Cancer survival in Lower Silesia: insights from a national oncology network pilot in Poland
Magdalena Władysiuk, Paweł Zawadzki, Paweł Prędkiewicz, Robert Plisko, Dawid Błaszczyk, Rafał Matkowski, Adam Maciejczyk, Bożena Cybulska-Stopa

TL;DR
This study examines breast cancer survival in Polish women, showing that early detection significantly improves outcomes, especially for aggressive cancer types.
Contribution
The study provides population-based insights into breast cancer subtypes and survival in Poland's Lower Silesia region during a national oncology pilot.
Findings
Luminal B subtype is most prevalent, increasing with age to 46% in the 80+ group.
Luminal A subtype has the highest five-year survival (90.3%), while TNBC has the lowest (68.5%).
Stage I breast cancer shows ≥92% five-year survival across all subtypes, highlighting the importance of early detection.
Abstract
This study provides population-based data on biological subtypes of breast cancer (BC) and associated survival outcomes among Polish women diagnosed between 2019 and 2023 in the Lower Silesia region during the national pilot phase of the National Oncology Network (NON). Data on BC cases were obtained from the DCOPIH databases as the leader of the pilot program in Poland in between 2019 and 2023 also in the Lower Silesia region. The main outcome was overall cancer survival and cases were linked to existing mortality databases. All patient consent and scope of data analysis was provided based on the MoH Regulation. Analyses included stage at diagnosis, biological subtypes, and five-year survival, stratified by age, subtype, and stage. A total of 4490 women with BC were included. The luminal B subtype was the most prevalent, generally increasing with age and peaking at 46% in the 80+ age…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
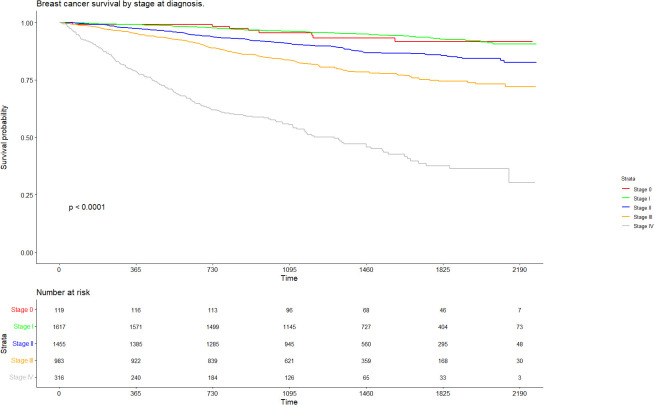 Figure 1
Figure 1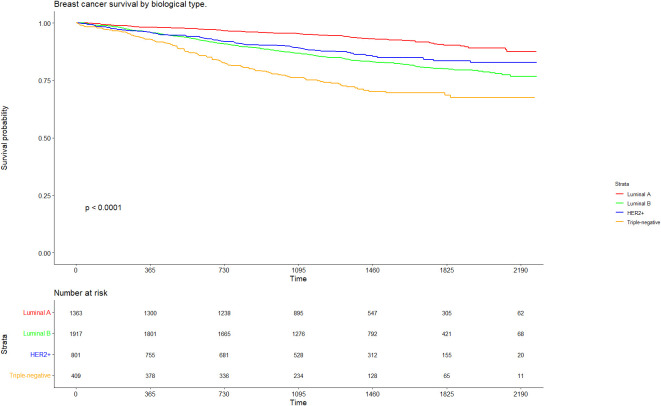 Figure 2
Figure 2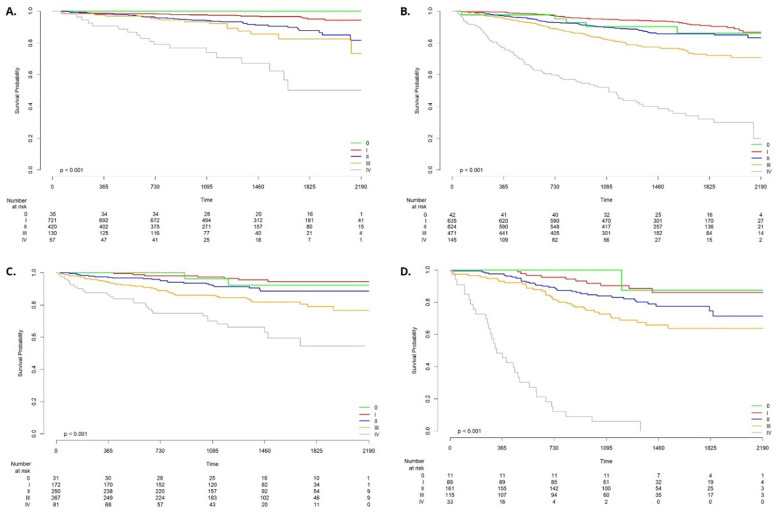 Figure 3
Figure 3| Parameter | Total (%) |
|---|---|
| N | 4490 (100%) |
| Gender | |
| Woman | 4490 (100%) |
| Age | |
| Mean (SD) | 61.6 (13, 2) |
| Median IQR | 63 (52-70) |
| Cancer stages (%) | |
| 0 | 119 (2.7%) |
| I | 1617 (36.0%) |
| II | 1455 (32.4%) |
| III | 983 (21.9%) |
| IV | 316 (7.0%) |
| Type of breast cancer | |
| Luminal A | 1363 (30.4%) |
| Luminal B | 1917 (42.7%) |
| HER2+ | 801 (17.8%) |
| Triple negative | 409 (9.1%) |
| Age | Luminal A (n=1363) | Luminal B (n=1917) | HER2-positive (n=801) | Triple-negative (n=409) | All (n=4490) |
|---|---|---|---|---|---|
| 19-39 | 1.9% | 5.9% | 10.0% | 12.2% | 6.0% |
| 40-49 | 14.3% | 14.5% | 18.5% | 13.0% | 15.0% |
| 50-59 | 18.9% | 18.9% | 21.0% | 22.2% | 19.6% |
| 60-69 | 39.3% | 33.9% | 27.6% | 30.6% | 34.1% |
| 70-79 | 17.6% | 18.2% | 15.9% | 15.4% | 17.3% |
| 80+ | 7.9% | 8.7% | 7.1% | 6.6% | 8.0% |
| Variable | Unadjusted HRs– cancer type | Unadjusted HRs– cancer stage | Adjusted HRs – cancer type and stage | Adjusted HRs - cancer type, stage and age | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | HR | 95% CI | P-value | HR | 95% CI | P-value | ||
| Cancer type | Luminal A | 1 (ref) |
|
|
|
|
| 1 (ref) |
|
| 1 (ref) |
|
|
| Luminal B | 2.45 | 1.94-3.08 | <0.001 |
|
|
| 1.85 | 1.46, 2.34 | <0.001 | 1.91 | 1.51, 2.41 | <0.001 | |
| HER2 positive | 1.98 | 1.50-2.62 | <0.001 |
|
|
| 1.20 | 0.90, 1.60 | 0.2 | 1.49 | 1.12, 1.98 | 0.007 | |
| Triple negative | 4.43 | 3.36-5.83 | <0.001 |
|
|
| 3.53 | 2.67, 4.67 | <0.001 | 4.15 | 3.13, 5.49 | <0.001 | |
| Cancer stage | I |
|
|
| 1 (ref) | 1 (ref) | 1 (ref) |
|
| 1 (ref) |
|
| |
| 0 |
|
|
| 1.13 | 0.55, 2.33 | 0.7 | 1.06 | 0.51, 2.19 | 0.9 | 1.02 | 0.49, 2.10 | >0.9 | |
| II |
|
|
| 2.24 | 1.73, 2.90 | <0.001 | 2.01 | 1.55, 2.60 | <0.001 | 1.77 | 1.36, 2.30 | <0.001 | |
| III |
|
|
| 4.13 | 3.22, 5.31 | <0.001 | 3.55 | 2.75, 4.59 | <0.001 | 3.31 | 2.55, 4.28 | <0.001 | |
| IV |
|
|
| 14.4 | 11.1, 18.7 | <0.001 | 13.9 | 10.7, 18.1 | <0.001 | 12.4 | 9.52, 16.1 | <0.001 | |
| Age group | 60-69 |
|
|
|
|
|
|
|
|
| 1 (ref) |
|
|
| <_30 |
|
|
|
|
|
|
|
|
| 1.14 | 0.47, 2.77 | 0.8 | |
| 30-39 |
|
|
|
|
|
|
|
|
| 0.56 | 0.37, 0.86 | 0.008 | |
| 40-49 |
|
|
|
|
|
|
|
|
| 0.43 | 0.30, 0.61 | <0.001 | |
| 50-59 |
|
|
|
|
|
|
|
|
| 0.60 | 0.46, 0.79 | <0.001 | |
| 70-79 |
|
|
|
|
|
|
|
|
| 1.57 | 1.27, 1.94 | <0.001 | |
| 80+ |
|
|
|
|
|
|
|
|
| 3.53 | 2.83, 4.41 | <0.001 | |
| Stage | ||||||
|---|---|---|---|---|---|---|
| 0 | I | II | III | IV | ||
| Molecular type | Luminal A | -a | 1 (ref) | 2.78 (1.66-4.67) <0.001 | 3.99(2.09-7.61) <0.001 | 12.8 (6.96-23.7) <0.001 |
| Luminal B | 1.50 (0.60-3.77) 0.4 | 1 (ref) | 1.77 (1.23-2.54) 0.002 | 3.31 (2.35-4.68) <0.001 | 12.8 (8.93-18.2) <0.001 | |
| HER2-positive | 1.50 (0.31-7.22) 0.6 | 1 (ref) | 2.28 (0.97-5.33) 0.058 | 4.49 (2.03-9.95) <0.001 | 10.7 (4.65-24.4) <0.001 | |
| Triple-negative | 0.70 (0.09-5.46) 0.7 | 1 (ref) | 1.95 (0.96-3.96) 0.064 | 3.23 (1.60-6.50) 0.001 | 32.3 (15.6-67.0) <0.001 | |
| ALL | 1.18 (0.55-2.33) 0.7 | 1 (ref) | 2.24 (1.73-2.90) <0.001 | 4.13 (3.22-5.31) <0.001 | 14.4 (11.1-18.7) <0.001 | |
| Biological type | |||||
|---|---|---|---|---|---|
| Luminal A | Luminal B | HER2-positive | Triple-negative | ||
| Stage | 0 | – | – | – | – |
| I | 1 (ref) | 2.14 (1.31-3.49) 0.002 | 1.27 (0.54-2.94) 0.6 | 3.45 (1.65-7.23) <0.001 | |
| II | 1 (ref) | 1.40 (0.94-2.07) 0.10 | 1.03 (0.61-1.75) 0.9 | 2.46 (1.53-3.94) <0.001 | |
| III | 1 (ref) | 1.86 (1.08-3.20) 0.025 | 1.45 (0.81-2.60) 0.2 | 2.86 (1.56-5.22) <0.001 | |
| IV | 1 (ref) | 2.18 (1.31-3.63) 0.003 | 1.09 (0.60-1.97) 0.8 | 7.30 (4.05-13.2) <0.001 | |
| ALL | 1 (ref) | 2.45 (1.94-3.08) <0.001 | 1.98 (1.50-2.62) <0.001 | 4.43 (3.36-5.83) <0.001 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Global Cancer Incidence and Screening · Breast Lesions and Carcinomas
Introduction
Breast cancer remains one of the most significant challenges in oncology and is the fourth most common cause of cancer-related deaths overall, ranking first among causes of cancer mortality in women (1). In Poland, it is the third most frequently diagnosed cancer, with 24, 418 new cases reported in 2022, accounting for 11.7% of all cancer diagnoses nationwide. The disease contributes substantially to cancer mortality and prevalence, with 8, 723 deaths (7.3% of all cancer-related deaths) and a five-year prevalence of 100, 017 cases, reflecting a large and growing population of women living with breast cancer or its sequalae (2).
Although breast cancer is increasingly recognized as a chronic disease, survival rates in Poland remain lower than the European average, despite significant global improvements over recent decades resulting from advances in early detection, treatment strategies, and public awareness. Since the mid-2000s, several initiatives have been undertaken in Poland to improve cancer care outcomes. These include two editions of the National Program for Cancer Disease Control. A key policy milestone occurred in January 2015, when a dedicated “fast-track” oncology pathway was introduced to expedite diagnosis and treatment for patients suspected of having cancer. In 2019, the National Oncology Network (NON) was piloted and now constitutes a central component of the National Cancer Strategy for 2020–2030 (3). A deeper understanding of the biological profiles of breast cancer within the Polish population is essential, as these features guide precision medicine approaches and provide prognostic and predictive value regarding treatment response, recurrence risk, metastatic patterns, and overall outcomes.
This article, for the first time, explores the breast cancer survival - encompassing tumor biology and patient characteristics—in women newly diagnosed between 2019 and 2023 in the Lower Silesia region, as part of the pilot implementation of the National Oncology Network.
Methods
This study is a retrospective data analysis based on a cohort derived from the pilot implementation of the National Oncology Network (NON) in the Lower Silesia region, coordinated by the Lower Silesian Oncology Center (DCOPiH), covering the period from February 1, 2019, to March 31, 2023. Data were collected by the National Health Fund in cooperation with healthcare providers based on the respective ACT (4) and the MoH Regulations. The security and protection of data was assured. A total of 6, 917 female patients newly diagnosed with primary breast cancer were included. Data collection occurred in multiple stages. In the initial phase, patients who provided informed consent (in NON pilot) and had histopathologically confirmed diagnoses were enrolled. This retrospective cohort study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Eligible participants were adult women (aged ≥18 years) with newly diagnosed primary breast cancer diagnosis (stage 0-IV) between from February 1, 2019, to March 31, 2023, regardless of treatment intent. Clinical data were extracted from medical records and coded according to the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) (5), including invasive carcinoma (code C50) and in situ lesions (code D05). All patients included in the National Cancer Network (NCN) pilot program in Poland made a written declaration of informed consent to participate in the NCN pilot program (6). Before enrollment, each patient obtained information about the principles of the pilot program and the detailed information of personal data processing as part of the NCN (6) and the long effectiveness evaluation. Tumor staging was classified into five categories (0, I, II, III, and IV), and TNM staging was determined based on the AICC/UICC and the ESMO Clinical Practice Guidelines (7). Deaths from any cause were analyzed and survival curves were generated for the entire cohort, stratified by clinical stage and biological subtype, including luminal A, luminal B, HER2-positive, and triple-negative breast cancer.
Nominal variables were summarized using frequencies and percentages, while interval-scaled variables were described using the mean, standard deviation, median, range, and interquartile range (IQR). A statistical significance level of 0.05 was adopted for the analysis. Survival analysis was conducted using the Kaplan–Meier method for the entire cohort, as well as stratified by biological subtype, clinical stage, stage within subtype, and screening status. A complete-case approach was applied, in which follow-up time was calculated from the date of diagnosis to either the date of death or the end of the study period. Differences in survival between subgroups were assessed using the Cox proportional hazards model.
Five-year (60-month) overall survival was estimated using the Kaplan–Meier product-limit method. Because the diagnostic period (2019–2023) includes patients without the possibility of complete 5-year follow-up (e.g., those diagnosed in 2022–2023), the 60-month survival probability represents a Kaplan–Meier estimate at t = 60 months, i.e., an estimate obtained under right censoring rather than observed 5-year follow-up for all individuals. Patients contributed risk time from diagnosis until death or administrative censoring; those without an event by the censoring date were treated as right-censored.
Follow-up time was defined as the time from diagnosis to removal from the risk set (death or censoring). In the analytical cohort, follow-up ranged from 7 to 2, 269 days (median 1, 313 days, IQR 935–1, 723). Among censored individuals, time to censoring ranged from 35 to 2, 269 days (median 1, 388 days, IQR 1, 044–1, 790). Thus, the minimum potential follow-up in the dataset was 7 days (overall) and 35 days among those censored.
Results
Population
A total of 6, 917 women were included in the study cohort; however, the analytical dataset comprised 4, 490 patients (Table 1).
A total of 6, 917 women who initiated the diagnostic pathway during the PSO program and for whom follow-up data were available for Kaplan–Meier analyses were initially eligible. The analytical cohort was derived using a complete-case approach for key tumour characteristics required for stratified and adjusted analyses (stage at diagnosis and biological subtype). We first excluded 418 women with missing stage information; within this group, 340 also had missing subtype data. From the remaining 6, 499 women with known stage, we additionally excluded 2, 009 women with missing subtype. The final analytical dataset therefore comprised 4, 490 women (overall exclusion: 2, 427/6, 917; 35.1%), with exclusions attributable to missing stage and/or subtype information.
To evaluate potential selection bias related to these exclusions, we compared age distributions between included and excluded individuals. Age was highly similar in the analytical cohort versus excluded cases (mean 61.6 vs 61.2 years; median 63.1 vs 62.8 years; SD 13.1 vs 13.5; range 22.4–98.8 vs 21.0–95.4), indicating negligible differences by this key baseline characteristic (standardized mean difference ≈0.03). The Wilcoxon rank sum test did not confirm the significance of median differences (p=0.30), and the Student’s t-test did not show any differences in means (p=0.25).
The mean age at breast cancer diagnosis was 61.6 years (SD = 13.1), with half of the patients being older than 63 years. The youngest patient was 22 years old, and the oldest was 99. Women aged 50–69 years—eligible for population-based breast cancer screening—constituted 53.9% of the sample.
Stage I was the most commonly diagnosed stage, accounting for 36.0% of cases, whereas stage IV disease was observed in 7.0% of patients. The most prevalent biological subtype was luminal B, identified in 42.7% of cases.
The percentage of patients diagnosed at stage 0 decreased from 3.4% in 2019 to 0.5% in 2023. The percentage of patients diagnosed at stage I in 2019–2022 varied in relatively narrow range from 34.5% in 2020 to 36.7% in 2021, while in 2023 the percentage was noticeably higher: 41.2%.
Throughout the observation period, the percentage of patients diagnosed at advanced stages (stage III or IV) ranged from 27.8% in 2019, to 29.9% in both 2020 and 2022, 28.6% in 2021, and declined to 27.3% in 2023.
In the analysed cohort, the age distribution within each biological subtype of breast cancer revealed significant differences (chi-squared test, p<0.001). Among patients with triple-negative breast cancer (TNBC), 12.2% were aged 19–39 years, indicating that younger women constituted a relatively larger share of this subgroup compared to other subtypes. Similarly, patients with HER2-positive tumours were more frequently observed in younger age categories (10.0% aged 19–39 years), whereas the proportion of young patients was markedly lower in the luminal A group (1.9%).
The luminal A subtype showed a pronounced shift toward older age groups, with 39.3% of patients aged 60–69 years and 7.9% aged ≥80 years. A similar trend, though slightly less pronounced, was observed for the luminal B subtype. The details of age and biological sub-type distribution are presented in Table 2.
Kaplan-Meier survival estimations
The overall survival rate at 36 months from the time of diagnosis was 88.8% (95% CI: 87.8%-89.7%) (Kaplan-Meier extrapolation). During the first 12 months, survival was approximately 96.3% (95% CI: 95.8%-96.9%), decreasing to 92.0% (95% CI: 91.2%-92.8%) at 24 months. At 5 years Kaplan-Meier extrapolated overall survival rate was 82.6% (95% CI: 81.2%-84.0%). A DiLO (fast-track oncology) card was issued for 98.4% of patients (n = 4, 419), while 3.2% of patients did not initiate treatment within the Lower Silesia region.
The median time from the initiation of diagnostic procedures to the commencement of treatment was 66 days across all age groups. Any type of treatment was initiated within 49 days (7 weeks) in 37.5% of patients.
In patients diagnosed at stage 0, Kaplan-Meier survival at 36/48/60 months was 95.6% (95% CI: 91.9%–99.4%), 93.3% (95% CI: 88.6%–98.3%) and 91.6%(95% CI: 86.1%–97.6%) respectively. In patients diagnosed at stage I, Kaplan-Meier survival at 36/48/60 months was therefore 96.1% (95% CI: 95.2%–97.1%), 94.9% (95%CI: 93.8%–96.1%) and 92.8% (95%CI: 91.1%–94.5%, respectively. In contrast, stage IV disease was associated with significantly lower survival – the extrapolated values were 55.4% (95% CI: 50.0%–61.4%) at 36 months, 45.7% at 48 months (95% CI: 39.8%–52.4%) and 37.6% (95% CI: 31.1%–45.4%) at 60 months (Figure 1).
Breast cancer survival by stage at diagnosis.
Patients with the luminal A subtype demonstrated the most favourable prognosis, with a 60-month Kaplan-Meier extrapolated survival rate of 90.3% (95% CI: 88.1%–92.5%). Conversely, those with triple-negative breast cancer had the poorest outcomes, with extrapolated survival declining to 68.5% (CI 95% 63.4%–74.0%) at 60 months. (Figure 2).
Breast cancer survival by biological type.
The 12-, 36- and 60 -month Kaplan-Meier survival rates among patients aged 50–69 years who participated in the screening program at DCOPiH were 99.6%, 94.8% and 89.5% respectively, representing about 3–5 percentage point increase compared to patients in the same age group who did not undergo screening within the pilot program (97.1%, 90.9% and 86.3%). Although the difference in survival rates appears clinically relevant, the Cox proportional hazards model indicated that the reduction in mortality risk did not reach conventional levels of statistical significance. The hazard ratio for the “DCOPiH Screening” group compared to the reference group (“No Screening in DCOPiH”) was 0.66 (CI 0.42-1.02 p = 0.059).
Cancer stage and type – detailed survival analysis
Analysis of the collected data confirmed that patients with the luminal A subtype exhibit the most favorable prognosis, although survival outcomes vary substantially depending on disease stage. The 60-month survival rate among patients with stage I and II disease was 95.1% and 87.8%, respectively. In contrast, survival decreased in more advanced stages, reaching 82.6% for stage III and 50.4% for stage IV. No death was recorded during the study in small subgroup of patients with stage 0 (n=35). Stage I was defined as the reference category in the Cox proportional hazards model, which demonstrated statistically significant differences in survival for stages II, III, and IV compared to stage I (p < 0.001) (Figure 3A).
Breast cancer survival by stage for biological type Luminal A (A), Luminal B (B), HER2+ (C), Triple negative (D).
Patients with the luminal B subtype showed a less favorable prognosis. The 60-month survival rates for stage I and II disease were 91.0% and 85.7%, respectively, while for stage III and IV, survival declined to 72.1% and 32.1%. In the small subset of patients diagnosed with stage 0 cancer (n=42) the 60-month survival was 86.1%. Using stage I as the reference, the Cox model indicated significantly worse outcomes for stages II–IV (p < 0.001 to p=0.002) (Figure 3B).
Among patients with the HER2-positive subtype, survival outcomes were intermediate. The 60-month survival rates were 94.4% for stage I and 88.7% for stage II. In more advanced stages, survival decreased to 79.1% for stage III and 63.0% for stage IV. The 60-month survival rate for stage 0 was 92.2%; however, this estimate is based on a small group (n = 31), with only two deaths reported during the study period. The Cox model confirmed significantly worse survival in stages III and IV compared to stage I (p < 0.001) (Figure 3C).
Among the analyzed cohort, patients with the triple-negative breast cancer subtype exhibited the poorest prognosis, with survival outcomes varying markedly by disease stage. The 60-month survival rates for stages 0, I, and II were 87.5%, 86.0%, and 74.6%, respectively. A further decline in survival was observed for patients diagnosed at stage III (63.8%), with a dramatic drop for those at stage IV, where 36-month survival reached only 6.1% and none of the patients observed survived 48 months (Figure 3D).
Adjusted Cox analysis
The Cox proportional hazards model in all patients revealed no statistically significant differences in survival between stages 0 and I in total population – neither in unadjusted and adjusted analysis, as presented in Table 3. However, stages II, III and IV were associated with a significantly increased risk of death compared to stage I, with p-values <0.001, both in the unadjusted and adjusted calculations.
In this analysis stage I was selected as the reference because there were more observations in this stage than in stage 0 for each type of cancer. In a similar vein, the 60–69 age group was selected as the reference point for age analysis, as it constituted the largest age stratum, thereby enhancing the statistical inference.
When examining the interaction between biological subtype and disease stage (Tables 4, 5), a consistent trend emerged: survival was strongly dependent on disease stage across all subtypes. The triple-negative subtype showed the widest variation in survival by stage with the hazard ratio for stage IV in TNBC compared to stage I of 32.3 (15.6-67.0). In all subtypes no significant differences were observed between stages 0 and I, and in HER2-positive and triple negative no differences were also observed between stage II and I. Stages III and IV were consistently associated with significantly worse outcomes (p < 0.001).
Discussion
This study provides comprehensive population-based insights into breast cancer survival in the Lower Silesia region during the pilot phase of the National Oncology Network (NON), with a specific focus on the prognostic relevance of clinical stage and biological subtype. The results confirm that disease stage at diagnosis remains the strongest determinant of patient outcomes, regardless of tumour biology. These findings align with international evidence and underscore the critical need for early detection, structured care coordination, and standardized reporting.
The share of categories 0+I (combined) fluctuated between 37.2% and 41.7% across the years with the share of stage I within a range of 34.5% to 41.2%. The lowest proportion was recorded in 2022 (37.2%) due to COVID19 pandemia impact, while the highest was in 2023 (41.7%). Overall, the average for the five-year period stands at 39.6%, showing a relatively stable but slightly increasing trend toward the end of the observed period. In contrast, the share of categories III+IV (combined) remained fairly stable, ranging between 27.3% and 29.9%. The highest proportions were observed in 2020 and 2022 (29.9%), whereas the lowest appeared in 2023 (27.3%). The five-year average is 28.9%, with no clear upward or downward trend overall. During the pandemic, from March 2020 to May 2022, the number of tests statistically decreased dramatically to an average of 37.93 per month for overall newly diagnosed breast cancer in DCOPIH, while positive diagnoses dropped to 24.74 per month. In comparison, from January 2018 to February 2020, the number of histopathological tests for breast cancer was relatively stable, averaging 67.23 per month, with 31.50 positive diagnoses (with positive diagnoses during this period was 46.85%) (8).
Consistent with previous studies, patients with the luminal A subtype exhibited the most favourable prognosis, with 60-month survival rates exceeding 90% in total population and 95% in stages 0 and I. This outcome reflects the relatively indolent clinical course and strong responsiveness to endocrine therapy characteristic of this subtype (9, 10). Luminal B tumours, although also hormone receptor–positive, were associated with a moderately worse prognosis—especially at advanced stages—likely due to higher proliferation indices and reduced endocrine sensitivity (11). Among HER2-positive patients, survival was high in early stages but declined at stage IV (54.6%), probably due the availability of targeted therapies such as trastuzumab and pertuzumab (12, 13). Triple-negative breast cancer (TNBC) was associated with the poorest prognosis, showing a precipitous drop in 60-month survival from 86.0-87.5% at stages 0 and I to only 63.8% at stage III. In stage IV TNBC cancer no patient was observed to achieve a 48-month survival and the study documented a 36-month survival rate of only 6.1% (14, 15). The fact that this particular type of cancer has such a low survival rate is especially notable given that this specific subtype comprised the highest proportion of patients in the youngest age group, i.e. those under 30 years of age.
The pattens of age structure within each biological subtype in our study reflect the known association between tumour biology and patient age, with hormone receptor–positive subtypes being more common in older women, and aggressive subtypes such as TNBC and HER2-positive tumours being relatively more prevalent among younger patients within their respective subtype distributions. Age at diagnosis may then inform risk stratification, surveillance intensity, and treatment planning.
Importantly, while biological subtype stratifies risk within stages, survival declined consistently across all subtypes with increasing disease stage. Patients with stage 0 and I disease had 60-month survival rates exceeding 86%, while those diagnosed at stage IV had survival rates as low as 0–54.6%, depending on subtype. Notably TNBC cases showed the most pronounced stage-dependent decline. These findings reflect the biological aggressiveness and limited treatment options for TNBC and reinforce the need for intensified systemic therapy and rapid intervention in this group.
Despite significant improvements in breast cancer treatment, Poland continues to lag behind many EU countries in survival outcomes. In 2021, breast cancer mortality in Poland was 20 per 100, 000 women - 5% higher than the EU average. While the mortality rate declined by 8% in Poland between 2011 and 2021, the EU average saw a 16% reduction during the same period. Moreover, while two-thirds of EU countries had reached five-year survival rates of ~80% for breast cancer patients diagnosed between 2000 and 2007, Poland only achieved a similar benchmark for patients diagnosed between 2015 and 2018 (16). For this period, five-year survival in Poland was 77%, compared to the EU average of 82%. Regional disparities further complicate the landscape: five-year survival in the 2010–2014 period ranged from 69.7% (Podkarpackie) to 79.8% (Mazowieckie), with Lower Silesia at 77.3%—broadly consistent with our observed outcomes.
The pilot implementation of the National Oncology Network in Lower Silesia aimed to address these systemic deficiencies. It introduced standardized diagnostic and treatment pathways, mandatory participation of multi-level care providers (SOLO I–III), and centralized coordination by Provincial Coordinating Centers. Additionally, it was the first nationwide program to implement real-time digital data collection and reporting for oncology quality indicators. The Lower Silesia Oncology Center was also the first in Poland to obtain iPAAC certification in breast cancer care, contributing to consistent and standardized data collection.
Nevertheless, the results reveal persistent gaps in early detection. Only 2.7% of patients in this population were diagnosed at stage 0, but European guidelines recommending that at least 15% of new breast cancer cases should be diagnosed at this stage in this population (17). In the pilot population for the Lower Silesia 7.3% had in situ breast cancer. Furthermore, only 36.0% of cases were detected at stage I, while stages III and IV accounted for 21.9% and 7.0%, respectively. These distributions stand in contrast to results from Norway (2005–2010), where 90.6% of cancers were diagnosed at stages I–II, and just 9.4% at stages III–IV, as well as similar benchmarks in the Netherlands and Spain (18).
These observations are particularly concerning given that participation in screening programs in Poland remains low - only 37% of eligible women underwent screening in 2023. In our analysis, patients aged 50–69 who participated in screening at DCOPiH had 36 and 60-month survival rates of 94.8% and 89.5 respectively, compared to 90.9% and 86.3% among non-participants. Although the difference did not reach conventional statistical significance (HR = 0.66 CI 0.42-1.02 p = 0.059), it reflects a clinically relevant benefit and aligns with previous European data showing that population-based screening programs reduce the incidence of advanced breast cancer and improve survival (19–24).
Indeed, systematic reviews and cohort studies from the Netherlands, Sweden, Finland, Italy, Germany, and France have consistently demonstrated that organized screening programs lead to a measurable reduction in the incidence of advanced-stage disease (T2+, N+, stage II+) (25). For example, Paci et al. (26) reported a risk ratio of 0.72 for stage II+ cancers in screened versus unscreened populations, while Dutch studies (27) showed annual reductions in advanced breast cancer incidence ratios ranging from 0.86 to 0.72 (19, 21). Our findings are consistent with these trends and reinforce the need for broader access and adherence to screening programs in Poland. Finally, while our results generally correspond to international registry data (e.g., Canadian Cancer Registry), notable differences remain in the distribution of disease stages and biological subtypes. For example, Canadian data showed about 47% of luminal A tumours, whereas this figure was 30.3% in our cohort (28). These discrepancies may reflect differences in population structure, access to care, and data completeness.
Conclusions
Survival outcomes in breast cancer in Poland are strongly influenced by both the biological subtype and the stage at diagnosis. Early-stage detection through screening and rapid diagnostic pathways remain the most effective strategies to improve prognosis, particularly for aggressive subtypes such as TNBC and HER2-positive disease. The implementation of the National Oncology Network represents a step toward coordinated, data-driven cancer care in Poland, but further efforts are needed to increase screening participation, reduce diagnostic delays, and standardize treatment across regions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 2Didkowska J Barańska K Miklewska MJ Wojciechowska U . Cancer incidence and mortality in Poland in 2023. Nowotwory J Oncol. (2024) 74:75–93. doi: 10.5603/njo.99065, PMID: 39099251 · doi ↗ · pubmed ↗
- 3Sagan A Kowalska-Bobko I Gałązka-Sobotka M Holecki T Maciejczyk A Mc Kee M . Assessing recent efforts to improve organization of cancer care in Poland: what does the evidence tell us. Int J Environ Res Public Health. (2022) 19:9369. doi: 10.3390/ijerph 19159369, PMID: 35954721 PMC 9368127 · doi ↗ · pubmed ↗
- 4Act of 27th August 27, 2004 on healthcare benefits financed from public funds Dz.U.2025.1461. Available online at: https://dziennikustaw.gov.pl/DU/2025/1461 (Accessed January 11, 2025).
- 5Organization WH . International Classification of Diseases for Oncology (ICD-O): First Revision. 3rd ed. Geneva: World Health Organization (2013). p. 252.
- 6Regulation of the minister of health of 13 December 2018 on the pilot program of care for the patients within the oncological network, Dz.U. 2018 poz.2423 (2018). Available online at: https://isap.sejm.gov.pl/isap.nsf/Doc Details.xsp?id=WDU 20180002423 (Accessed January 11, 2025).
- 7Cardoso F Kyriakides S Ohno S Penault-Llorca F Poortmans P Rubio IT . Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. (2019) 30:1194–220. doi: 10.1093/annonc/mdz 173, PMID: 31161190 · doi ↗ · pubmed ↗
- 8Szkudlarek D Kalinowska K Wiatrak B . Impact of the COVID-19 pandemic on histopathological cancer diagnostics in Lower Silesia: A comparative analysis of prostate, breast, and colorectal cancer from 2018 to 2022. Cancers (Basel). (2025) 17:134. doi: 10.3390/cancers 17010134, PMID: 39796761 PMC 11720222 · doi ↗ · pubmed ↗