COVID-19 Infection in a Patient With Sigmoid Diverticulitis: Viral Diverticulitis or Incidental Association?
Maria J Araujo, Victor A Sato, Precil D Neves, Erico S Oliveira, Leonardo V Pereira, Sara Mohrbacher, Alessandra M Bales, Luciana L Nardotto, Marcella M Frediani, Andrea Santos Galvão, Wares F Medeiros, Américo L Cuvello-Neto, Pedro R Chocair

TL;DR
A woman with diverticulitis developed a persistent fever, later found to be caused by a coinciding COVID-19 infection.
Contribution
This case emphasizes the need to consider viral infections like COVID-19 when treating patients with diverticulitis and unexplained fever.
Findings
A patient with acute sigmoid diverticulitis developed persistent fever and was later diagnosed with SARS-CoV-2.
The patient's symptoms improved after completing antibiotic therapy and with the resolution of the viral infection.
The case suggests the importance of testing for viral infections in patients with treatment-resistant fever.
Abstract
This report describes the case of a previously healthy 54-year-old woman who presented with acute sigmoid diverticulitis. Outpatient treatment with ciprofloxacin and metronidazole was initiated. After four days of starting on antibiotics, she returned to the hospital with medication-resistant fever and worsening abdominal discomfort, prompting admission. Intravenous therapy with appropriate antibiotics (ceftriaxone and metronidazole) was initiated, but the fever recurred, suggesting possible treatment failure. On the fourth day of hospitalization, with the onset of mild respiratory symptoms (mild rhinorrhea and nasal voice), a respiratory viral panel was performed, which tested positive for SARS-CoV-2. The patient showed progressive clinical improvement and was discharged after completion of antibiotic therapy. This case highlights the importance of considering viral infections,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
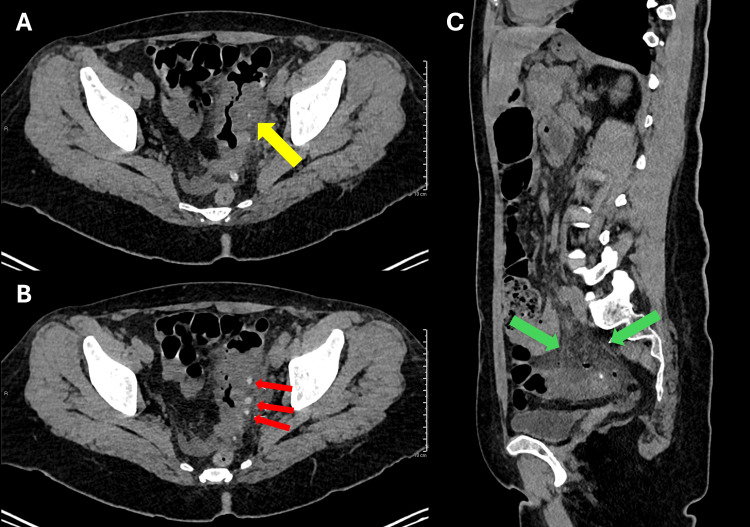 Figure 1
Figure 1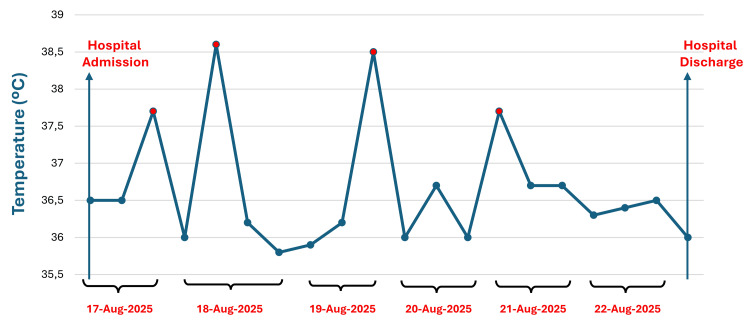 Figure 2
Figure 2| Laboratory Test | Reference Range | Day 0 | Day 4 | Day 7 | Day 9 |
| Hemoglobin (g/dL) | 11.7 – 14.9 | 14.6 | 13.9 | 12.2 | 13.2 |
| Hematocrit (%) | 35.1 – 45.1 | 41.3 | 39.7 | 35.5 | 38 |
| Leukocytes (/mm3) | 3,650 – 8,120 | 10,730 | 10,820 | 5,730 | 5,560 |
| Platelets (/mm3) | 163,000 – 343,000 | 193,000 | 199,000 | 186,000 | 193,000 |
| Creatinine (mg/dL) | 0.6 – 1.1 | 0.71 | 0.72 | - | 0.63 |
| C-Reactive protein (mg/dL) | <1 | 1.8 | 1.61 | 1.20 | 0.55 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiverticular Disease and Complications · Pneumothorax, Barotrauma, Emphysema · Otolaryngology and Infectious Diseases
Introduction
Acute colonic diverticulitis is a common gastrointestinal condition, accounting for a significant proportion of emergency department visits related to abdominal pain and fever, particularly in middle-aged and older adults [1,2]. The disease results from micro- or macro-perforation of a colonic diverticulum, leading to localized inflammation and, in some cases, abscess formation or peritonitis. Uncomplicated diverticulitis is usually managed conservatively with antibiotics and supportive care, while complicated cases may require invasive interventions [1].
Persistent fever during treatment typically raises concern for complications such as abscess, perforation, or antimicrobial failure. However, during the COVID-19 pandemic, SARS-CoV-2 infection has been increasingly recognized as a cause of gastrointestinal symptoms, including abdominal pain, diarrhea, and fever, sometimes occurring in the absence of prominent respiratory manifestations [3-6].
Several reports have demonstrated that COVID-19 may mimic acute abdominal conditions or alter their clinical presentation, posing diagnostic challenges for clinicians [7-12]. In this context, distinguishing persistent inflammatory fever from treatment failure versus concomitant viral infection becomes clinically relevant. We report a case of acute sigmoid diverticulitis in which persistent fever during appropriate antimicrobial therapy was ultimately explained by concurrent SARS-CoV-2 infection, highlighting an important diagnostic pitfall.
Case presentation
A 54-year-old woman, previously healthy and a living kidney donor approximately 20 years earlier, presented to the emergency department with a three-day history of unconfirmed fever and left lower quadrant abdominal pain. She denied respiratory symptoms at presentation. Physical examination revealed a patient in good general condition, afebrile, with blood pressure of 118/68 mmHg, respiratory rate of 18 breaths per minute, heart rate of 75 beats per minute, and an axillary temperature of 36.5°C. Abdominal examination showed tenderness on deep palpation of the left iliac fossa, with mild rebound tenderness.
Laboratory tests showed hemoglobin of 14.6 g/dL, hematocrit of 41.3%, leukocyte count of 10,730/mm³, platelet count of 193,000/mm³, serum creatinine of 0.71 mg/dL, no electrolyte abnormalities, amylase of 56 U/L, lipase of 31 U/L, C-reactive protein of 1.8 mg/dL, aspartate aminotransferase (AST) of 16 U/L, alanine aminotransferase (ALT) of 13 U/L, and a normal urinalysis. Laboratory test results are given in Table 1. Abdominal computed tomography (CT) without intravenous contrast revealed findings consistent with uncomplicated sigmoid diverticulitis, including focal parietal thickening of a sigmoid diverticulum and adjacent mesenteric fat stranding (Figure 1) [1,2].
Non-contrast abdominal CT findings consistent with acute sigmoid diverticulitis.(A, B) Axial images showing parietal thickening of a sigmoid diverticulum (yellow and red arrows) and adjacent wall. (C) Sagittal image demonstrating densification of the adjacent mesenteric fat (green arrows).
The patient was initially managed on an outpatient basis with oral ciprofloxacin (500 mg twice daily) and metronidazole (400 mg three times daily). After four days of antibiotic therapy, she returned to the emergency department due to persistent fever, chills, and worsening abdominal discomfort, prompting hospital admission for further evaluation.
On physical examination, blood pressure was 140/70 mmHg, respiratory rate 16 breaths per minute, heart rate 88 beats per minute, and temperature 38.5 °C (Figure 2). Abdominal examination again demonstrated tenderness on deep palpation of the left iliac fossa, without important rebound tenderness. Laboratory evaluation revealed hemoglobin of 13.9 g/dL, hematocrit of 39.7%, leukocyte count of 10,820/mm³, platelet count of 199,000/mm³, serum creatinine of 0.72 mg/dL, no electrolyte disturbances, amylase of 56 U/L, lipase of 31 U/L, C-reactive protein of 1.2 mg/dL, AST of 16 U/L, and ALT of 13 U/L (Table 1). Antibiotic therapy was escalated to intravenous ceftriaxone (1 g twice daily), while metronidazole was continued.
Temperature curve during the hospitalization
Over the following days, despite improvement in abdominal pain, the patient continued to experience daily episodes of fever. On the fourth day of hospitalization, a contrast-enhanced abdominal CT scan was performed to exclude potential complications of diverticulitis, which showed no evidence of abscess formation, perforation, or disease progression. In addition to fever, the patient reported new mild upper respiratory symptoms, including rhinorrhea and nasal speech.
Given these findings, a respiratory viral panel using reverse-transcription polymerase chain reaction (RT-PCR) was performed, and tested positive for SARS-CoV-2. The patient remained hemodynamically stable, required no respiratory support, and had no recurrence of abdominal pain. She completed a seven-day course of antibiotic therapy, did not receive any specific antiviral treatment, and became afebrile on the same day the COVID-19 diagnosis was established. She was discharged two days later in good clinical condition. At follow-up, she reported complete resolution of abdominal symptoms and no COVID-19-related complications.
Discussion
This case aims to highlight the diagnostic challenges associated with persistent fever in diverticulitis. Although antibiotic treatment failure or intra-abdominal complications are the main initial concerns, concurrent viral infections should also be considered. SARS-CoV-2 has been shown to cause gastrointestinal symptoms, which may manifest with fever and abdominal pain in the absence of significant respiratory symptoms [3-6]. Abdominal imaging may be normal in some patients with COVID-19; however, a systematic review indicates that more than half of cases exhibit abdominal findings [7].
Persistent fever in diverticulitis during the COVID-19 pandemic should also prompt consideration of non-abdominal causes, including viral infections [8-12]. In patients with diverticulitis undergoing antibiotic treatment, persistent fever or the emergence of new febrile episodes during the clinical course should prompt evaluation with contrast-enhanced abdominal computed tomography to investigate disease-related complications, such as abscess formation or perforation. Other potential sources of fever, including pulmonary or urinary complications that may develop during the course of the illness, should also be considered [13,14].
Besides the clinical overlap, several biological mechanisms support this association: SARS-CoV-2 demonstrates enterotropism, thus disrupting the gut microbiota and inducing microvascular injury, which may contribute to diverticular inflammation. These mechanisms provide a plausible explanation for persistent fever despite appropriate antimicrobial therapy, highlighting the need to consider viral etiologies when the clinical course deviates from expected [8-12]. A previous report has indicated that the clinical appearance of diverticulitis can be altered by a concomitant viral infection and that gastrointestinal symptoms and extra-abdominal complications are common in patients with COVID-19 [12].
Gastrointestinal symptoms, including abdominal pain, nausea, vomiting, and diarrhea, have been reported in approximately 20% of patients diagnosed with COVID-19 [3,4,12]. There are reports of COVID-19 mimicking appendicitis, cholecystitis, and colitis; however, its overlap with diverticulitis is rarely described [9-12]. This rarity highlights the importance of this case report. Previous studies also highlight that persistent fever in diverticulitis should not be immediately interpreted as treatment failure, but rather that extra-abdominal causes, such as viral infections and variations in clinical presentation related to the pandemic, should be considered immediately [8-12].
In patients with diverticulitis under antibiotic treatment, persistent or recurrent fever should prompt contrast-enhanced abdominal CT scanning to rule out complications such as abscess or perforation. Other potential clinical sources of fever, including pulmonary or urinary infections, should also be considered [13,14].
Conclusions
Persistent fever in patients with diverticulitis is not necessarily a sign of treatment failure or disease progression. In the current epidemiological context, particularly when mild respiratory symptoms are present, COVID-19 infection should be considered as a potential confounder, while maintaining standard evaluation for diverticulitis-related complications. Physicians need to be aware of this diagnostic challenge, as identifying viral coinfection can avoid unnecessary antibiotic use or invasive interventions, ultimately contributing to patient safety and outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12020 update of the WSES guidelines for the management of acute colonic diverticulitis in the emergency setting World J Emerg Surg Sartelli M Weber DG Kluger Y 321520203238112110.1186/s 13017-020-00313-4PMC 7206757 · doi ↗ · pubmed ↗
- 2Epidemiology, pathophysiology, and treatment of diverticulitis Gastroenterology Strate LL Morris AM 1282129815620193066073210.1053/j.gastro.2018.12.033PMC 6716971 · doi ↗ · pubmed ↗
- 3Prevalence of gastrointestinal symptoms and fecal viral shedding in patients with coronavirus disease 2019: a systematic review and meta-analysis JAMA Netw Open Parasa S Desai M Thoguluva Chandrasekar V 03202010.1001/jamanetworkopen.2020.11335 PMC 729040932525549 · doi ↗ · pubmed ↗
- 4Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, cross-sectional, multicenter study Am J Gastroenterol Pan L Mu M Yang P 76677311520203228714010.14309/ajg.0000000000000620 PMC 7172492 · doi ↗ · pubmed ↗
- 5Abdominal imaging findings in COVID- 19: preliminary observations Radiology Bhayana R Som A Li MD 015297202010.1148/radiol.2020201908 PMC 750800032391742 · doi ↗ · pubmed ↗
- 6Gastrointestinal symptoms and COVID- 19: case-control study from the United States Gastroenterology Nobel YR Phipps M Zucker J Lebwohl B Wang TC Sobieszczyk ME Freedberg DE 37337515920203229447710.1053/j.gastro.2020.04.017PMC 7152871 · doi ↗ · pubmed ↗
- 7A systematic review of abdominal imaging findings in COVID-19 patients Visc Med Singh P Singh SP Verma AK Raju SN Parihar A 1122620213458063410.1159/000518473 PMC 8450847 · doi ↗ · pubmed ↗
- 8Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID- 19): a review JAMA Wiersinga WJ Rhodes A Cheng AC Peacock SJ Prescott HC 78279332420203264889910.1001/jama.2020.12839 · doi ↗ · pubmed ↗