Comparative Outcomes Between Black and White Patients With Early‐Stage Diffuse Large B‐Cell Lymphoma
María Herrán, Sindu Iska, Hong Liang, Ludovic Saba, Chakra P. Chaulagain, Chieh‐Lin Fu

TL;DR
This study found no significant survival difference between Black and White patients with early-stage diffuse large B-cell lymphoma, despite existing socioclinical disparities.
Contribution
The study reveals that race does not significantly affect survival in early-stage DLBCL when controlling for other factors.
Findings
Black and White patients with early-stage DLBCL had similar survival rates (HR 0.98, p=0.5263).
Socioclinical factors like age, comorbidities, and income were significant predictors of mortality.
Survival disparities between races are likely linked to advanced-stage DLBCL rather than early-stage disease.
Abstract
Determinants of survival in DLBCL stage I–IV collectively have reported Black patients and advanced stage to have worse outcomes on multivariate analysis. As advanced stage is a factor in outcome, available data have not focused on early‐stage DLBCL to evaluate the impact of race and SES on outcome. To address this research gap, the study aims to examine and compare the characteristics and the determinants of survival between US Black and White patients with early‐stage (I–II) DLBCL. A retrospective NCDB analysis of early‐stage DLBCL patients was conducted, comparing sociodemographic, clinical, and treatment factors between Black and White groups. Chi‐square tests assessed differences. Multivariate Cox regression identified survival predictors. Matched patient pairs were analyzed using Cox models with robust variance, and Kaplan–Meier curves evaluated survival outcomes by race. 81,430…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
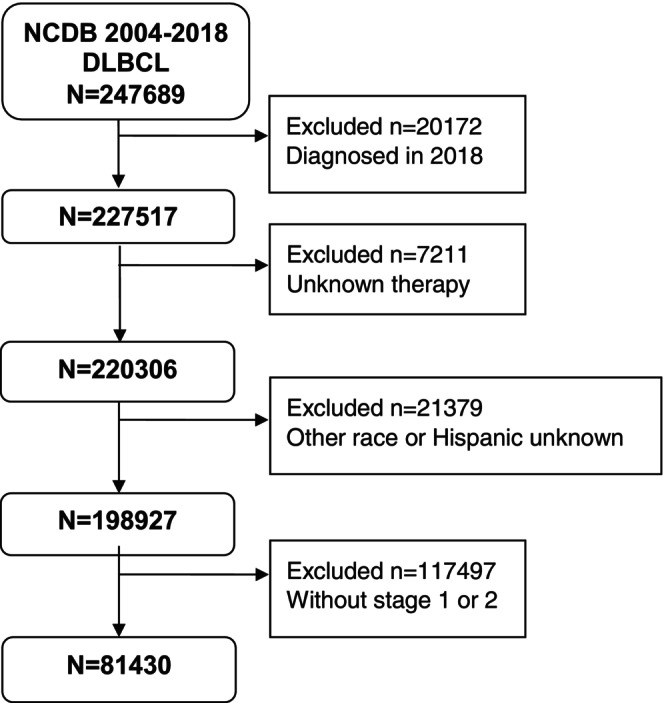 FIGURE 1
FIGURE 1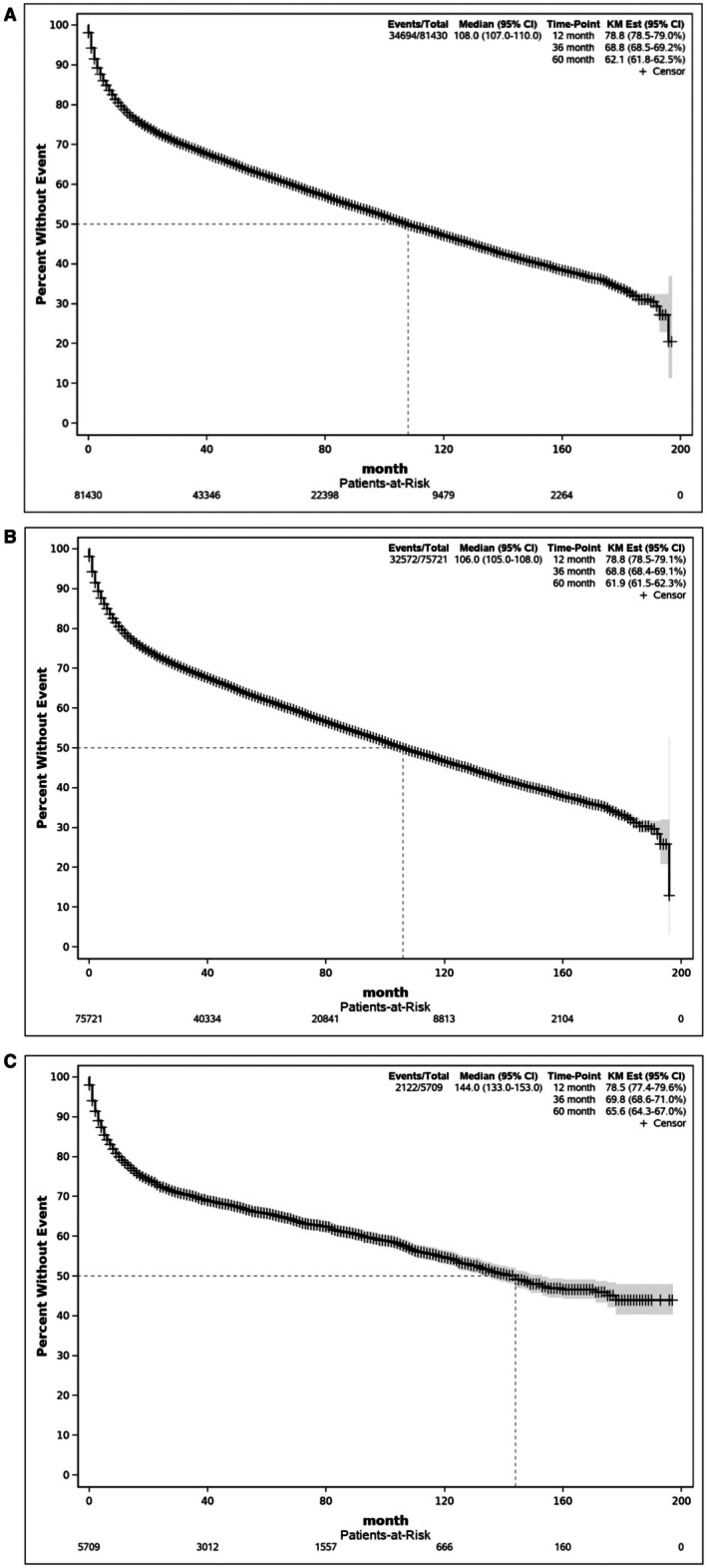 FIGURE 2
FIGURE 2| Variable | All Patients | Case‐Matched Patients | |||
|---|---|---|---|---|---|
| White ( | Black ( |
| White ( | Black ( | |
| Age, median (IQR) | 68.0 (56.0–78.0) | 56.0 (43.0–68.0) | < 0.0001 | ||
| Age | |||||
| Male, | 40,703 (53.0) | 2,949 (51.7) | 0.0022 | 611 (48.8) | 611 (48.8) |
| Hispanic, | 5,596 (7.4) | 76 (1.3) | 0.0022 | 4 (0.32) | 4 (0.32) |
| Education | |||||
| < 7.0% | 19,006 (25.1) | 530 (9.3) | < 0.0001 | 210 (16.8) | 210 (16.8) |
| 7.0%–12.9% | 24,068 (31.8) | 1,132 (19.8) | 369 (29.4) | 369 (29.4) | |
| 13.0%–20.9% | 16,484 (21.8) | 1,824 (31.9) | 390 (31.1) | 390 (31.1) | |
| > 21.0% | 10,104 (13.3) | 1,722 (30.2) | 284 (22.7) | 284 (22.7) | |
| NA | 6,063 (8.0) | 501 (8.8) | |||
| Median household income, | 0.0001 | ||||
| < 38,000 | 9,478 (12.5) | 2,040 (35.7) | 358 (28.6) | 358 (28.6) | |
| 38,000–47,000 | 16,181 (21.4) | 1,182 (20.7) | 264 (21.1) | 264 (29.1) | |
| 48,000–62,000 | 19,265 (25.4) | 1,059 (18.6) | 285 (22.7) | 285 (22.7) | |
| > 63,000 | 24,697 (32.6) | 923 (16.2) | 346 (27.6) | 346 (27.6) | |
| NA | 6,100 (8.1) | 505 (8.8) | |||
| Insurance status, | |||||
| Private | 27,672 (36.5) | 2,252 (39.4) | < 0.0001 | 547 (43.7) | 547 (43.7) |
| Medicare | 40,339 (53.3) | 1,884 (33.0) | 645 (51.5) | 645 (51.5) | |
| Medicaid/Other | 4,191 (5.5) | 979 (17.2) | 6 (0.5) | 6 (0.5) | |
| Not‐insured | 2,164 (2.9) | 447 (7.8) | 17 (1.3) | 17 (1.3) | |
| Unknown | 1,355 (1.8) | 147 (2.6) | 38 (3.0) | 38 (3.0) | |
| Year of diagnosis, | 0.0527 | ||||
| 2004–2007 | 17,411 (23.0) | 1,257 (22.0) | 252 (20.1) | 252 (20.1) | |
| 2008–2011 | 20,885 (27.6) | 1,539 (27.0) | 420 (33.5) | 420 (33.5) | |
| 2012–2014 | 18,162 (24.0) | 1,453 (25.4) | 254 (20.3) | 254 (20.3) | |
| 2015–2017 | 19,263 (25.4) | 1,460 (25.6) | 327 (26.1) | 327 (26.1) | |
| Charlson‐Deyo Score, | |||||
| 0 | 56,847 (75.1) | 4,076 (71.4) | < 0.0001 | 1,077 (86.0) | 1,077 (86.0) |
| 1 | 12,491 (16.5) | 873 (15.3) | 129 (10.3) | 129 (10.3) | |
| ≥ 2 | 6,383 (8.4) | 760 (13.3) | 47 (3.7) | 47 (3.7) | |
| Stage, | < 0.0001 | ||||
| 1 | 43,962 (58.1) | 3,100 (54.3) | 731 (58.3) | 731 (58.3) | |
| 2 | 31,759 (41.9) | 2,609 (45.7) | 522 (41.7) | 522 (41.7) | |
| HIV, | |||||
| Positive | 1,304 (1.7) | 753 (13.2) | < 0.0001 | 10 (0.8) | 10 (0.8) |
| Negative | 43,177 (57.0) | 3,170 (55.5) | 847 (67.6) | 847 (67.6) | |
| NA | 31,240 (41.3) | 1,786 (31.3) | 396 (31.6) | 396 (31.6) | |
| B symptoms, | < 0.0001 | ||||
| B symptoms | 13,313 (17.6) | 1,402 (24.6) | 147 (11.7) | 147 (11.7) | |
| No B symptoms | 56,634 (70.8) | 3,577 (62.6) | 1,025 (81.8) | 1,025 (81.8) | |
| Unknown | 8,774 (11.6) | 730 (12.8) | 81 (6.5) | 81 (6.5) | |
| Chemotherapy, | 0.0026 | ||||
| Multi‐agent | 54,816 (72.4) | 4,047 (70.9) | 980 (78.2) | 980 (78.2) | |
| Single/unknown agent | 6,872 (9.1) | 499 (8.7) | 47 (3.8) | 47 (3.8) | |
| Not administered | 14,033 (18.5) | 1,163 (20.4) | 226 (18.0) | 226 (18.0) | |
| Hormone therapy, | 33,438 (44.2) | 2,300 (40.3) | < 0.0001 | 565 (45.1) | 565 (45.1) |
| Immunotherapy, | 22,893 (30.2) | 1,604 (28.1) | 0.0007 | 359 (28.7) | 359 (28.7) |
| Variable | HR (95% CI) |
|
|---|---|---|
| Age (≥ 60 vs. < 60) | 2.04 (1.96–2.12) | < 0.0001 |
| Gender (male vs. female) | 1.09 (1.06–1.11) | < 0.0001 |
| Hispanic (yes vs. no) | 0.84 (0.80–0.89) | < 0.0001 |
| Median household income | ||
| < 38,000 | 1.18 (1.14–1.22) | < 0.0001 |
| 38,000 – 47,000 | 1.14 (1.11–1.18) | < 0.0001 |
| 48,000 – 62,000 | 1.13 (1.10–1.16) | < 0.0001 |
| > 63,000 (Ref.) | 1 | — |
| Unknown | 1.25 (0.95–1.64) | 0.1174 |
| Insurance | ||
| Private (Ref.) | 1 | — |
| Medicare | 1.79 (1.73–1.84) | < 0.0001 |
| Medicaid | 1.55 (1.46–1.63) | < 0.0001 |
| Uninsured | 1.31 (1.21–1.42) | < 0.0001 |
| Unknown | 1.34 (1.23–1.46) | < 0.0001 |
| Year of diagnosis | ||
| 2004–2007 | 0.99 (0.95–1.03) | 0.5984 |
| 2008–2011 | 0.95 (0.91–0.99) | 0.0102 |
| 2012–2014 | 1.01 (0.97–1.05) | 0.6187 |
| 2015–2017 (Ref.) | 1 | — |
| Distance traveled (miles) | ||
| < 10 (Ref.) | 1 | |
| 10–23 | 0.93 (0.90–0.96) | < 0.0001 |
| > 23 | 0.96 (0.94–0.99) | 0.0059 |
| Facility type | ||
| Academic (Ref.) | 1 | — |
| Non‐academic | 1.00 (0.98–1.03) | 0.9829 |
| Unknown | 0.52 (0.48–0.56) | < 0.0001 |
| CDC | ||
| 0 (Ref.) | 1 | — |
| 1 | 1.37 (1.33–1.41) | < 0.0001 |
| ≥ 2 | 1.92 (1.85–1.98) | < 0.0001 |
| Stage | ||
| 1 (Ref.) | 1 | |
| 2 | 1.16 (1.13–1.18) | < 0.0001 |
| HIV | ||
| Negative | 1 | |
| Positive | 1.59 (1.48–1.70) | < 0.0001 |
| Unknown | 1.03 (1.01–1.05) | 0.0093 |
| B symptoms | ||
| No B symptoms (Ref.) | 1 | |
| B symptoms | 1.23 (1.20–1.27) | < 0.0001 |
| Unknown | 1.00 (0.97–1.04) | 0.9115 |
| Chemotherapy | ||
| Unadministered (Ref.) | 1 | |
| Multiagent | 0.38 (0.37–0.39) | < 0.0001 |
| Single agent | 0.66 (0.63–0.68) | < 0.0001 |
| Hormone therapy (yes vs. no) | 0.86 (0.84–0.89) | < 0.0001 |
| Immunotherapy (yes vs. no) | 0.81 (0.78–0.84) | < 0.0001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · CNS Lymphoma Diagnosis and Treatment · T-cell and Retrovirus Studies
Introduction
1
Diffuse Large B‐Cell Lymphoma (DLBCL) is the most common type of non‐Hodgkin lymphoma (NHL), accounting for approximately 30% of cases [1, 2]. In the United States (US), DLBCL exhibits racial variation, with White Americans having higher incidence rates compared to Black, Asian, and American Indian or Alaska Native individuals, in decreasing order of occurrence. DLBCL tends to occur more frequently in males, accounting for approximately 55% of cases [2]. Around two‐thirds of patients with DLBCL are diagnosed with advanced‐stage (III/IV) disease. Early‐stage (I/II) DLBCL has a favorable 10‐year overall survival (OS) rate of at least 80% [3, 4, 5]. Utilizing rituximab‐based chemotherapy as a curative treatment approach for all stages of DLBCL has demonstrated long‐term survival in over two‐thirds of patients and is currently the standard of care [3, 4, 5]. Despite advances in the treatment of DLBCL, determinants of survival in DLBCL stage I–IV have collectively reported Black patients and advanced stage (III–IV) to have worse outcomes on multivariate analysis [6, 7, 8, 9, 10]. Black patients with DLBCL have a risk of death that is 10% to 20% higher than the non‐Hispanic White population, noted since rituximab approval [6, 11]. Several studies suggest an association of race with socioeconomic status (SES), which was shown to affect DLBCL mortality and potential access to care [12, 13, 14, 15]. As advanced stage is a factor in outcome, available data have not focused, however, on early‐stage DLBCL to evaluate the impact of race and SES on outcome as reported. To address this research gap, the present study aims to examine and compare the characteristics and the determinants of survival between US Black and White patients diagnosed with early‐stage (I–II) DLBCL to identify opportunities for interventions for a highly curable subgroup.
Materials and Methods
2
Data Source
2.1
We aimed to determine the characteristics and outcomes for stage I and II DLBCL between Black and White patients using a retrospective analysis obtained from the National Cancer Database (NCDB) from 2004 to 2017. The NCDB is a comprehensive hospital‐based oncology database that captures around 70% of newly diagnosed cancer cases across over 1500 medical facilities in the United States, including those in Puerto Rico [16]. The NCDB is supported by the American College of Surgeons and the American Cancer Society. Since the NCDB contains de‐identified patient data, the study was exempt from Institutional Review Board approval. This study followed the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) guidelines. More detailed information on available treatments and outcomes is available in the NCDB than in the Surveillance, Epidemiology, and End Results (SEER) database. The NCDB includes the use of chemoimmunotherapy, comorbidities, primary payer, facility characteristics, and other measures of sociomedical determinants. Fewer DLBCL patients in the NCDB cohort had an unknown stage compared to those in the SEER cohort, as reported in one publication [7].
Patient Selection
2.2
Inclusion criteria comprised the following: (1) aged at least 18 years; (2) diagnosed with early‐stage (I or II) DLBCL from 2004 to 2017. Exclusion criteria included patients with unknown or unreported data regarding race or ethnicity, stage, chemotherapy, hormone therapy, and immunotherapy.
Clinical Variables
2.3
Sociodemographic data (age, race, ethnicity, gender, median household income, insurance status, education, facility type, distance to treatment facility, and facility location) and clinical characteristics (comorbidities, year of diagnosis, stage, HIV infection, presence of B symptoms, chemotherapy, hormone therapy, and immunotherapy) were included in the analysis. The standard treatment for early‐stage DLBCL is chemoimmunotherapy, conventionally cyclophosphamide, doxorubicin, vincristine, prednisone with rituximab (CHOP‐R) [16]. Approved in 1997, rituximab is a CD20 monoclonal antibody reported as an immunotherapy, while prednisone is reported as hormone therapy in the NCDB treatment categories.
Statistical Analysis
2.4
Descriptive statistics were used to summarize the patients' characteristic variables. The Chi‐square test and the Wilcoxon rank sum test were used to evaluate the differences in characteristic variables between White and Black populations. Multivariate Cox regression analysis with backward elimination was used to identify independent predictors of survival. Additionally, a Kaplan–Meier survival curve was generated for the patient cohort. Furthermore, a White and Black group‐matched sample was constructed by exact matching for all characteristic variables, and the Cox proportional hazards model with robust variance estimators was used to compare the survivorships between the White and Black patients in the matched pairs. SAS version 9.4 was used to analyze the data.
Results
3
81,430 deidentified patients diagnosed with early‐stage DLBCL between 2004 and 2017 were available for evaluation (Figure 1); 5709 (7.0%) were Black and 75,721 (93%) were White. Detailed clinical and demographic characteristics of White and Black patients are outlined in Table 1. In this dataset of early‐stage DLBCL, multivariable Cox regression analysis using the backward elimination method revealed multiple factors associated with increased mortality, including age, gender, ethnicity, income, insurance, distance traveled, Charlson‐Deyo Comorbidity Index, stage, HIV infection, B symptoms, and types of treatment received (Table 2). Higher mortality risk was observed in males (HR 1.09, 95% CI 1.06–1.11, p < 0.0001). As expected, higher risk of death was observed in patients 60 years or older (HR 2.04, 95% CI 1.96–2.12, p < 0.0001); with ≥ 2 comorbidities (HR 1.92, 95% CI 1.85–1.98, p < 0.0001); presenting with B‐symptoms (HR 1.23, 95% CI 0.53–0.68, p < 0.0001), HIV infection (HR 1.59, 95% CI 1.48–1.70) and lower household income (HR 1.18, 95% CI 1.11–1.18, p < 0.0001). Interestingly, Hispanic patients had decreased risk of death compared to non‐Hispanic patients (HR 0.84, 95% CI 0.80–0.89, p < 0.0001). Notably, survival rates between Black and White patients were not significantly different (HR 0.98, 95% CI 0.94–1.03, p = 0.5263). Kaplan–Meier analyses showed that whole cohort survival rates at 1‐, 3‐, or 5‐year were 78.8%, 68.8%, and 62.1%, respectively (Figure 2A). Kaplan–Meier survival rates for White patients at 1‐, 3‐, or 5‐year were 78.8%, 68.8%, and 61.9%, respectively (Figure 2B). Kaplan–Meier survival rates for Black patients at 1‐, 3‐, or 5‐year were 78.5%, 69.8%, and 65.6%, respectively (Figure 2C).
Consort Diagram.
A. Overall Kaplan–Meier survival curve for the whole cohort. Figure 2B. Overall Kaplan–Meier survival curve for White patients. Figure 2C. Overall Kaplan–Meier survival curve for Black patients.
Evaluation of the sociomedical variables between White and Black patients in early‐stage DLBCL revealed the following. Among the White patients, the median age was 68 years (IQR 56.0–78.0), and 56 years (IQR 43.0–68.0) for Black patients. There was an increased frequency of HIV infection, B symptoms, and a comorbidity index > 2 for Black patients compared to White patients. There were statistically significant differences in education, socioeconomic status, and type of medical coverage between the Black and White populations. Statistical differences were noted between Black and White patients in receiving chemotherapy treatment and in receiving immunotherapy, likely rituximab. Both types of treatment affect survival on multivariate analysis; immunotherapy received (HR 0.81, 95% CI 0.78–0.84) and multiagent chemotherapy received (HR 0.38, 95% CI 0.37–0.39, p < 0.0001). For the exact matching sample (n = 1,253), using all the variables in Table 1 in a 1:1 ratio, there was no significant difference in survival between White and Black groups in early‐stage DLBCL (p = 0.1818).
There was no significant difference in survival based on the year of diagnosis evaluated in 4‐year intervals. The frequency of diagnosis of early‐stage DLBCL between Black and White patients measured in 4‐year intervals was not different. Treatment has not changed significantly since the approval of rituximab in 1997. Therefore, outcomes measured from 2004 to 2017 are representative of practice patterns over the timespan. Our study reported a lower survival rate at 5 years for early‐stage lymphoma, as it includes a subset of untreated patients.
Discussion
4
In this analysis using a large nationwide cancer registry via multivariate model, we compared survival and described multiple socio‐demographic (i.e., insurance, household income, education, distance to center) and clinical factors (i.e., age, gender, Hispanic ethnicity, comorbidity, B symptoms and HIV infection) with treatment modalities associated with mortality in early‐stage (I, II) DLBCL (Table 2). Additionally, we evaluated the sociomedical determinants between Black and White patients with early‐stage DLBCL (Table 1). No significant difference in OS was found between White and Black patients in early‐stage DLBCL despite sociomedical disparities. After matching White and Black patients for homogenous characteristics, 5‐year survival remained similar. Interestingly, Hispanic patients exhibited higher survival compared to non‐Hispanic patients in our study.
Although racial disparity in survival has been observed collectively (stages I–IV) for DLBCL, we report no racial disparity in survival in early (stage I–II) DLBCL, despite finding similar disparities in sociomedical determinants as reported collectively for DLBCL. Additionally, there was no difference in survival on treatment at an academic or nonacademic center. Therefore, we suggest that the similar survival observed in early‐stage DLBCL for Black and White patients in our study is primarily overcome by the favorable remission rate of early‐stage DLBCL with chemoimmunotherapy with minimal morbidity and accessibility of a common standard therapy (CHOP‐R) that can be given at any facility. We also imply that the survival disparity between Black and White patients in DLBCL reported in published data is more likely to be the impact of socioclinical determinants on advanced stage III/IV DLBCL. We recommend that studies evaluating DLBCL outcomes across different racial groups should be stratified by stage to better determine the effect of socioclinical factors. Therefore, to narrow the survival disparity gap reported between Black and White groups, the focus should be primarily concentrated on advanced‐stage DLBCL, including access to novel treatment via clinical trials, for which distance to center and medical coverage can be barriers. We also submit that access to healthcare to detect DLBCL in the early stage, which is highly curative, may decrease the racial disparity seen across DLBCL, and therefore, awareness and education of DLBCL are warranted. Our study notes that Black patients with early‐stage DLBCL have a higher frequency of Medicaid coverage. Therefore, Medicaid expansion may have a positive impact on earlier diagnosis and treatment.
We suggest the principal factor in outcome for early‐stage DLBCL is access to standard therapy that provides excellent long‐term remission. Gene expression profiling has suggested the ABC‐subtype, associated with worse OS even after being treated with rituximab CHOP, is more commonly found in those with African American ancestry [17, 18, 19]. This would suggest that the biologic features in DLBCL in patients of African origin may not significantly influence early‐stage DLBCL. Although comorbidities and HIV infection have been borne out as variables affecting survival in early‐stage DLBCL, the differences did not appear to impact survival in early‐stage DLBCL between Black and White patients. The median age at presentation has been reported to be younger for Black Americans compared to White Americans [2, 6, 17, 18, 20, 21] for DLBCL collectively (stage I–IV). Our study of early‐stage DLBCL observed a similar age disparity.
It was interesting to note that Hispanics had a better OS in limited‐stage DLBCL, confirming previous studies that suggest better OS in Hispanics across all stages. Further studies are warranted. Blansky et al. demonstrated that Hispanics diagnosed with DLBCL had a 52% lower risk of mortality compared to non‐Hispanic whites after controlling for clinical prognostic factors [22]. It is noteworthy that Hispanics represent a broad group with different countries of origin and different genetic distributions of European, African, and Indigenous ancestry. Therefore, their unique genetic variations may contribute to their survival outcomes, and accordingly, some authors have suggested that certain genetic subtypes might have a better response to rituximab [23]. In addition, the “health immigrant effect” has been described as a condition in which those in good health are more prone to leave their country [24], and therefore, this might partly explain the results.
Strengths and Limitations
5
A key strength of our study is that we analyzed the largest cohort of patients diagnosed with early‐stage DLBCL. Therefore, our analysis captured a significant cohort of racial and ethnic groups, specifically Blacks and Hispanics living in the United States, providing real‐world insights. Important limitations of our analysis relate to the retrospective observational study design, as well as the nature of the database, due to the unavailability of some relevant data that would have allowed for capturing more patients, and it does not account for non‐observable confounding variables. Although the exact type of therapy is unknown, CHOP‐R remains the most common treatment. The number of cycles, time to treatment, and biologic features that may be significant in DLBCL cannot be further determined from the NCDB registry.
Conclusion
6
Black patients have been reported to have worse survival for DLBCL, considering both early and advanced stages collectively. However, we present the only study limited to early‐stage DLBCL that examines the survival determinants and characteristics between Black and White patients. The most remarkable finding of our study was that despite disparities in socioclinical determinants, no overall survival difference was observed between Black and White patients with early‐stage DLBCL. Our study's independent characteristics, evaluated through multivariate analysis, that were associated with a worse outcome for early‐stage DLBCL, support similar sociomedical determinants for DLBCL stages I–IV, except for race. Racial disparities and access to appropriate treatments may be more pronounced in advanced DLBCL.
Additionally, the exact matching of variables, including demographic and clinical determinants, confirmed that survival remained similar, not better. Therefore, in early‐stage DLBCL, the accessibility to standard of care with favorable remission rates and minimal morbidity, even with Medicaid being more frequent in Black patients, may be more predictive of outcome between Black and White patients and can overcome other socioclinical disparities. DLBCL should be stratified by stage to evaluate socioclinical determinants on survival. Advanced stage is a known independent prognostic feature for DLBCL. Achieving health equity in DLBCL with observed racial disparity may be more impactful on the advanced stage than for the limited stage, as there is no survival disparity between White and Black patients in stage I/II DLBCL despite the disparity in demographic and social determinants. Additionally, the conventional therapy for early DLBCL has not changed significantly and remains very favorable, for which diagnosis and treatment of DLBCL at an earlier stage (I–II) via access to healthcare may narrow the racial disparity gap observed in DLBCL.
Author Contributions
M.H., S.I., L.S., C.P.C., and C.‐L.F. conceived and designed the study. H.L. performed statistical analysis. All authors contributed to data interpretation, participated in manuscript writing, approved the manuscript for publication, and are accountable for all aspects of the work.
Ethics Statement
This study used de‐identified data from the National Cancer Database (NCDB), which is HIPAA‐compliant and does not contain patient identifiers. As such, the project was exempt from IRB review. All data use agreements were followed.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. H. Swerdlow , E. Campo , S. A. Pileri , et al., “The 2016 Revision of the World Health Organization Classification of Lymphoid Neoplasms,” Blood 127, no. 20 (2016): 2375–2390.26980727 10.1182/blood-2016-01-643569 PMC 4874220 · doi ↗ · pubmed ↗
- 2L. M. Morton , S. S. Wang , S. S. Devesa , P. Hartge , D. D. Weisenburger , and M. S. Linet , “Lymphoma Incidence Patterns by WHO Subtype in the United States, 1992–2001,” Blood 107, no. 1 (2006): 265–276.16150940 10.1182/blood-2005-06-2508 PMC 1895348 · doi ↗ · pubmed ↗
- 3S. Susanibar‐Adaniya and S. K. Barta , “2021 Update on Diffuse Large B Cell Lymphoma: A Review of Current Data and Potential Applications on Risk Stratification and Management,” American Journal of Hematology 96, no. 5 (2021): 617–629.33661537 10.1002/ajh.26151 PMC 8172085 · doi ↗ · pubmed ↗
- 4E. A. Hawkes , A. Barraclough , and L. H. Sehn , “Limited‐Stage Diffuse Large B‐Cell Lymphoma,” Blood 139, no. 6 (2022): 822–834.34932795 10.1182/blood.2021013998 · doi ↗ · pubmed ↗
- 5A. E. Rojek and S. M. Smith , “Evolution of Therapy for Limited Stage Diffuse Large B‐Cell Lymphoma,” Blood Cancer Journal 12, no. 2 (2022): 33.35210407 10.1038/s 41408-021-00596-z PMC 8867133 · doi ↗ · pubmed ↗
- 6A. A. Phillips and D. A. Smith , “Health Disparities and the Global Landscape of Lymphoma Care Today,” in American Society of Clinical Oncology Educational Book, vol. 37 (Wolters Kluwer Health, Inc, 2017), 526–534.28561692 10.1200/EDBK_175444 · doi ↗ · pubmed ↗
- 7C. R. Flowers , S. A. Fedewa , A. Y. Chen , et al., “Disparities in the Early Adoption of Chemoimmunotherapy for Diffuse Large B‐Cell Lymphoma in the United States,” Cancer Epidemiology, Biomarkers & Prevention 21, no. 9 (2012): 1520–1530.10.1158/1055-9965.EPI-12-0466 PMC 415549222771484 · doi ↗ · pubmed ↗
- 8K. Mac Dougall , S. Day , S. Hall , et al., “Impact of Race and Age and Their Interaction on Survival Outcomes in Patients With Diffuse Large B‐Cell Lymphoma,” Clinical Lymphoma, Myeloma & Leukemia 23, no. 5 (2023): 379–384.10.1016/j.clml.2023.01.01536813625 · doi ↗ · pubmed ↗