Disseminated Cutaneous Herpes Zoster in an Immunocompetent Patient: A Diagnostic Challenge
Meriah Frauwirth, Randall Scott

TL;DR
A rare case of disseminated cutaneous herpes zoster in a healthy adult highlights the diagnostic challenges and importance of early treatment.
Contribution
This case report adds to the understanding of DCHZ in immunocompetent individuals and emphasizes early diagnosis.
Findings
DCHZ can occur in immunocompetent adults and may mimic benign skin conditions.
Early recognition is crucial to prevent complications.
Clinical differentiation based on lesion morphology and symptoms is essential.
Abstract
Disseminated cutaneous herpes zoster (DCHZ) typically occurs in immunocompromised individuals. However, rare cases arise in immunocompetent adults. These cases may initially resemble benign dermatoses or be difficult to distinguish from other systemic rashes when overlapping risk factors obscure diagnosis. Early recognition is essential to prevent visceral or neurologic complications. A 32-year-old immunocompetent male with childhood varicella presented with a 10-day history of a pruritic vesicular rash, right ear fullness, and viral prodromal symptoms. He had recent diving exposure five days prior. The eruption began with axillary myalgia progressing to vesicles spanning multiple right thoracic dermatomes, eventually extending anteriorly. Folliculitis was excluded due to non-pustular morphology and preceding neuropathic discomfort. Decompression-related skin injury was ruled out,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
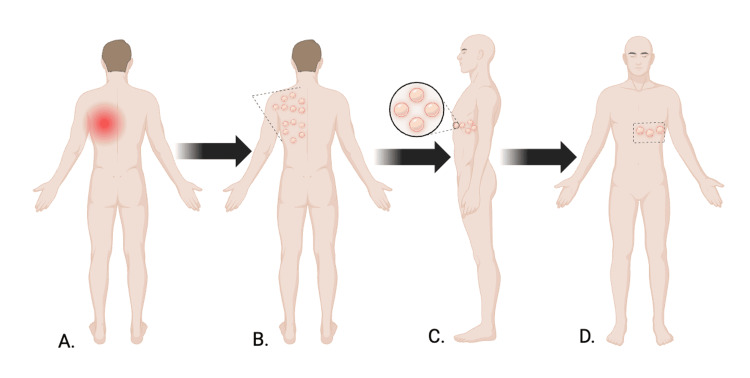 Figure 1
Figure 1 Figure 2
Figure 2| Disease | Folliculitis | “The Bends” (Decompression Sickness) | Disseminated Cutaneous Herpes Zoster (DCHZ) |
| Cause | Superficial inflammation or infection of hair follicles, commonly caused by Staphylococcus aureus | Nitrogen gas embolization due to rapid decompression after diving | Reactivation of latent varicella-zoster virus- widespread vesicular eruption involving ≥20 lesions beyond the primary or adjacent dermatomes |
| Risk Factors | Friction, occlusion, moisture, or bacterial contamination after shaving or water exposure | Deep or prolonged dives, inadequate decompression, repetitive diving | Typically immunocompromised states, though, may occur in transient immune dysregulation or viral prodrome in immunocompetent adults |
| Presentation | Small, erythematous pustules centered around hair follicles, often pruritic or tender | Mottled or marbled reddish-purple rash (cutis marmorata) with joint pain, dizziness, or neurologic symptoms | Grouped vesicular lesions on an erythematous base following multiple dermatomes, usually confined to one body side |
| Prognosis | Generally self-limited | Life-threatening | Potentially serious |
| Management | Warm compress, avoid irritants, topical antibiotics | Hyperbaric oxygen therapy needed | Early antiviral therapy prevents visceral or neurologic complications |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Facial Nerve Paralysis Treatment and Research · Cytomegalovirus and herpesvirus research
Introduction
Herpes zoster (HZ) is one of the most well-known dermatologic manifestations that is classically described with a dermatomal rash. Herpes zoster is understood to be caused by the reactivation of latent varicella-zoster virus (VZV) within sensory ganglia. This leads to a pathognomonic unilateral vesicular rash confined to a single dermatome, without crossing the body’s midline. Disseminated cutaneous herpes zoster (DCHZ) is defined as having ≥20 vesicular lesions outside the primary or adjacent dermatomes and traditionally occurs in immunocompromised hosts [1,2]. However, rare cases in immunocompetent adults exist and establish that viral dissemination can occur even without immune dysfunction [2-4].
Disseminated herpes zoster can lead to life-threatening complications with potential visceral organ involvement and neurologic complications; therefore, early recognition and antiviral treatment are critical [5,6]. Clinical management and diagnosis may be challenging due to unusual clinical presentation, symptom onset, or relevant risk factors for other systemic rashes. This case highlights a rare case of disseminated herpes zoster in an immunocompetent adult and emphasizes the diagnostic challenges and importance of timely antiviral therapy.
Case presentation
A 32-year-old male, with a childhood history of varicella infection at age four, presented with a 10-day history of a pruritic, erythematous vesicular rash and right ear fullness. The patient was a frequent diver with an involved underwater activity and had last descended five days prior to his office visit. He reported right axillary muscle pain that was unlike the typical soreness he experiences after diving sessions. He also admitted to headaches and sinus congestion, suggesting a possible viral upper respiratory prodrome. He denied dizziness, confusion, nausea, or vomiting.
The eruption began with localized axillary myalgia, followed by the appearance of itchy, mildly painful vesicles over the right posterior thoracic region. Over several days, the lesions crusted and partially healed, while new vesicles appeared and progressively spread across multiple right thoracic dermatomes. The rash subsequently extended anteriorly, following the dermatomal distribution to the chest below the nipple line (Figure 1). The eruption consisted of more than 20 vesicular lesions extending beyond the primary and adjacent dermatomes, meeting criteria for disseminated cutaneous herpes zoster. He denied fever, burning, tingling, or other systemic symptoms. Symptomatic measures such as epsom salt baths and ibuprofen provided minimal relief.
Progression and distribution of vesicular eruptionsSchematic illustration demonstrating the temporal progression and anatomic distribution of the patient’s cutaneous findings. Panel A depicts localized neuropathic discomfort preceding rash onset. Panel B shows clustered vesicular lesions involving multiple right posterior thoracic dermatomes. Panel C provides a magnified view of grouped vesicles. Panel D illustrates subsequent anterior extension below the nipple line. Arrows indicate areas of interest, including posterior involvement, anterior progression, and satellite lesions beyond contiguous regions, consistent with disseminated cutaneous herpes zoster. Created in BioRender. Frauwirth, M. (2026) https://BioRender.com/joz7k3o
A comprehensive clinical evaluation was initiated to determine the underlying etiology. Folliculitis was excluded as the lesions were vesicular rather than pustular, were not centered around hair follicles, and the presence of localized neuropathic pain preceding the rash was inconsistent with a bacterial process (Figure 2). The more serious diagnosis of decompression-related skin injury (“the bends”) was also ruled out, as the rash lacked the mottled or marbled pattern typically associated with nitrogen embolization. Further, the lack of neurologic deficits and the timeline for serious illness, even considering delayed diagnosis, was well past 24-48 hours of typical occurrence (Table 1).
Disseminated clusters of vesicles involving multiple thoracic dermatomesClinical photograph demonstrating clustered vesicular lesions distributed across multiple right thoracic dermatomes, consistent with disseminated cutaneous herpes zoster. The image demonstrates grouped vesicles accompanied by satellite lesions extending beyond adjacent dermatomal boundaries.
Physical examination revealed clustered vesicular lesions involving multiple thoracic dermatomes with several satellite vesicles beyond contiguous regions, consistent with disseminated cutaneous herpes zoster (Figure 2). Furthermore, the distribution confined to the right thoracic dermatomes, accompanied by localized muscle discomfort and progression along contiguous dermatomes, was most consistent with herpes zoster infection. Taken together, the clinical presentation strongly suggested a diagnosis of disseminated herpes zoster infection. The patient’s prior varicella infection, along with the characteristics of the skin lesions and associated symptoms, reinforced the diagnosis of disseminated cutaneous herpes zoster. The patient was started on valacyclovir 1 gram orally three times daily for 14 days and gabapentin 300 mg daily for neuropathic discomfort, with subsequent improvement in pain and gradual resolution of the vesicular lesions.
Discussion
Disseminated herpes zoster in immunocompetent adults is rare but potentially life-threatening if not promptly recognized and treated, and is generally defined as the presence of 20 or more vesicular lesions occurring outside the primary or adjacent dermatomes [2,3]. Systemic dissemination can lead to serious neurologic complications, including but not limited to the notorious Ramsay Hunt syndrome, Bell’s palsy, or encephalitis, as well as systemic complications such as hepatitis or pneumonitis in otherwise healthy individuals [5,6]. The early presentation of skin manifestations may complicate the diagnosis. This is because early presentation may mimic benign dermatoses such as folliculitis or contact dermatitis. In cases with prevalent risk factors, such as this patient, decompression-related skin changes may be considered as differential. The simultaneous involvement of multiple dermatomes is not the most common presentation and may lead to overlooking herpes zoster infection and delaying diagnosis. Delayed diagnosis increases the potential for ongoing viral replication, thereby increasing the risk of systemic involvement. Therefore, when evaluating unilateral or disseminated dermatomal eruptions with vesicles extending beyond a single dermatome or associated neuropathic pain, it is important to consider herpes zoster infection. Early initiation of high-dose antiviral therapy is the mainstay of management, limiting viral replication and preventing potential visceral complications [1,5].
Reports suggest that aging is the primary risk factor for disseminated varicella-zoster virus infection in immunocompetent hosts [3,9]. However, in our case, disseminated VZV occurred in a younger male. An alternative explanation for disseminated cutaneous herpes zoster in younger immunocompetent individuals may be related to transient changes in immunity, specifically viral infections or physiological stress. These factors may cause brief suppression of VZV-specific T-cell immunity, allowing viral reactivation and dissemination in otherwise healthy hosts, such as our patient [3,10]. This patient’s upper respiratory viral prodrome may have contributed to the reactivation, or the stress-related diving may have acted as a catalyst for this event. However, it would be challenging to specify whether one event had more influence than the other. While DCHZV in immunocompetent adults is rare, a greater understanding of the mechanisms and risk factors that may contribute to the disease process is critical. This case illustrates how disseminated herpes zoster in an immunocompetent adult can be clinically difficult to distinguish from more common cutaneous conditions, reinforcing the importance of thoughtful diagnostic evaluation, early recognition, and prompt antiviral intervention, while also raising consideration of preventive strategies such as vaccination.
Conclusions
This case demonstrates the diagnostic challenge posed by disseminated herpes zoster in an immunocompetent adult, especially when the eruption resembles benign skin disorders or when coexisting factors predispose the patient to alternative rash etiologies. Identification requires thoughtful evaluation of lesion morphology, distribution, and symptom progression. Clinicians should consider DCHZ when vesicles extend beyond a single dermatome, particularly in the setting of viral prodrome or life stress. Clinicians should recognize that dissemination can occur even in healthy adults, and timely antiviral therapy is essential to prevent systemic spread and associated complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Centers for Disease Control and Prevention: Clinical overview of shingles (herpes zoster) 5 2024 2024 https://www.cdc.gov/shingles/hcp/clinical-overview/index.html
- 2Disseminated cutaneous herpes zoster in an immunocompetent elderly patient Infect Dis Rep Gomez E Chernev I 5513620142527633210.4081/idr.2014.5513 PMC 4178270 · doi ↗ · pubmed ↗
- 3Disseminated herpes zoster in an immunocompetent elderly patient Korean J Pain Yoon KJ Kim SH Lee EH Choi JH 1951982620132361408610.3344/kjp.2013.26.2.195PMC 3629351 · doi ↗ · pubmed ↗
- 4A case of disseminated zoster in an immunocompetent patient Cureus Drone E Ganti L 011201910.7759/cureus.6286 PMC 693997131911878 · doi ↗ · pubmed ↗
- 5Herpes zoster N Engl J Med Cohen JI 25526336920132386305210.1056/NEJ Mcp 1302674 PMC 4789101 · doi ↗ · pubmed ↗
- 6Herpes zoster N Engl J Med Gnann JW Jr Whitley RJ 34034634720021215147210.1056/NEJ Mcp 013211 · doi ↗ · pubmed ↗
- 7Folliculitis Winters RD Mitchell M Treasure Island (FL)Stat Pearls 2025 https://www.ncbi.nlm.nih.gov/books/NBK 547754/31613534 · pubmed ↗
- 8Decompression Sickness Cooper JS Hanson KC Treasure Island Stat Pearls 2025 https://www.ncbi.nlm.nih.gov/books/NBK 537264/30725949 · pubmed ↗