The relationship between perceived stress and depression in colorectal cancer patients: the mediating role of illness perception and the moderating role of self-efficacy
Fuzhuo Wang, Jiashuang Xu, Hong Sun, Xiuli Wang, Zhongguang Che, Ye Huang

TL;DR
This study explores how stress leads to depression in colorectal cancer patients, showing that illness perception mediates this link and self-efficacy plays a moderating role.
Contribution
The study reveals illness perception as a mediator and self-efficacy as a moderator in the stress-depression relationship among colorectal cancer patients.
Findings
Perceived stress is strongly correlated with depression in colorectal cancer patients.
Illness perception partially mediates the relationship between stress and depression.
Higher self-efficacy strengthens the link between perceived stress and illness perception.
Abstract
Numerous studies have demonstrated a close association between perceived stress and depression in colorectal cancer patients; however, the underlying mechanisms remain incompletely understood. This study aims to investigate the impact of perceived stress on depression in this population, as well as the mediating role of illness perception and the moderating role of self-efficacy. A cross-sectional design was employed. From May to November 2024, a questionnaire survey was conducted among 290 colorectal cancer patients at two Grade A tertiary hospitals in Shenyang and Jinzhou, Liaoning Province, China. The questionnaire comprised sections on general demographics, perceived stress, illness perception, self-efficacy, and depression. Descriptive statistics and correlation analyses were performed using SPSS 25.0 and the PROCESS 3.5 macro. Mediation and moderation effects were tested using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
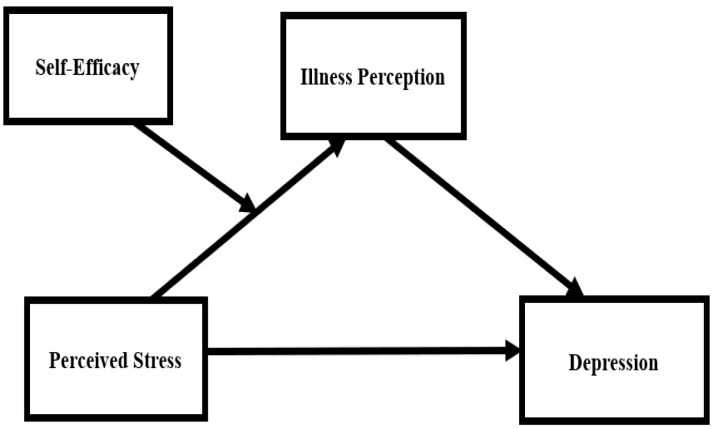 Figure 1
Figure 1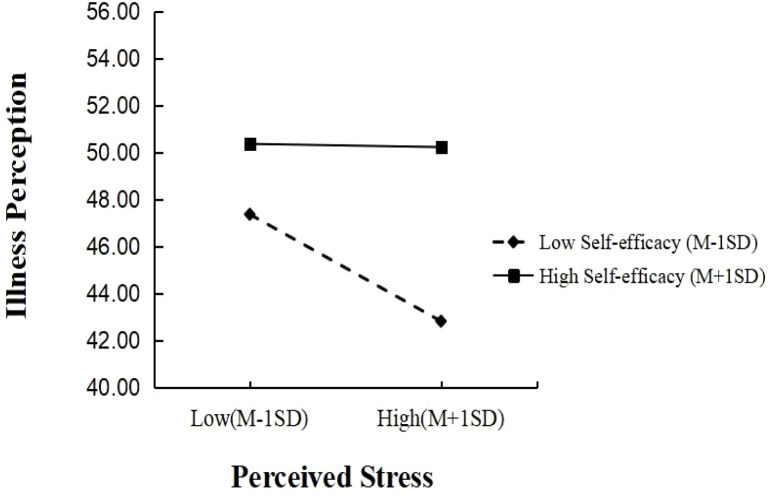 Figure 2
Figure 2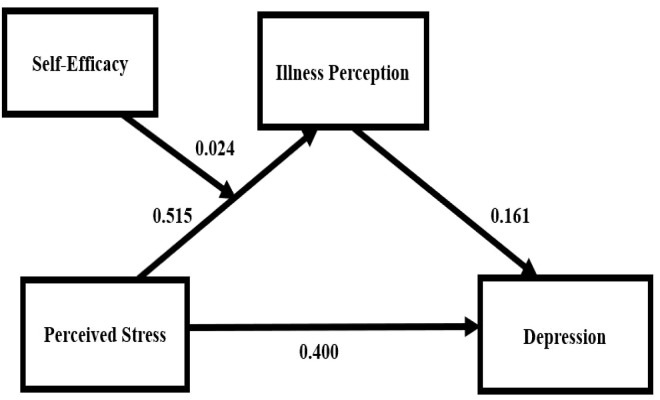 Figure 3
Figure 3| Variables | Group |
|
| ||
|---|---|---|---|---|---|
| Age | ≤44 | 42 (14.5) | 6.24 ± 4.08 | 2.306 | 0.001 |
| 45-59 | 84 (29.0) | 8.57 ± 4.86 | |||
| ≥60 | 164 (56.6) | 10.26 ± 4.17 | |||
| Gender | Male | 149 (51.40) | 10.07 ± 4.80 | 15.308 | <0.001 |
| Female | 141 (48.60) | 8.26 ± 4.15 | |||
| Educational level | Elementary school and below | 144 (49.7) | 10.37 ± 4.36 | 10.722 | <0.001 |
| Junior high school | 77 (26.6) | 9.00 ± 4.63 | |||
| High school or vocational school | 33 (11.4) | 7.88 ± 3.29 | |||
| College or above | 36 (12.4) | 6.06 ± 4.65 | |||
| Marital status | Unmarried | 13 (4.5) | 6.15 ± 5.06 | 3.955 | 0.009 |
| Married | 235 (81.0) | 9.06 ± 4.42 | |||
| Divorced | 8 (2.8) | 11.13 ± 5.30 | |||
| Widowed | 34 (11.7) | 10.79 ± 4.75 | |||
| Economic Status | Income falls short of expenses | 176 (60.7) | 9.27 ± 4.51 | 0.106 | 0.900 |
| Income and expenses are balanced | 85 (29.3) | 9.13 ± 4.48 | |||
| Income exceeds expenses | 29 (10) | 8.86 ± 5.39 | |||
| Residence | Rural | 81 (27.9) | 9.07 ± 4.85 | 0.067 | 0.796 |
| Urban | 209 (72.1) | 9.23 ± 4.48 | |||
| Hospitalization Count | 1 time | 144 (29.7) | 8.42 ± 3.42 | 0.067 | 0.796 |
| 2 times | 102 (35.2) | 10.83 ± 4.99 | |||
| 3 times | 26 (9.0) | 6.85 ± 5.53 | |||
| ≥4 times | 18 (6.2) | 9.33 ± 6.02 | |||
| Pathological Stage | I | 38 (13.1) | 7.45 ± 5.76 | 10.313 | <0.001 |
| II | 122 (42.1) | 8.38 ± 4.13 | |||
| III | 86 (29.7) | 9.59 ± 4.15 | |||
| IV | 44 (15.2) | 12.14 ± 4.08 |
| Variables | 1 | 2 | 3 | 4 | |
|---|---|---|---|---|---|
| Perceived stress | 29.56 ± 6.45 | 1 | |||
| Self-efficacy | 32.20 ± 7.15 | -0.617** | 1 | ||
| Illness perception | 29.33 ± 4.63 | 0.556** | -0.456** | 1 | |
| Depression | 9.19 ± 4.58 | 0.713** | -0.597** | 0.520** | 1 |
| Predictors | Depression | Perceived stress | Depression | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| SE |
| 95%CI |
| SE |
| 95%CI |
| SE |
| 95%CI | |
| Age | -0.576 | 0.349 | -1.648 | (-1.265, 0.112) | 1.693 | 0.532 | 3.182** | (0.646, 2.741) | -0.849 | 0.346 | -2.457* | (-1.530, -0.169) |
| Gender | -0.437 | 0.393 | -1.112 | (-1.211,0.337) | 2.501 | 0.598 | 4.182*** | (1.324, 3.678) | -0.840 | 0.393 | -2.136* | (-1.615, -0.069) |
| Educational level | -0.956 | 0.229 | -4.181*** | (-1.406, -0.506) | -0.083 | 0.348 | -0.239 | (-0.768, 0.602) | -0.943 | 0.222 | -4.244*** | (-1.379, -0.505) |
| Marital status | 0.108 | 0.281 | 0.386 | (-0.444, 0.661) | 0.014 | 0.427 | 0.033 | (-0.826, 0.855) | 0.106 | 0.273 | 0.389 | (-0.431, 0.643) |
| Hospitalization Count | 0.681 | 0.224 | 3.034** | (0.239, 1.122) | 1.301 | 0.341 | 3.813*** | (0.629, 1.973) | 0.471 | 0.223 | 2.107* | (0.031, 0.910) |
| Pathological staging | 0.201 | 0.219 | 0.917 | (-0.23, 0.631) | 1.218 | 0.333 | 3.659*** | (0.563, 1.873) | 0.004 | 0.217 | 0.019 | (-0.424,0.432) |
| Perceived stress | 0.483 | 0.032 | 14.887*** | (0.419,0.547) | 0.515 | 0.049 | 10.423*** | (0.417, 0.612) | 0.400 | 0.037 | 10.790*** | (0.327, 0.473) |
| Illness perception | 0.161 | 0.038 | 4.243*** | (0.087, 0.236) | ||||||||
|
| 0.746 | 0.685 | 0.763 | |||||||||
|
| 0.556 | 0.469 | 0.583 | |||||||||
|
| 50.428*** | 35.569*** | 49.03*** | |||||||||
| Effect | Effect value | SE | LLCI | ULCI | Effect ratio % |
|---|---|---|---|---|---|
| Total effect | 0.483 | 0.033 | 0.419 | 0.547 | 100 |
| Direct effect | |||||
| X→Y | 0.400 | 0.037 | 0.327 | 0.535 | 82.82 |
| Indirect effect | |||||
| X→M→Y | 0.083 | 0.026 | 0.036 | 0.137 | 17.18 |
| Variables | Illness perception | Depression | ||||||
|---|---|---|---|---|---|---|---|---|
|
| SE |
| 95%CI |
| SE |
| 95%CI | |
| Age | 1.398 | 0.519 | 2.693*** | (0.376, 2.420) | -0.849 | 0.346 | -2.457* | (-1.530, -0.169) |
| Gender | 2.413 | 0.579 | 4.170** | (1.274, 3.552) | -0.840 | 0.393 | -2.136* | (-1.614, -0.066) |
| Educational level | -0.199 | 0.337 | -0.589 | (-0.862, 0.465) | -0.943 | 0.222 | -4.244*** | (-1.379, -0.506) |
| Marital status | -0.161 | 0.414 | -0.389 | (-0.977, 0.654) | 0.106 | 0.273 | 0.389 | (-0.431, 0.643) |
| Hospitalization Count | 1.411 | 0.337 | 4.191*** | (0.748, 2.074) | 0.471 | 0.223 | 2.107* | (0.031, 0.910) |
| Pathological staging | 1.014 | 0.326 | 3.115** | (0.373, 1.655) | 0.004 | 0.217 | 0.019* | (-0.424, 0.432) |
| Perceived stress | 0.404 | 0.059 | 6.819*** | (0.287, 0.520) | 0.400 | 0.037 | 10.787*** | (0.327, 0.473) |
| Self-efficacy | -0.164 | 0.054 | -3.05** | (-0.269, -0.058) | ||||
| Perceived stress* | 0.024 | 0.006 | 4.207*** | (0.287, 0.520) | ||||
|
| 0.713 | 0.763 | ||||||
|
| 0.508 | 0.583 | ||||||
|
| 32.125 | 49.034 | ||||||
| Self-efficacy | Effect | SE | LLCI | ULCI |
|---|---|---|---|---|
| M-1SD | 0.233 | 0.077 | 0.081 | 0.384 |
| M | 0.403 | 0.059 | 0.287 | 0.520 |
| M+1SD | 0.575 | 0.066 | 0.444 | 0.705 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Stoma care and complications · Music Therapy and Health
Introduction
Colorectal cancer, one of the most prevalent malignant tumors worldwide, imposes not only physical burdens but also significantly impacts patients’ mental health throughout diagnosis and treatment (1, 2). Depression, the most common psychological disorder among colorectal cancer patients (3), leads to symptoms such as low mood, loss of interest, sleep disturbances, and decreased appetite (4). Depression in these patients is associated with poorer treatment outcomes and prognosis, and constitutes a significant risk factor for suicidal ideation and behavior (5, 6). Therefore, investigating the factors influencing depression and their underlying mechanisms in colorectal cancer patients is clinically important for developing targeted psychological interventions, improving psychological well-being, and enhancing prognosis.
Perceived stress refers to an individual’s subjective experience resulting from the appraisal of environmental stressors, reflecting a perceived imbalance between situational demands and coping capacity (7). Substantial evidence confirms that perceived stress is prevalent among cancer patients and serves as a strong predictor of depression (8, 9). This association has been consistently observed in colorectal cancer populations across both cross-sectional and longitudinal studies (10–12). Despite this established link, the psychological mechanisms remain poorly understood.
Illness perception, defined as the cognitive representation of illness shaped by personal experience and knowledge (13), is a key factor influencing self-management, emotional adjustment, and clinical outcomes (14). Negative illness perception is closely associated with greater psychological distress, including anxiety and depression (15–17). Furthermore, perceived stress has been identified as a significant antecedent of negative illness perception (18, 19). To theoretically construct this relationship, we draw on Leventhal’s Common-Sense Model of Self-Regulation (CSM) (20). The CSM is a dynamic framework explaining how individuals cope with health threats. Its core components include: cognitive representation (the individual’s understanding of the illness’s identity, cause, timeline, consequences, and controllability), emotional representation (emotional responses triggered by illness cognition), and a coping process involving primary appraisal (threat judgment) and secondary appraisal (coping resource evaluation). In this context, perceived stress among colorectal cancer patients can be viewed as the outcome of primary appraisal within the CSM. Through secondary appraisal, which integrates personal experience and medical information, patients are prone to form negative illness perception (e.g., perceiving severe consequences, a long timeline, and low controllability of the illness). These perception tendencies are, in turn, associated with depression. Therefore, from the CSM theoretical perspective, illness perception constitutes a plausible cognitive pathway through which perceived stress influences depression.
Meanwhile, according to Bandura’s Social Cognitive Theory (21), self-efficacy (defined as an individual’s belief in their ability to cope) (19) is considered a key moderating variable in cognitive processing under stress. A central tenet of this theory posits that self-efficacy actively shapes the cognitive adaptation process by influencing the individual’s appraisal frame and interpretative style toward stressful events. Specifically, high self-efficacy may prompt individuals to appraise perceived stress as a “manageable challenge,” thereby initiating a series of adaptive cognitive processes (such as actively seeking information and engaging in rational reappraisal). This proactive, in-depth processing is expected to strengthen the association between perceived stress and illness perception (22). Conversely, low self-efficacy tends to lead to an appraisal of “uncontrollable threat,” which can trigger catastrophizing interpretations, thereby weakening the link between perceived stress and illness perception (23). Hence, this study proposes that self-efficacy may play a positive moderating role in the relationship between perceived stress and illness perception; that is, higher levels of self-efficacy are likely to strengthen the effect of perceived stress on illness perception.
In summary, this study innovatively integrates the Common-Sense Model of Self-Regulation and Social Cognitive Theory to construct a moderated mediation model (Figure 1), aiming to systematically examine the following two hypotheses: (1) Illness perception mediates the relationship between perceived stress and depression; and (2) Self-efficacy positively moderates the pathway from perceived stress to illness perception. The implementation of this research is expected to provide a novel perspective for uncovering the psychological mechanisms underlying depressive symptoms in colorectal cancer patients, as well as a theoretical basis for developing multidimensional intervention programs that integrate stress management, cognitive restructuring, and efficacy enhancement.
The hypothesized moderated mediation model.
Methods
Study design and setting
This study employed a cross-sectional design. Data collection took place from May to November 2024 at two Grade-A tertiary hospitals in Liaoning Province, China.
Participants and sampling
A multistage stratified random sampling method was used. Inclusion criteria were: (1) diagnosis of colorectal cancer confirmed by clinical pathology; (2) voluntary provision of informed consent; (3) clear consciousness and adequate communication ability; (4) age ≥18 years. Exclusion criteria were: (1) critically ill patients unable to complete the process; (2) clinically assessed life expectancy of less than 6 months; (3) presence of cognitive impairment or diagnosed psychiatric disorders; (4) history of psychological interventions that could interfere with study outcomes; (5) individuals unaware of their diagnosis.
Sampling procedure
The sampling procedure consisted of three stages. Stage 1: Within Liaoning Province, eight Grade III Class A hospitals with specialized oncology departments were selected based on national rankings. Using hospital primary specialty as the stratification variable and a random number table, Dalian University of Technology Affiliated Cancer Hospital and Jinzhou Medical University Affiliated Hospital were selected (sampling proportion 25%). Stage 2: Within each hospital, departments admitting colorectal cancer patients were listed and stratified by primary treatment modality. Using random number tables, selected departments were: Dalian University of Technology Affiliated Cancer Hospital: Colorectal Surgery Wards 5 and 6, Department of Integrated Traditional and Western Medicine; Jinzhou Medical University Affiliated Hospital: General Surgery Colorectal Wards 1 and 3, Oncology Department. Stage 3: Researchers visited selected departments weekly. Eligible patients were screened from the daily inpatient lists. Systematic random sampling was applied: eligible patients were listed by bed number, a random starting point was determined, and every other patient (k=2) was invited. This ensured approximately 50% systematic sampling of daily eligible patients, enabling efficient recruitment while maintaining randomness.
Sample size estimation
Sample size was determined using a dual approach. First, based on the factor analysis guideline of 10–20 participants per scale dimension, and considering the 7 dimensions across the scales used in this study, a preliminary sample size estimate ranged from 70 to 140 (24). Second, an a priori power analysis was conducted using G*Power 3.1.9.4 software. Specifically, we selected the statistical test “F-test—Linear Multiple Regression: Fixed Model, R² Deviates from Zero.” The analysis targeted the hypothesized moderated mediation model, which included 12 predictor variables (8 demographic variables, perceived stress, illness perception, self-efficacy, and their interaction term). Parameters were set as α = 0.05 (two-tailed), statistical power = 0.95, and a medium effect size (f² = 0.15) (25). This calculation yielded a minimum required sample size of 221. Accounting for an estimated 20% rate of invalid questionnaires or attrition, the target sample size was adjusted to 277 [221/(1-0.20)]. In practice, to ensure data quality and representation, the scope of recruitment was expanded. A total of 319 questionnaires were distributed, and 290 valid questionnaires were ultimately retained (159 from Dalian University of Technology Affiliated Cancer Hospital and 131 from Jinzhou Medical University Affiliated Hospital), resulting in a valid response rate of 90.91%.
Data collection procedure
Before data collection, all research personnel completed a standardized training program (26–28). Standardized training refers to structured, uniform training procedures implemented for all research personnel to ensure the consistency, accuracy, and reliability of research data. The program consisted of two key modules: (1) scoring criteria and tool familiarization to ensure consistent understanding of the measurement tools (Perceived Stress Scale, Self-Efficacy Scale, Illness Perception Scale, and Depression Scale) and their scoring protocols; and (2) patient-centered communication skills, focusing on techniques for building rapport, delivering clear and neutral instructions, and creating a supportive environment to facilitate honest and accurate responses.
Ethical considerations
This study was approved by the Research Ethics Committee of Jinzhou Medical University (Approval No. JZMULL2023029). All procedures were in accordance with the ethical standards of the institutional committee and the Declaration of Helsinki. Written informed consent was obtained from all participants.
Instruments
General demographic characteristics questionnaire
This questionnaire followed commonly used standards in psychosocial research (29), covering age, gender, education, marital status, economic status, residence, hospitalization count, and tumor staging. Categories were defined as follows: Age (≤44, 45-59, ≥60 years); Gender (male, female); Education (elementary school or below, junior high school, high school/vocational school, college or above); Marital status (unmarried, married, divorced, widowed); Economic status (below means, balanced, surplus); Residence (rural, urban); Hospitalization count (1, 2, 3, ≥4 times); Tumor stage (I, II, III, IV).
Perceived stress scale
The 14-item Perceived Stress Scale by Cohen et al. (1983) (30) comprises two dimensions: tension and helplessness. Items are rated on a 5-point Likert scale (0=“Never” to 4=“Very much”). Seven items are reverse-scored. Total scores range from 0-56, categorized as mild (0-28), moderate (29-42), or excessive (43-56) perceived stress. In this study, Cronbach’s α was 0.814, and KMO = 0.648.
Self-efficacy scale
The 10-item General Self-Efficacy Scale by Schwarzer et al. (1992) (31) uses a 5-point Likert scale (1=“Disagree” to 5=“Strongly Agree”). Total scores range from 10-50, categorized as low (<25), moderate (25-37), or high (>37) self-efficacy. In this study, Cronbach’s α was 0.935, KMO = 0.936.
Illness perception scale
The Brief Illness Perception Questionnaire by Broadbent et al. (2006) (32) consists of 9 items across three dimensions: disease cognition, emotion, and comprehension. Item 9 is open-ended and not scored. The first 8 items are rated on a 0–10 scale (three reverse-scored), yielding a total score of 0-80. Higher scores indicate stronger negative perceptions. In this study, Cronbach’s α was 0.752, KMO = 0.713.
Depression scale
The 9-item Patient Health Questionnaire (PHQ-9) by Kroenke et al. (2001) (33) uses a 4-point scale (0=“Not at all” to 3=“Nearly every day”). Total scores range from 0-27, categorized as: 0-4 (none), 5-9 (mild), 10-14 (moderate), 15-19 (moderately severe), 20-27 (severe). In this study, Cronbach’s α was 0.875, KMO = 0.891.
Statistical analysis
Data analysis was conducted using IBM SPSS Statistics 25.0 and the PROCESS macro version 3.5. Normality of continuous variables was assessed via the Kolmogorov-Smirnov test; all variables were normally distributed (P > 0.05). Descriptive statistics included frequencies/percentages for categorical variables and mean ± standard deviation for continuous variables. Independent samples t-tests and one-way ANOVA were used to examine differences in depression scores across demographics. Pearson correlation analysis evaluated associations among study variables. Moderated mediation analysis was performed using PROCESS macro 3.5 (Model 14 for moderation, Model 4 for mediation). Effects were examined using bootstrap resampling (5,000 samples) to generate 95% bias-corrected confidence intervals (CI). A two-tailed P < 0.05 was considered statistically significant.
Results
Descriptive statistics
Table 1 presents demographic characteristics and univariate analysis. Participants’ mean age was 59.58 ± 13.09 years (range 19-90). The sample comprised 149 males (51.4%) and 141 females (48.6%). Most were married (81.0%). Univariate analysis revealed significant associations between depression and age, gender, education level, marital status, hospitalization count, and pathological stage (P < 0.05). These variables were retained as covariates in subsequent analyses.
Correlations between variables
As shown in Table 2, perceived stress was negatively correlated with self-efficacy and positively correlated with illness perception and depression (P < 0.01). Self-efficacy was negatively correlated with illness perception and depression (P < 0.01). Illness perception was positively correlated with depression (P < 0.01). Mean scores were: perceived stress 29.56 ± 6.45, self-efficacy 32.20 ± 7.15, illness perception 29.33 ± 4.63, depression 9.19 ± 4.58.
Mediation analysis
As shown in Table 3, after controlling for covariates, mediation analysis (PROCESS Model 4) indicated a significant positive correlation between perceived stress and depression (β = 0.483, P < 0.001). When illness perception was introduced as a mediator, the direct effect remained significant (β = 0.400, P < 0.001). Perceived stress was positively correlated with illness perception (β = 0.515, P < 0.001), and illness perception was positively correlated with depression (β = 0.161, P < 0.001). The indirect effect was significant (B = 0.083, SE = 0.026, 95% CI = [0.036, 0.137]), indicating partial mediation. The mediating effect accounted for 17.18% of the total effect (Table 4).
Moderated mediation analysis
Moderated mediation analysis (PROCESS Model 14) was conducted, controlling for covariates. As shown in Table 5, the interaction term between perceived stress and self-efficacy was positively correlated with illness perception (B = 0.024, P < 0.001), indicating that self-efficacy moderated the “perceived stress → illness perception” pathway.
To illustrate this moderation, self-efficacy was categorized into three levels (low: M - 1SD; medium: M; high: M + 1SD). Simple slope analysis (Table 6; Figure 2) showed that among participants with low self-efficacy, perceived stress significantly positively predicted illness perception (B = 0.233, SE = 0.077, t = 3.026, P < 0.01). This positive predictive effect was stronger among participants with high self-efficacy (B = 0.575, SE = 0.066, t = 8.655, P < 0.001).
Plot of the relationship between perceived stress and illness perception at two levels of self-efficacy.
Summary of main findings
Overall, perceived stress directly influenced depression and indirectly affected it through illness perception. Self-efficacy moderated the “perceived stress → illness perception” pathway (Figure 3).
Moderated mediation model.
Discussion
This study found a significant positive correlation between perceived stress and depression in colorectal cancer patients, consistent with existing literature (34). This relationship may arise from the physical toll of diagnosis and treatments (e.g., surgery, chemotherapy), which deplete patients’ resources and likely intensify perceived stress (35). Mechanistically, from a mechanistic perspective, persistent perceived stress may be associated with depression through dual pathways: physiologically, chronic stress can activate the HPA axis, dysregulate stress hormones (e.g., cortisol), and disturb neurotransmitter balance (e.g., serotonin, dopamine)—processes associated with depression (36). Psychologically, high perceived stress often coincides with feelings of helplessness and drains emotional regulation capacity, hindering adaptive coping with negative affect, which may cumulatively contribute to depression (37). Thus, implementing individualized care focused on reducing perceived stress is recommended as a supportive component of depression prevention and management in this population.
The study also found that illness perception mediates the relationship between perceived stress and depression, consistent with the theoretical framework of Leventhal’s Common-Sense Model of Self-Regulation (20). This model proposes that individuals undergo a cognitive-emotional process of “primary appraisal—secondary appraisal—emotional response” when coping with illness. Colorectal cancer patients face multiple stressors, including diagnostic shock, treatment trauma, recurrence risk, and financial burden (38). These are perceived as stress during primary appraisal, triggering secondary appraisal and forming cognitive representations of disease etiology, progression, and consequences (i.e., illness perception) (39). Negative illness perception may be associated with negative emotions through two pathways: first, by reinforcing the cognitive bias of “stress uncontrollability,” linking to depressive emotional responses; second, by prompting passive coping strategies like avoidance, which diminish the protective effect of social support and may thus correlate with depression (40, 41).
Further analysis indicates that self-efficacy moderates the relationship between perceived stress and illness perception. pathway, and social cognitive theory contributes to a richer understanding of this process (21). Patients with high self-efficacy exhibit greater confidence in their ability to cope with illness, tending to evaluate perceived stress as “manageable challenges.” Consequently, they proactively seek illness information and rationally assess treatment options, facilitating the transformation of stress into clear, controllable illness perception. This results in a stronger association between stress and cognition (42, 43). In contrast, patients with low self-efficacy, lacking confidence in coping, are prone to cognitive avoidance under stress. Stress-related information fails to fully integrate into their illness perception, resulting in a relatively weaker association between the two (44, 45). Consequently, future intervention programs may prioritize enhancing patients’ self-efficacy as a core objective. This can be achieved through setting phased, attainable behavioral goals, providing skill practice, and offering feedback on successful experiences. Such interventions help patients develop more adaptive stress coping and illness perception patterns, potentially yielding positive impacts on their mental health.
Limitations
This study has several limitations. First, the cross-sectional design can only reveal correlations between variables and cannot infer causal directionality. Future longitudinal or experimental studies may be conducted to further validate the temporal sequence and causal relationships among variables. Second, the sample originates from two hospitals within the same province, potentially limiting the representativeness of the results. Subsequent research may expand the sampling scope to enhance external validity. Additionally, all data were collected through self-reported questionnaires, potentially subject to social desirability and recall bias. Future studies should integrate multi-source data, such as physiological indicators and clinical assessments, to enhance measurement objectivity and strengthen the robustness of conclusions.
Implication
Based on the moderated mediation model established in this study, a multidimensional psychological support program for colorectal cancer patients should be designed across three levels: First, integrate the Brief Perceived Stress Scale, the Illness Perception Questionnaire, and the General Self-Efficacy Scale into routine care for systematic screening. Patients can be categorized based on assessment results to inform subsequent support program development (46, 47). Second, for patients with elevated perceived stress levels, structured programs such as mindfulness-based stress reduction training and relaxation technique instruction should be offered. Patients with negative illness perception may benefit from visual disease education and cognitive restructuring dialogues to foster more adaptive illness understanding. Those with low self-efficacy can participate in symptom management skill workshops and peer experience-sharing groups, providing platforms for learning and exchange (48). Third, establish a multidisciplinary collaboration mechanism involving healthcare providers and mental health professionals. Integrate digital health tools (e.g., health education apps, mood diary mini-programs) as extensions of in-hospital support. Implement regular follow-up protocols to tailor support content according to patients’ conditions at different treatment stages (49, 50). These comprehensive measures will help build a more holistic support system, thereby playing a positive role in reducing depression risk among colorectal cancer patients.
Conclusions
Overall, this study indicates that illness perception partially mediates the relationship between perceived stress and depression in colorectal cancer patients, while self-efficacy moderates the association between perceived stress and illness perception. These findings highlight the interconnectedness of perceived stress, illness perception, and self-efficacy with depression in colorectal cancer patients. Therefore, developing targeted interventions may represent a crucial direction for supporting the mental health of colorectal cancer patients in future research and clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dekker E Tanis PJ Vleugels JLA Kasi PM Wallace MB . Colorectal cancer. Lancet. (2019) 394:1467–80. doi: 10.1016/S 0140-6736(19)32319-0, PMID: 31631858 · doi ↗ · pubmed ↗
- 2Abedizadeh R Majidi F Khorasani HR Abedi H Sabour D . Colorectal cancer: a comprehensive review of carcinogenesis, diagnosis, and novel strategies for classified treatments. Cancer Metast Rev. (2024) 43:729–53. doi: 10.1007/s 10555-023-10158-3, PMID: 38112903 · doi ↗ · pubmed ↗
- 3Cheng V Oveisi N Mc Taggart-Cowan H Loree JM Murphy RA De Vera MA . Colorectal cancer and onset of anxiety and depression: A systematic review and meta-analysis. Curr Oncol. (2022) 29:8751–66. doi: 10.3390/curroncol 29110689, PMID: 36421342 PMC 9689519 · doi ↗ · pubmed ↗
- 4Song L Su Z He Y Pang Y Zhou Y Wang Y . Association between anxiety, depression, and symptom burden in patients with advanced colorectal cancer: A multicenter cross-sectional study. Cancer Med. (2024) 13:e 7330. doi: 10.1002/cam 4.7330, PMID: 38845478 PMC 11157164 · doi ↗ · pubmed ↗
- 5Xia S Zhu Y Luo L Wu W Ma L Yu L . Prognostic value of depression and anxiety on colorectal cancer-related mortality: a systematic review and meta-analysis based on univariate and multivariate data. Int J Colorect Dis. (2024) 39:45. doi: 10.1007/s 00384-024-04619-6, PMID: 38563889 PMC 10987367 · doi ↗ · pubmed ↗
- 6Conejero I OliéE Calati R Ducasse D Courtet P . Psychological pain, depression, and suicide: recent evidences and future directions. Curr Psychiatry Rep. (2018) 20:33. doi: 10.1007/s 11920-018-0893-z, PMID: 29623441 · doi ↗ · pubmed ↗
- 7Rueggeberg R Wrosch C Miller GE . The different roles of perceived stress in the association between older adults’ physical activity and physical health. Health Psychol. (2012) 31:164–71. doi: 10.1037/a 0025242, PMID: 21875206 PMC 3279628 · doi ↗ · pubmed ↗
- 8Kreitler S Peleg D Ehrenfeld M . Stress, self-efficacy and quality of life in cancer patients. Psycho-Oncology. (2007) 16:329–41. doi: 10.1002/pon.1063, PMID: 16888704 · doi ↗ · pubmed ↗