A Comparative Analysis of Microscopic and Endoscopic Stapedotomy: A Prospective Study
Ishi Jain, Pradeep Singh Rawat

TL;DR
This study compares microscopic and endoscopic stapedotomy techniques for otosclerosis, finding that endoscopic surgery offers better visualization and fewer complications.
Contribution
The study introduces a direct comparison of endoscopic and microscopic stapedotomy, highlighting the advantages of endoscopic techniques in surgical precision and patient outcomes.
Findings
Endoscopic stapedotomy provides better visualization of anatomical landmarks compared to microscopic stapedotomy.
Endoscopic surgery requires less drilling and manipulation of the facial nerve, leading to reduced postoperative pain and dizziness.
Both techniques are effective in improving hearing outcomes, but endoscopic stapedotomy has better cosmetic results.
Abstract
Stapedotomy is a procedure performed for the treatment of otosclerosis in which a small hole is created in the footplate stapes and a prosthesis is inserted from the incus to the vestibule. The present study aims to compare the benefits of endoscopic stapedotomy with those of microscopic stapedotomy. We included 20 patients of the Outpatient Department of Ear, Nose, and Throat (ENT) of a private medical college, who were diagnosed with otosclerosis and were scheduled to undergo stapedotomy. After they provided informed consent, the patients were randomly divided into two groups: group A underwent microscopic stapedotomy, and group B, endoscopic stapedotomy. Both the groups were compared in terms of intraoperative time, surgical approach, visualization of anatomical landmarks, extent of drilling of the posterosuperior part of external auditory canal, manipulation of the facial nerve,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
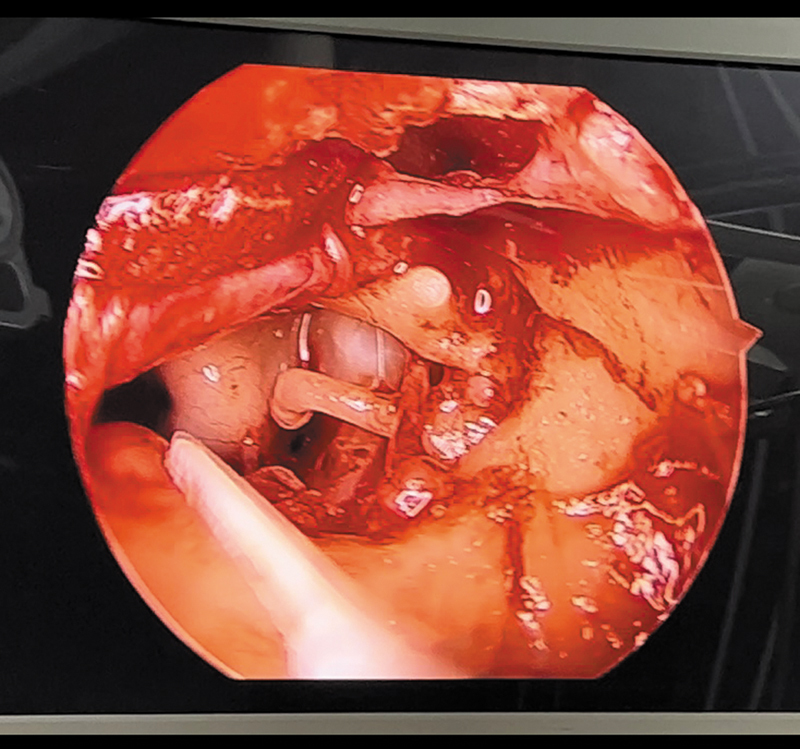 Fig. 1
Fig. 1| Parameters | Group A (microscopic stapedotomy) | Group B (endoscopic stapedotomy) | ||
|---|---|---|---|---|
| Mean age (years) | 39.5 | 38.9 | 1 | |
| Gender (n) | Male | 4 | 3 | 0.63 |
| Female | 6 | 7 | ||
| Parameters | Group A (microscopic stapedotomy) | Group B (endoscopic stapedotomy) | ||
|---|---|---|---|---|
| Mean intraoperative time (minutes) | 54.5 | 50.9 | 1 | |
| Surgical approach (n) | Transcanal | 6 | 10 | 0.025 |
| Postaural | 4 | 0 | ||
| Anatomical landmarks visualized (n) | Anterior crura of the stapes | 2 | 10 | 0.001 |
| Long process of the incus | 7 | 10 | 0.06 | |
| Chorda tympani manipulated (n) | 10 | 2 | 0.001 | |
| Need for drilling (n) | 10 | 2 | 0.001 | |
| Parameters | Group A (microscopic stapedotomy) | Group B (endoscopic stapedotomy) | ||
|---|---|---|---|---|
| Mean postoperative pain score on the Visual Analog Scale | 5.8 | 5.1 | 1 | |
| Postoperative dizziness (n) | 10 | 4 | 0.025 | |
| Postoperative hearing loss (air-bone gap) at the 4th week (n) | < 20 dB | 5 | 6 | 0.23 |
| > 20 dB | 5 | 4 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Vestibular and auditory disorders · Nasal Surgery and Airway Studies
Introduction
Stapedotomy is a procedure performed for the treatment of otosclerosis in which a small hole is created in the footplate stapes and a prosthesis is inserted from the incus to the vestibule.
Objective
The present study aims to compare the benefits of endoscopic stapedotomy with those of microscopic stapedotomy.
Methods
The current study was conducted at the Outpatient Department of Ear, Nose, and Throat (ENT) of a private medical college between February 2023 and February 2024. After the application of the inclusion and exclusion criteria, we selected 20 cases of otosclerosis to compose the sample. After receiving approval from the institutional Ethics in Research Committee and obtaining proper informed written consent from each patient, the sample was randomly divided into two groups: group A underwent microscopic stapedotomy, and group B, endoscopic stapedotomy. Stapedotomy was performed in all the patients either via the transcanal approach or the postaural approach. A tympanomeatal flap was raised, and the middle ear structures were visualized. Then, the posterior wall of the external auditory canal was drilled, and stapes fixation was checked. After that, the stapedial tendon was dissected, the incudostapedial joint was cut, and the anterior and posterior crura of the stapes were fractured and removed. A small hole, or fenestration, was created in the footplate of the stapes using a microdrill. Then, a teflon prosthesis was inserted into the fenestration to bypass the fixed stapes, the tympanomeatal flap was repositioned, and the external auditory canal was filled with abgel. 5
The inclusion criteria were a diagnosis of otosclerosis based on clinical history, an otoscopic examination within normal limits, pure tone audiometry conclusive of conductive hearing loss, with an air-bone gap ≥ 20 dB, 1 absent stapedial reflex on impedance audiometry, and normal appearance of the temporal bone on high-resolution computed tomography scans. And the exclusion criteria were history or presence of middle and external ear infection and pure tone audiometry conclusive of conductive hearing loss, with an air-bone gap < 20 dB.
Points of Comparison
Intraoperative timing (from infiltration of the local anesthetic agent in the external auditory canal until the placement of last piece of abgel).Surgical approach – in patients with wider external auditory canals, the transcanal approach was used; and in cases of a narrow canal, the postaural approach was preferred.Visualization of anatomical landmarks such as the long process of the incus and the anterior crura of the stapes.Extent of drilling of the posterosuperior part of the external auditory canal.Manipulation of the chorda tympani.Postoperative pain assessed through the Visual Analog Scale (VAS) 8 hours after surgery.Postoperative dizziness assessed 8 hours after surgery.Postoperative hearing assessment at the 4th week after surgery through pure tone audiometry, with a comparison with the preoperative hearing loss.
Both groups were compared using the Chi-squared test.
Results
Table 1 shows the demographic characteristics of the sample. The mean age of the subjects in group A was 39.5 years, and, in group B, 38.5 years, which was not statistically significant ( p = 1).
In both groups, there was a predominance of female subjects (6 in group A and 7 in group B), which was not statistically significant either ( p = 0.63).
Table 2 shows the comparison of intraoperative parameters. In group A, the mean intraoperative time was 54.5 minutes, while in group B it was 50.9 minutes, which was not statistically significant ( p = 1).
Regarding the approach, 6 patients in group A were submitted to the transcanal approach and 4, to the postaural approach. In group B, all patients were operated on via the transcanal approach. This was statistically significant ( p = 0.025).
The anterior crura of the stapes was visualized in all patients in group B, but only in 2 patients in group A, which was statistically significant ( p = 0.001).
The long process of the incus was visualized in 7 patients in group A, and in all subjects in group B, which was not statistically significant ( p = 0.06).
Manipulation of the chorda tympani was performed in all subjects in group A, but only in 2 patients in group B, which was statistically significant ( p = 0.001).
Drilling of the posterosuperior part of the external auditory canal was performed in all subjects in group A, and only in 2 subjects in group B, which was also statistically significant ( p = 0.001).
Table 3 shows the comparison of postoperative parameters. The mean postoperative pain score on the VAS was 5.8 in group A and 5.1 in group B, which was not statistically significant ( p = 1)
Postoperative dizziness assessed after 8 hours of surgery was present in all subjects in group A and only in 4 patients in group B, which was statistically significant ( p = 0.025)
The postoperative air-bone gap in the 4th week after surgery was lower than 20 dB in 5 patients in group A and in 6 patients in group B, and it was higher than 20 dB in 5 patients in group A and in 4 patients in group B, which was not statistically significant ( p = 0.23).
Discussion
Stapedotomy, a surgical procedure to treat otosclerosis in which the traditional approach is microscopic, has undergone advancements with the introduction of endoscopic techniques.
In the current study, there was a predominance of female patients, which is in line with a study by Harikumar and Kumar, 3 in which there were 38 female and 22 male subjects.
In the present study, the mean intraoperative time for microscopic stapedotomy was 54.5 minutes, which was longer than the intraoperative time for endoscopic stapedotomy (50.9 minutes), a finding similar to that of the study by Migirov and Wolf. 6
In the current study as well as in the study by Kojima et al., 7 the transcanal approach was used only in microscopic stapedotomy. We also observed that visualization of the middle ear structures was better in the endoscopic procedure, which is in line with the findings by Nikolaos et al., 8 who stated that endoscopic stapedotomy provides more detailed visualization of the middle ear structures.
In the present study, there were higher levels of manipulation of the chorda tympani in microscopic stapedotomy, an observation similar to the one made by Mahendran et al., 9 in which manipulation of the chorda tympani was only performed in microscopic procedures.
We also observed that the need for drilling of the posterorsuperior part of the external auditory canal was minimal in endoscopic stapedotomy in the current study, which is in line with the study by Migirov and Wolf. 6
Regarding the levels of postoperative pain, they were higher in the microscopic group in the current study and in the study by Iannella et al. 10 As for the levels of postoperative dizziness, they were lower in the endoscopic group in the present study, and minimal in the same group in the study by Ataide et al. 11
According to present study, there was no significant difference in the postoperative air-bone gap between the the groups, a finding similar to the one made by Harikumar and Kumar. 3
Techniques such as canal straightening stitch or 3-mm otoendoscopy can also be used, but these techniques are surgeon- and institution-specific.
Conclusion
In conclusion, the findings of the present study shed light on the efficacy and safety of microscopic stapedotomy versus endoscopic stapedotomy in the treatment of otosclerosis. Through a meticulous examination and comparison of outcomes, it becomes evident that both techniques offer distinct advantages, but considerations must be made. Microscopic stapedotomy, with its established history and familiarity among surgeons, showcases consistent success rates. On the other hand, endoscopic stapedotomy emerges as a promising alternative, resulting in enhanced visualization of middle-ear structures, minimal need of drilling, lower levels of postoperative pain and dizziness, as well as a lower requirement of manipulation of the chorda tympani ( Fig. 1 ).
Middle-ear structures viewed from a 0° endoscope.
However, it is crucial to acknowledge the nuanced complexities and learning curves associated with each approach. Surgeon experience, patient-specific factors, and institutional resources all play pivotal roles in determining the optimal choice of technique. Furthermore, ongoing advancements in endoscopic instrumentation and surgical techniques may further shape the landscape of stapes surgery in the future.
Ultimately, the decision between microscopic and endoscopic stapedotomy should be made judiciously, considering the unique circumstances of each patient and the proficiency of the surgical team.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gleeson M Growing G G Burton M J Clarke R John H Jones N S Scott- Brown's Otorhinolaryngology: Head and Neck Surgery 7th ed London Hodder Education 2008
- 2Ho S Patel P Ballard D Rosenfeld R Chandrasekhar S Systematic review and meta-analysis of endoscopic vs microscopic stapes surgery for stapes fixation Otolaryngol Head Neck Surg 20211650562663510.1177/019459982199066933528314 · doi ↗ · pubmed ↗
- 3Harikumar B Kumar KJ A Comparative study between microscopic and endoscopic stapes surgery Int J Otorhinolaryngol Head Neck Surg 201730228528910.18203/issn.2454-5929.ijohns 20171179 · doi ↗
- 4Fan C J Kaul V F Mavrommatis M A Schwam Z G Hu S Kong D K Endoscopic versus microscopic stapedotomy: a single-blinded randomized control trial Otol Neurotol 202142101460146610.1097/MAO 000000000000329834726874 · doi ↗ · pubmed ↗
- 5Isaacson B Hunter J B Rivas A Endoscopic stapes surgery Otolaryngol Clin North Am 2018510241542810.1016/j.otc.2017.11.01129395112 · doi ↗ · pubmed ↗
- 6Migirov L Wolf M Endoscopic transcanal stapedotomy: how I do it Eur Arch Otorhinolaryngol 2013270041547154910.1007/s 00405-013-2420-523463349 · doi ↗ · pubmed ↗
- 7Kojima H Komori M Chikazawa S Yaguchi Y Yamamoto K Chujo K Moriyama H Comparison between endoscopic and microscopic stapes surgery Laryngoscope 20141240126627110.1002/lary.2414423670854 · doi ↗ · pubmed ↗
- 8Nikolaos T Aikaterini T Dimitrios D Sarantis B John G Eleana T Konstantinos M Does endoscopic stapedotomy increase hearing restoration rates comparing to microscopic? A systematic review and meta-analysis Eur Arch Otorhinolaryngol 2018275122905291310.1007/s 00405-018-5166-230327907 · doi ↗ · pubmed ↗