Liver Embolization for Subcapsular Hematoma in HELLP (Hemolysis, Elevated Liver Enzymes, and Low Platelets) Syndrome: A Case Report
El Hajjami Ayoub, Bouktib Youssef, Badr Boutakioute, Meriem Ouali Idrissi, Najat Cherif Idrissi El Ganouni

TL;DR
A 38-year-old woman with HELLP syndrome and a subcapsular liver hematoma was successfully treated with embolization, avoiding surgery.
Contribution
This case report demonstrates the effectiveness of transarterial embolization as a minimally invasive treatment for subcapsular hepatic hematoma in HELLP syndrome.
Findings
Transarterial embolization using microparticles achieved complete hemostasis and preserved hepatic perfusion.
The patient's hematoma resolved and laboratory parameters normalized without surgical intervention.
Multidisciplinary collaboration improved maternal outcomes in a high-risk obstetric case.
Abstract
HELLP syndrome is a severe obstetric complication characterized by hemolysis, elevated liver enzymes, and low platelet count, typically occurring in the third trimester or postpartum period. One of its rare but life-threatening complications is subcapsular hepatic hematoma, which may rupture and cause catastrophic hemorrhage. We report the case of a 38-year-old woman with type 2 diabetes mellitus who developed severe right upper quadrant pain three days after a cesarean delivery complicated by eclampsia. Laboratory findings were consistent with HELLP syndrome. Abdominal ultrasound and contrast-enhanced computed tomography (CT) revealed a right subcapsular hepatic hematoma measuring 34 mm in thickness, associated with hepatic infarctions and moderate ascites. Given the high risk of rupture, urgent transarterial embolization was performed via selective catheterization of the right hepatic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
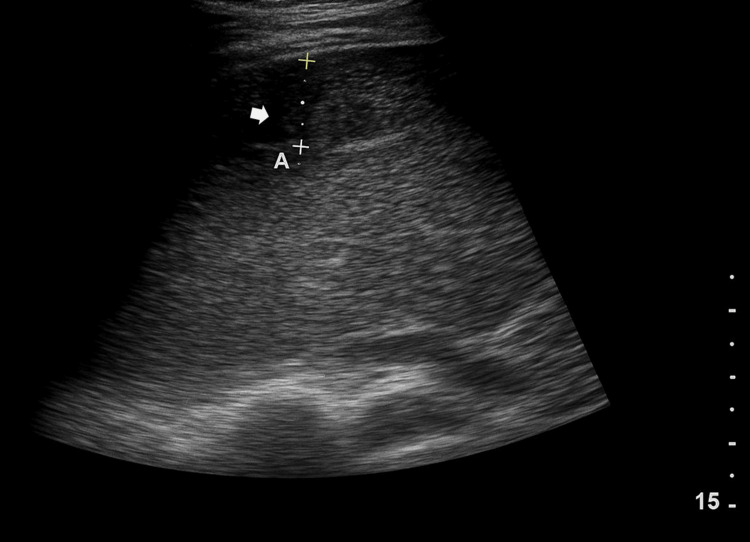 Figure 1
Figure 1 Figure 2
Figure 2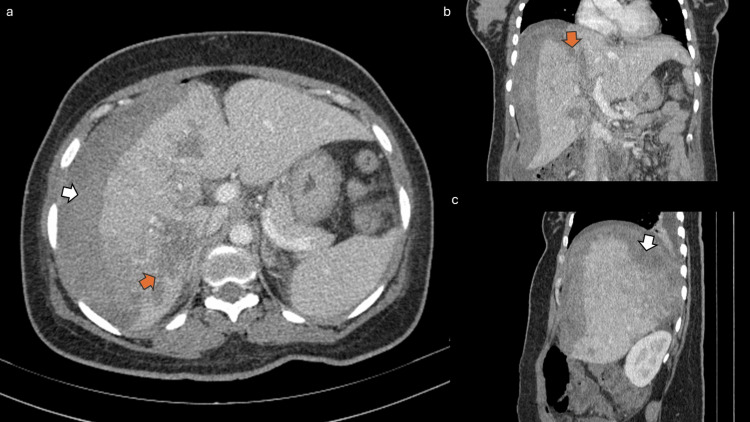 Figure 3
Figure 3 Figure 4
Figure 4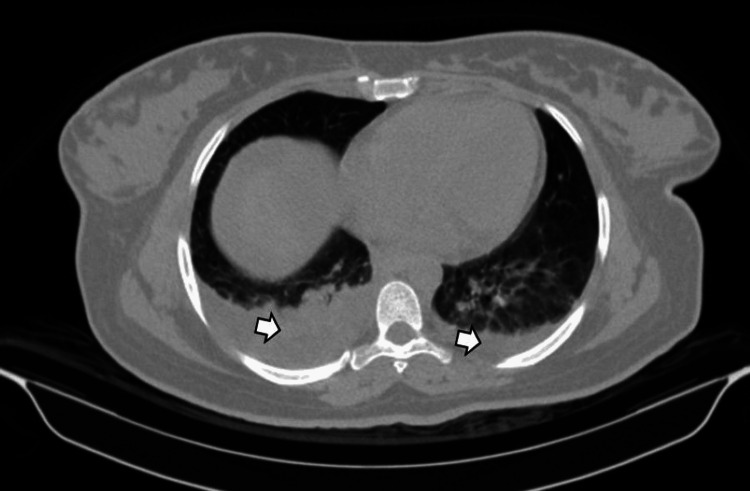 Figure 5
Figure 5 Figure 6
Figure 6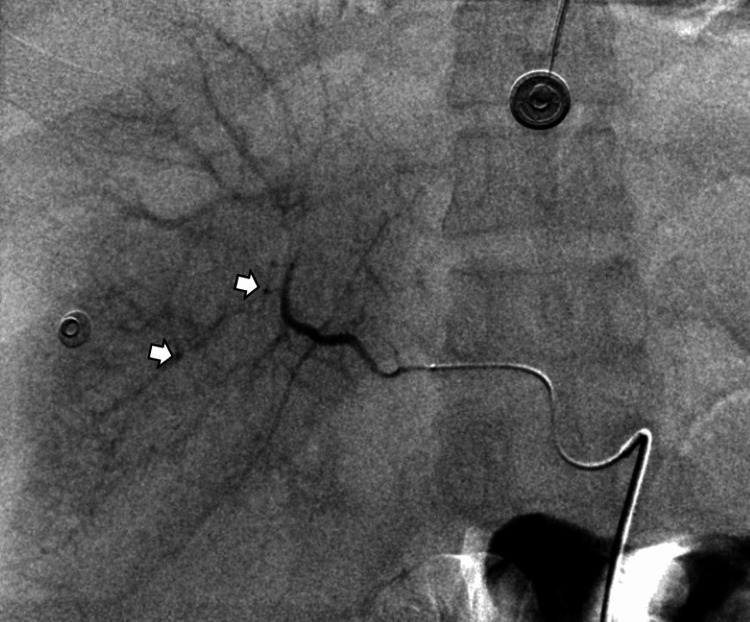 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Maternal and fetal healthcare · Organ Transplantation Techniques and Outcomes
Introduction
HELLP syndrome is a severe obstetric complication characterized by hemolysis, elevated liver enzymes, and low platelet count, often developing in the third trimester of pregnancy or in the postpartum period [1]. It can be seen in approximately 0.5%-0.9% of all pregnancies and in 10%-20% of patients with severe preeclampsia [1]. Diagnosis can be challenging due to its variable and often non-specific clinical presentation, frequently overlapping with other hypertensive disorders of pregnancy [2]. A particularly life-threatening complication of HELLP syndrome is subcapsular liver hematoma, which can rupture and lead to catastrophic hemorrhage and maternal mortality, historically reported at around 17%-59%, particularly when rupture occurs [2]. While most reported cases of ruptured hepatic subcapsular hematoma are managed surgically, transarterial embolization has emerged as a less invasive yet effective therapeutic option in select cases [2]. We report a case of HELLP syndrome complicated by a ruptured subcapsular liver hematoma successfully managed with transarterial embolization, emphasizing a multidisciplinary approach for optimal patient outcomes [1].
Case presentation
A 38-year-old woman with a medical history of type 2 diabetes mellitus was referred to the obstetric intensive care unit three days after a cesarean delivery complicated by eclampsia. She presented with severe right upper quadrant pain and malaise but no signs of hemodynamic shock. Laboratory investigations revealed severe thrombocytopenia, elevated liver enzymes, and biochemical hemolysis, consistent with HELLP syndrome in the postpartum period.
Abdominal ultrasonography revealed a well-defined heterogeneous subcapsular collection overlying the anterior, posterior, and right lateral aspects of the right hepatic lobe, measuring approximately 34 mm in maximal thickness, consistent with a subcapsular hematoma (Figure 1).
Abdominal ultrasonography showing a well-defined heterogeneous subcapsular collection (white arrow) over the anterior, posterior, and right lateral aspects of the right hepatic lobe, measuring approximately 34 mm in maximal thickness, consistent with a subcapsular hematoma.
The adjacent liver parenchyma appeared compressed with mild capsular bulging, and several poorly demarcated hypoechoic areas were identified within the right hepatic lobe, suggestive of hepatic infarctions. A moderate amount of free anechoic peritoneal fluid was also visualized in the hepatorenal recess, perisplenic space, and pelvis, consistent with reactive or hemorrhagic ascites (Figure 2).
Ultrasound image demonstrating moderate anechoic peritoneal effusion (white arrow) in the hepatorenal recess, consistent with reactive or hemorrhagic ascites.
The gallbladder and biliary tree appeared unremarkable, with no intrahepatic biliary dilatation or focal hepatic mass detected. Color Doppler evaluation demonstrated preserved main hepatic arterial and venous flows without evidence of pseudoaneurysm, thrombosis, or arteriovenous shunting.
Contrast-enhanced computed tomography of the abdomen and pelvis confirmed a heterogeneous hyperdense subcapsular hepatic hematoma on the right, measuring 34 mm in maximum thickness, without enhancement after contrast administration (Figure 3, white arrows).
Contrast-enhanced CT scan of the abdomen in axial (a), coronal (b), and sagittal (c) views revealing a heterogeneous subcapsular hepatic hematoma (white arrows) over the right hepatic lobe and multiple poorly defined hypodense areas of hepatic infarction (orange arrows).CT: computed tomography
Multiple poorly defined hypodense areas of hepatic infarction were also observed (Figure 3, orange arrows) in the right lobe. There was associated periportal, perivesicular, and mesenteric fat infiltration, as well as mild edema of the anterior abdominal wall with small air bubbles near the operative scar (Figure 4).
Sagittal contrast-enhanced CT image showing anterior abdominal wall edema and small postoperative air bubbles adjacent to the cesarean scar (white arrow).CT: computed tomography
Moderate effusion was present in the perihepatic, perisplenic, paracolic, and pelvic spaces. Bilateral pleural effusions with adjacent passive atelectasis were also noted (Figure 5).
Chest CT image demonstrating bilateral pleural effusions (white arrows) with adjacent passive atelectasis.CT: computed tomography
Given the high risk of hepatic rupture and hemodynamic deterioration, an urgent transcatheter hepatic artery embolization was undertaken. Vascular access was obtained via the right common femoral artery using the Seldinger technique under local anesthesia. A 5-French introducer sheath was placed, and a Cobra C2 catheter was advanced to perform selective catheterization of the celiac trunk and the proper hepatic artery under fluoroscopic guidance (Figure 6).
Fluoroscopic image showing selective catheterization of the proper hepatic artery using a Cobra C2 catheter with subtle vascular blush areas.
Subsequently, a 2.7-French microcatheter (Progreat®, Terumo, Tokyo, Japan) was coaxially introduced for superselective access to the right hepatic arterial branches. Angiography revealed a subtle focal vascular blush, confirming the site of arterial bleeding (Figure 7).
Fluoroscopic image showing selective catheterization of the proper hepatic artery using a Cobra C2 catheter with subtle vascular blush areas.
Embolization was carried out using 8 mL of 400-micron HydroPearl® microparticles (Terumo) until complete stasis of the targeted vessels was achieved. A final angiographic control confirmed cessation of extravasation and preservation of distal perfusion to unaffected hepatic territories. The procedure was completed without periprocedural complications in two hours, and hemodynamic stability was maintained throughout.
Postoperatively, the patient was monitored in the intensive care unit with hemodynamic stabilization, transfusion support, and correction of coagulopathy. Serial imaging and laboratory follow-up demonstrated progressive improvement with partial resorption of the hematoma and normalization of liver enzymes and platelet count. The patient recovered without the need for surgical intervention and was discharged in stable condition.
Discussion
Subcapsular hepatic hematoma in the setting of HELLP syndrome is a rare but serious complication occurring in approximately one in 100,000 pregnancies, often necessitating prompt and aggressive management due to its high maternal and fetal mortality rates [2]. Early detection and intervention are paramount for improving outcomes, as delayed management can lead to further complications such as intra-abdominal abscesses or pleural effusions [2,3]. Furthermore, the presence of hepatic infarction, as observed in this case, can exacerbate liver dysfunction and increase the risk of subsequent liver failure [4].
The underlying mechanism involves hepatic necrosis and rupture of the sinusoidal capillaries caused by pregnancy-induced hypertension, leading to hemorrhage within the liver parenchyma and beneath Glisson's capsule [3]. This intracapsular bleeding can expand, causing ischemic necrosis of the liver and potentially leading to capsular rupture and life-threatening hemoperitoneum [1].
Diagnosis relies on imaging modalities, with ultrasound providing initial detection and CT defining the extent, presence of rupture, and active bleeding [5,6]. Definitive identification of the bleeding site and active extravasation, crucial for guiding interventional procedures, is typically achieved through angiography [7]. In this context, transcatheter arterial embolization emerges as a minimally invasive yet highly effective treatment modality, particularly in hemodynamically stable patients, by selectively occluding the bleeding vessels [1].
Management depends on the severity of the condition, ranging from conservative observation to arterial embolization or surgery. When conservative measures fail or in cases of hemodynamic instability, surgical intervention, such as hepatic packing or liver resection, may be warranted to control bleeding and prevent further deterioration [6].
In our case, the presence of active bleeding warranted urgent embolization, which was performed successfully without complications. This approach effectively stabilized the patient, preventing the need for more invasive procedures like hepatic transplantation, which has been reported in cases where embolization contributed to worsening hepatic ischemia [1].
This technique demonstrates superior outcomes over surgical intervention, particularly for postpartum subcapsular hematoma, by minimizing blood loss and preserving liver parenchyma. The application of transcatheter arterial embolization is further supported by evidence suggesting its efficacy in achieving hemostasis and preventing rebleeding, thereby reducing the need for more aggressive surgical interventions [1].
Conclusions
In conclusion, this case highlights the critical role of timely diagnosis and interventional radiology in managing subcapsular hepatic hematoma associated with HELLP syndrome, offering a less invasive alternative to surgical approaches with favorable outcomes. It underscores the importance of a multidisciplinary approach, integrating obstetrics, critical care, and interventional radiology, to optimize patient management. Future research should focus on refining patient selection criteria for embolization versus surgical intervention to further improve outcomes and reduce morbidity associated with this rare but severe obstetric complication. Further investigation into optimal embolization techniques, including the choice of embolic agents and the extent of vessel occlusion, is also warranted to minimize the risk of post-embolization liver injury while ensuring effective hemorrhage control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liver bleeding due to HELLP syndrome treated with embolization and liver transplantation: a case report and review of the literature Front Surg Messina V Dondossola D Paleari MC 774702820213488128810.3389/fsurg.2021.774702 PMC 8646087 · doi ↗ · pubmed ↗
- 2Ruptured subcapsular liver hematoma: a rare complication of HELLP syndrome Libyan Int Med Univ J Alharam A Abuzalout T Elmehdawi H 606282023
- 3Subcapsular hepatic hematoma as a complication of severe preeclampsia: a case report J Med Case Rep Luhning K Mac Cormick H Macaulay B Saunders M Craig C 6251520213492075410.1186/s 13256-021-03166-w PMC 8684064 · doi ↗ · pubmed ↗
- 4Hepatic infarction induced by HELLP syndrome: a case report and review of the literature BMC Pregnancy Childbirth Guo Q Yang Z Guo J Zhang L Gao L Zhou B Shi Q 1911820182984830410.1186/s 12884-018-1799-9PMC 5977550 · doi ↗ · pubmed ↗
- 5Ruptured hepatic hematoma managed with a Sengstaken-Blakemore probe in severe preeclampsia with hemolysis, elevated liver enzymes, low platelets (HELLP) syndrome Cir Cir Vázquez-Rodríguez JG Vázquez-Arredondo JG 313488202010.24875/CIRU.1900130932963393 · doi ↗ · pubmed ↗
- 6Successful management of intraoperatively diagnosed ruptured spontaneous sub-capsular liver hematoma in a woman with preeclampsia Int J Womens Health Tegene D Regassa G Usu A Ayalew N 117511791320213487686010.2147/IJWH.S 333905 PMC 8643198 · doi ↗ · pubmed ↗
- 7Subcapsular hepatic hematoma: a case of chronic expanding hematoma of the liver BMC Gastroenterol Ono Y Kariya S Nakatani M 2412120213404478310.1186/s 12876-021-01775-9PMC 8161977 · doi ↗ · pubmed ↗