins in ~17% (more frequent on the right) [8], and a trifid renal pelvis is extremely rare and is reported only as isolated case reports [9], making the simultaneous occurrence of all three findings highly uncommon. In this cadaver, equally notable arterial counterparts accompanied the venous anomalies, including multiple renal arteries on both sides arising from the abdominal aorta and the right common iliac artery. Hostiuc et al. reported a prevalence of circumaortic LRV of 3.5% [8]. Additionally, the renal pelvis displayed a trifid configuration on the right - an extremely rare occurrence attributed to atypical branching of the ureteric bud during gestation [10]. Such variants are typically asymptomatic and are most often identified incidentally on imaging.
From a clinical perspective, the coexistence of multiple vascular and pelvicalyceal variations considerably heightens operative risk. The accessory renal artery, with an average external diameter of 3-4 mm, probably supplies a distinct renal segment. If inadvertently ligated during renal surgery, this could increase the risk of segmental ischemia. Both limbs of the circumaortic channel require careful identification, and failure to control them could result in significant hemorrhage. The trifid pelvis with three separate infundibula may complicate endourological procedures and predispose to stasis or incomplete drainage. Aberrant vessels complicate surgical dissection and vascular control, increasing the likelihood of severe hemorrhage or compromised renal venous drainage [11]. Ureteropelvic junction obstruction and subsequent hydronephrosis may result due to mechanical compression of the ureter by anteriorly crossing arteries [12]. In case of a circumaortic venous collar, during a nephrectomy, if both limbs are not clamped properly, it might lead to hemorrhage [13]. Inadvertent injury or ligation of these terminal arteries, lacking any collateral circulation, can precipitate ischemia within the dependent renal segment [14]. Such anomalies gain indispensable significance in procedures like renal transplantation, nephron-sparing surgeries, and abdominal aortic aneurysm repair [15]. Likewise, endourological or reconstructive approaches are highly influenced by pelvicalyceal variations, as unexpected branching becomes a crucial consideration in planning drainage or stenting, and may predispose patients to urinary stasis, recurrent infections, hydronephrosis, and calculi formation [16].
The mesonephric arteries, arising from the dorsal aorta, that fail to regress during the ascent of the kidney from the pelvis through the lumbar region, give rise to supernumerary arteries. According to a study, 30.76% of the supernumerary arteries arise from the aorta, while 12.82% from renal arteries [17]. Around the eighth week of intrauterine life, retroaortic and preaortic segments form a venous ring. Usually, the retroaortic ring regresses, but when both divisions persist, a circumaortic renal vein results [13]. The nephric duct gives rise to the ureteric bud, which undergoes sequential branching due to the effect of the metanephric mesenchyme to form the renal pelvis, calyces, and collecting ducts. These divisions, due to premature or excessive branching or incomplete fusion, may lead to the formation of a triplication or trifid pelvis, in which three infundibula separately drain separate calyces and join distally [18].
A major limitation of this case report is that it is cadaveric, and hence, the functional consequences of these vascular and pelvicalyceal variations could not be assessed. The embalming of the cadaver may have affected vessel diameter and tissue pliability, potentially altering spatial relationships. Also, the images included in this case report were photographed during routine dissection, and no calibrated imaging equipment was used, which would allow the addition of scale bars. Similarly, fixed directional indicators could not be reliably incorporated, as the relative position and orientation of the structures would vary during dissection and acquisition of the image. Furthermore, this is a single case and cannot be generalized to the population.
In the future, studies could combine radiological imaging and cadaveric data to better define the prevalence and anatomical variations of coexisting anomalies. Virtual three-dimensional reconstruction may assist in preoperative planning. Correlating such anatomical findings with surgical outcomes could improve patient safety during complex interventions.
Conclusions
This case report highlights anatomical variations involving accessory arteries, anomalous venous channels, including a circumaortic channel, and a trifid pelvis, coexisting in the same individual. These variations increase intraoperative complexity and the risk of hemorrhage and urinary outflow obstruction if unrecognized. This report adds to the anatomical and surgical literature, emphasizing that renal variations should be dealt with as integrated patterns rather than isolated findings. Thorough preoperative imaging and assessment are therefore required to avoid complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Multiple renal vascular variations: a case series Int J Anat Var Potaliya P Sharma S Kataria D Dixit SG Ghatak S 9092112018 https://www.pulsus.com/scholarly-articles/multiple-renal-vascular-variations-a-case-series-4754.html
- 2Variations in human renal arteries Acta Sci Biol Sci Soares TR Ferraz JS Dartibale CB Oliveira IR 277282352013 https://www.researchgate.net/publication/270936825_Variations_in_human_renal_arteries
- 3A rare bilateral renal arterial configuration featuring a right-sided crossed trajectory and left-sided type I Ia branching: morphometric and embryological insights from cadaveric dissection Surg Radiol Anat Bagci S Ogut E Turkoglu P Falay Kislalioglu M Balyemez GS Isik M Barut C 2024720254093111510.1007/s 00276-025-03717-6 · doi ↗ · pubmed ↗
- 4Multiple variations of the renal and testicular vessels: possible embryological basis and clinical importance Surg Radiol Anat Mazengenya P 7297333820162650707110.1007/s 00276-015-1584-7 · doi ↗ · pubmed ↗
- 5Analysis of surgical errors associated with anatomical variations clinically relevant in general surgery. Review of the literature Transl Res Anat Kowalczyk KA Majewski A 232021
- 6Morphogenesis and molecular mechanisms involved in human kidney development J Cell Physiol Faa G Gerosa C Fanni D Monga G Zaffanello M Van Eyken P Fanos V 1257126822720122183021710.1002/jcp.22985 · doi ↗ · pubmed ↗
- 7Multiple renal vessels: the anatomical variants with clinical implications in renal interventions and hypertension Ann Afr Med Bolla SR Ispolov Z Nusserova G Tazhibay M Jumadilova D 202510.4103/aam.aam_207_2540924571 · doi ↗ · pubmed ↗
- 8Anatomical variants of renal veins: a meta-analysis of prevalence Sci Rep Hostiuc S Rusu MC Negoi I Dorobanțu B Grigoriu M 9201910.1038/s 41598-019-47280-8PMC 665848031346244 · doi ↗ · pubmed ↗