Crossed Erythrocytes Agglutination Pattern Observed in a Patient With Hereditary Elliptocytosis
Márcio A. W. Melo, Cristina M. Silveira, Maíra M. Ribeiro, Gabriela S. Arcanjo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
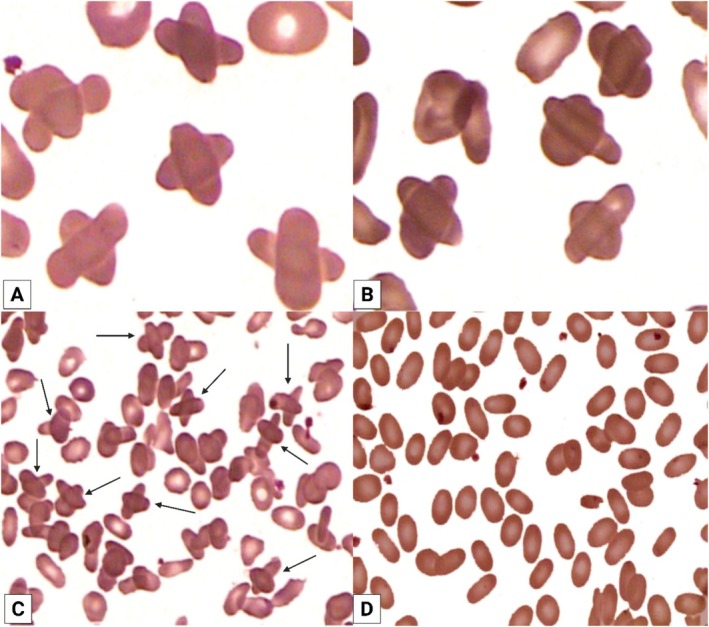 FIGURE 1
FIGURE 1- —Coordenação de Aperfeiçoamento de Pessoal de Nível Superior ‐Brasil (CAPES)10.13039/501100002322
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsErythrocyte Function and Pathophysiology · Blood properties and coagulation · Blood groups and transfusion
Case Image
1
Hereditary elliptocytoses (HE) are a group of autosomal dominant disorders characterized by peripheral blood smears showing at least 70% of erythrocytes with an elliptical shape. This abnormal morphology occurs because mutations in the spectrin protein of the cytoplasmic membrane cause erythrocytes to lose elasticity. Defects in spectrin dimer–dimer associations and in the spectrin–actin–protein 4.1 complex of the red cell membrane junction lead to weaker horizontal connections in the cytoskeleton. HE affects populations worldwide, with an estimated incidence of approximately 1 in every 2.000 to 4.000 individuals. It is more prevalent in malaria‐endemic areas, as elliptocytes may offer some resistance to the protozoan, providing a selective advantage to those affected with HE. For example, in West Africa, the prevalence of HE is approximately 1 in every 100 individuals [1].
Here, we report unusual findings in an 88‐year‐old woman with the symptomatic form of HE and no family history of erythrocyte membrane disorders. The patient did not report any medication use, nor were there signs of hepatic, renal, or endocrine dysfunction. Her blood tests showed a normal leukocyte count (7.9 × 10^9^/L; reference: 4–11 × 10^9^/L) and a platelet count (166 × 10^9^/L; reference: 150–450 × 10^9^/L). However, her hematimetric indices revealed anemia, with a low erythrocyte count (2.4 × 10^12^/L; reference: 4.0–5.4 × 10^12^/L), hemoglobin level (7.4 g/dL; reference: 12.0–16.0 g/dL), and hematocrit (21.9%; reference: 36%–46%). The red blood cell indices were as follows: mean corpuscular volume (MCV) 91.2 fL (reference: 80–101 fL), mean corpuscular hemoglobin (MCH) 30.8 pg (reference: 27–33 pg), mean corpuscular hemoglobin concentration (MCHC) 33.7 g/dL (reference: 31.5–36 g/dL), and red cell distribution width (RDW) 16.3% (reference: 11.5%–15.5%), indicating anisocytosis. Her peripheral blood smear showed over 75% elliptocytes and the peculiar presence of erythrocytes that agglutinated and were arranged perpendicularly to each other, forming a cross or an “X” shape (Figure 1A–C).
Peripheral blood smear stained with May‐Grünwald‐Giemsa. (A, B) Magnification 2000×, showing multiple “crossed” erythrocytes. (C) Magnification 800×, also demonstrating the presence of several “crossed” erythrocytes. (D) After washing the whole blood five times with 0.9% saline, the peripheral blood smear (800×) shows the absence of “crossed” erythrocytes, indicating that the phenomenon was reversed by restoring normal electrical charge between erythrocytes.
To rule out other hematological disorders that could explain this unusual erythrocyte arrangement, additional tests were performed. A myelogram presented normal results (apart from the presence of elliptocytes), and immunophenotyping of peripheral blood also showed no abnormalities. Together, these findings confirmed the diagnosis of HE.
To date, erythrocyte agglutination has only been described in the form of rouleaux—where red cells stack on top of one another—or in cases triggered by cold or warm antibodies, which result in irregular aggregates of erythrocytes [2]. However, “crossed” erythrocytes have not been described in either of these conditions.
To investigate the cause of these crossed erythrocytes, a sample of whole blood was washed five times with 0.9% saline solution. New blood smears were then prepared. The cytological assay showed that the crossed erythrocytes disappeared (Figure 1D), suggesting that their formation was due to alterations in surface electric charges between erythrocytes, which were reversed by the saline washes [3]. Three months later, a follow‐up blood smear confirmed the recurrence of “crossed” erythrocytes, and again, saline washing abolished their formation.
Interestingly, the presence of “crossed” erythrocytes has also been occasionally observed by our group in the peripheral blood of other HE patients.
Author Contributions
M.A.W.M., C.M.S., and M.M.R. wrote the manuscript and contributed to the diagnosis of the case. G.S.A. critically revised the article. All authors read and approved the final version of the manuscript.
Funding
The article processing charge for the publication of this research was funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior ‐Brasil (CAPES).
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. G. Patrick , “Abnormalities of the Erythrocyte Membrane,” Pediatric Clinics of North America 60, no. 6 (2013): 1349–1362.24237975 10.1016/j.pcl.2013.09.001PMC 4155395 · doi ↗ · pubmed ↗
- 2I. Talstad , P. Scheie , H. Dalen , and J. Roli , “Influence of Plasma Proteins on Erythrocyte Morphology and Sedimentation,” Scandinavian Journal of Haematology 31, no. 5 (1983): 47884.10.1111/j.1600-0609.1983.tb 01547.x 6648360 · doi ↗ · pubmed ↗
- 3E. Bennett‐Guerrero , B. S. Kirby , H. Zhu , A. E. Herman , N. Bandarenkon , and T. J. Mc Mahon , “Randomized Study of Washing 40 to 42 Day Stored Red Blood Cells,” Transfusion 54, no. 10 (2014): 2544–2552.24735194 10.1111/trf.12660 PMC 4194130 · doi ↗ · pubmed ↗