Post-hospital physical rehabilitation for physical function recovery among community-dwelling survivors of critical illness: A systematic review protocol
Christopher Farley, Anastasia N.L. Newman, Christine Caron, Kimia Honarmand, Stuart M. Phillips, Jenna Smith-Turchyn, Dina Brooks, Jiawen Deng, Jiawen Deng

TL;DR
This study will review how post-hospital physical rehabilitation affects long-term recovery in adults who survived critical illness.
Contribution
The protocol introduces a systematic review to evaluate the effectiveness of post-hospital physical rehabilitation for critical illness survivors.
Findings
The review will assess physical function recovery 12 months after acute care discharge.
It will include randomized controlled trials comparing rehabilitation to non-physical interventions.
The study will use Cochrane methods and GRADE to evaluate evidence certainty.
Abstract
Many survivors of critical illness experience lasting physical disability. Post-hospital rehabilitation has the potential to reduce this physical disability; however, primary studies have reported inconsistent results. We aimed to answer the following question: Among community-dwelling adults who survived critical illness, does participation in post-hospital physical rehabilitation, compared with no rehabilitation or alternative non-physical interventions, improve physical functioning 12 months after discharge from acute care? This is a systematic review protocol that was registered with PROSPERO (CRD 420251174065). It will be conducted with Cochrane methods and reported according to the 2020 Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. To optimize the impact of this review, our study team includes a patient partner to guide our methods and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
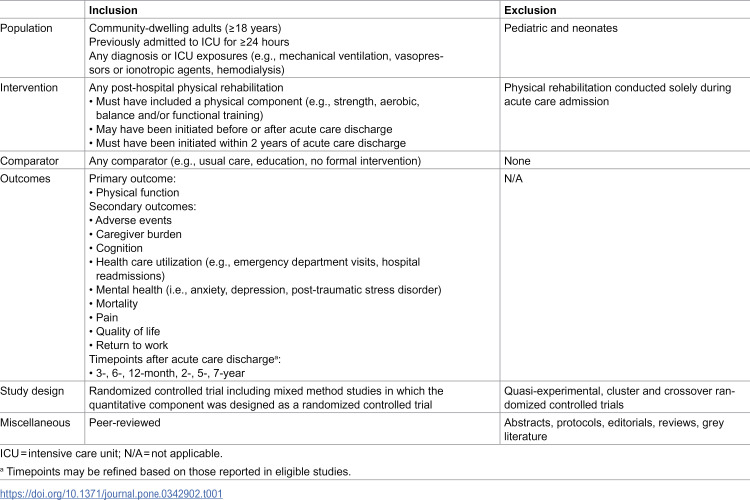 Figure 1
Figure 1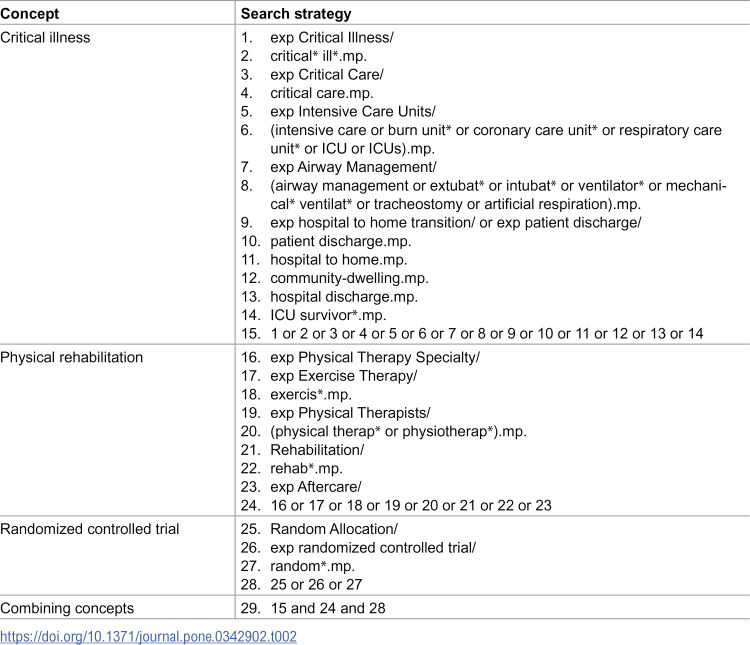 Figure 2
Figure 2- —http://dx.doi.org/10.13039/501100000221Canadian Lung Association
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Frailty in Older Adults · Cerebral Palsy and Movement Disorders
Introduction
The intensive care unit (ICU) provides care for people who have or are at risk of life-threatening illness, particularly of the respiratory, cardiac and renal systems [1]. With advances in intensive care medicine knowledge and technology, survival rates from critical illness are improving. Despite higher illness severity among patients, a retrospective time series analysis found a 35% decrease in ICU mortality from 1988 to 2012 in United States’ hospitals [2]. With improved survival, intensive care approaches no longer focus solely on survival but now integrate approaches to reduce the negative sequelae associated with critical illness [3].
Post-intensive care syndrome is a new onset or worsening of impairments in physical, cognitive and/or mental health that arises from an ICU admission and persists beyond hospital discharge [4,5]. These impairments are closely linked to the profound muscle loss experienced by adults with critical illness, who lose 2.1% (95% confidence interval [CI] 1.0 to 3.2) rectus femoris and 2.2% (95% CI 1.8 to 2.6) biceps brachii cross-sectional area each day [6]. Furthermore, for each day of immobilization within the ICU, survivors experienced a 3% (95% CI 0–7) reduction in muscle strength at hospital discharge [7]; this loss was compounded such that patients experienced an 11% (95% CI 4–19) strength reduction at 2-year follow-up for each day of ICU bedrest [7]. Overall, these physical impairments contribute to the 40% of people with critical illness who develop ICU-acquired weakness [8].
Seminal research followed survivors of critical illness after hospital discharge and found that 1 year after hospital discharge, they experienced physical disability with 6-minute walk test (6MWT) scores that were 66% of age- and sex-matched norms [9]. Even 5 years after hospital discharge, these survivors continued to have physical disability with 6MWT scores that were 76% of age- and sex-matched norms [10]. Further research has found lasting impacts on participation among survivors of critical illness. A cohort of 5,762 survivors of critical illness found that 2 years after hospital discharge, 30% were unable to return to work [11]. Post-hospital rehabilitation has the potential to reduce the physical disability and resultant participation limitations associated with critical illness.
Recent syntheses have indicated the potential benefit of post-hospital rehabilitation [12,13]; compared to controls, Cazeta et al. [12] reported significant improvement in SF-36 Physical Function scores among four trials (N = 341, mean difference = 4.04 [1.19 to 6.90]). However, these recent reviews only included patients who had required invasive mechanical ventilation [12,13], which only represents about one-third of those admitted to the ICU [14]. To capture the overall effect of post-hospital rehabilitation on those after critical illness, broad population eligibility criteria are necessary. As such, we set out to answer the following question: Among community-dwelling adults who survived critical illness, does participation in post-hospital physical rehabilitation, compared with no rehabilitation or alternative non-physical interventions, improve physical functioning 12 months after discharge from acute care?
Materials and methods
We registered our systematic review with the International Prospective Register of Systematic Reviews (PROSPERO) on 29 October 2025 (CRD420251174065). We have reported our protocol according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) Protocols (PRISMA-P) 2015 statement (S1 Table in S1 File) [15]. Our systematic review will be conducted using methods consistent with the Cochrane Handbook for Systematic Reviews of Interventions [16] and reported according to 2020 PRISMA statement [17].
Eligibility criteria
Peer-reviewed studies will be eligible for inclusion if they enrolled community-dwelling adults (≥ 18 years) who were previously admitted to the ICU for ≥24 hours and participated in a post-hospital physical rehabilitation program compared to any control intervention (Table 1). Our primary outcome is physical function, as measured by a validated outcome measure. Physical function refers to an individual’s ability to complete physical movements or actions necessary to maintain independence in living [18]. Only randomized controlled trials will be eligible, including mixed methods studies in which the quantitative component was designed as a randomized controlled trial.
Table 1: Eligibility criteria.
Information sources
We will search Medline (OVID interface, 1946 onwards), Embase (OVID interface, 1974 onwards), Emcare (OVID interface, 1995 onwards), Cumulative Index to Nursing and Allied Health Literature (EBSCOhost interface, 1981 onwards), and Web of Science (Clarivate interface, 1976 onwards) from their respective inceptions. We will hand search reference lists of included studies to identify potentially eligible reports which were missed by our database search.
Search strategy
We will develop search strategies for each database in consultation with a health sciences librarian. Search strategies will be composed of controlled vocabulary (i.e., subject headings) and keywords of three concepts: (i) critical illness, (ii) physical rehabilitation, and (iii) randomized controlled trial. We will combined search terms using Boolean operators. Each database search strategy will be validated by determining if it located three relevant citations previously identified by the authors [19–21]. Our preliminary Medline search strategy is available in Table 2.
Table 2: Preliminary Medline search strategy.
Screening and extraction
Search results will be uploaded to Covidence systematic review software (2025, Veritas Health Innovation Ltd., Melbourne, Australia) where citations will be automatically deduplicated. Two reviewers, working independently and in duplicate, will complete title and abstract screening and full-text review. During study title and abstract screening, reviewers will assess each title and abstract as potentially eligible or not eligible. If at least one reviewer deems a citation potentially eligible, it will be advanced to study selection. During study selection, reviewers will assess each full report for eligibility. Where disagreements exist, they will be resolved through discussion or with a third reviewer to arbitrate. To optimize reviewer consistency, a calibration activity of five to ten publications will be conducted prior to commencement of both study screening and selection. Within the resultant manuscript, study selection will be summarized using a PRISMA flow diagram.
We will complete data extraction independently and in duplicate using a standardized extraction template in Covidence. We will resolve discrepancies through discussion or a third reviewer, as needed. For each included study, we will extract data from its main manuscript and any supplemental material or cited protocols. Where discrepancies exist between documents, we will prioritize information from the main manuscript. Where results are incompletely reported and clarification is required, we will attempt to contact relevant study authors by email up to three times. Extracted information will include:
aStudy characteristics (e.g., title, journal, year of publication, first author, contact information, study design, funding sources)bParticipant characteristics (e.g., eligibility criteria, sample size, age, sex, ICU admission diagnosis, duration of ICU admission, comorbidities)cIntervention characteristics (e.g., setting, intervention description including frequency, intensity, timing, and type, treatment fidelity)dComparator characteristics (e.g., setting, comparator description including frequency, intensity, timing, and type, treatment fidelity)eOutcomes (e.g., construct assessed, outcome measure, assessment timepoint)fSample size, measures of central tendency and dispersion for sought outcomes.
If a study utilizes multiple outcome measures to assess a particular construct, we will prioritize extraction according to their primary outcome measure, followed by the outcome measure with the largest proportion of reported participant data.
Risk of bias
We will conduct risk of bias assessments for each extracted outcome using version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2) [22]. Accordingly, each outcome will be assessed for bias arising from: (i) the randomization process, (ii) deviations from intended interventions, (iii) missing outcome data, (iv) measurement of the outcome and (v) selection of the reported results [22]. Risk of bias will be assessed as ‘low risk’, ‘some concerns,’ and ‘high risk.’ Assessments will be conducted independently and in duplicate with disagreements resolved through discussion or with a third reviewer, as necessary. Within the resultant manuscript, risk of bias assessments will be presented in tables and figures.
Data analysis and synthesis
Data synthesis.
Results will be presented in text and table form. If results are sufficiently homogeneous, we will conduct meta-analyses using random-effects modeling with Review Manager (RevMan) software. If results are not homogeneous, we will summarize narratively.
Measures of treatment effect.
We will report dichotomous variables as risk ratio and 95% CIs. Where authors use the same continuous outcome measure, we will report as mean difference with 95% CIs. Conversely, if similar continuous outcome measures are utilized, we will report as standardized mean difference and 95% CIs.
Management of missing data.
If data are insufficiently reported to allow for inclusion in a meta-analysis, we will attempt to contact study authors up to three times for clarification. If further clarification is not obtained, we will exclude these results from the meta-analysis and report them narratively.
Assessment of heterogeneity.
We will assess clinical and statistical heterogeneity. When assessing clinical heterogeneity, we will consider population characteristics, intervention and comparator group components and outcome measures utilized. Statistical heterogeneity will be assessed by visual inspection of forest plots, with the Chi-squared test (p < 0.1) and the I^2^ statistic (0–40% = not important heterogeneity; 30%−60% = moderate heterogeneity; 50–90% = substantial heterogeneity; 75%−100% = considerable heterogeneity) [16].
Subgroup analyses.
We plan to conduct subgroup analyses according to the following criteria:
aBy physical rehabilitation type (i.e., strength-based versus aerobic-based versus multi-component)bBy time of physical rehabilitation initiation (i.e., early initiation [within 1 month of acute care discharge] versus delayed initiation [3 months or later after acute care discharge])cBy primary ICU admission diagnosis (i.e., sepsis versus cardiac versus respiratory versus neurological)dBy treatment fidelity (i.e., high [≥80% of planned dose] versus low [<80% of planned dose])
Sensitivity analyses.
We have no plans to conduct sensitivity analyses.
Quality of evidence
We will assess the strength of the body of evidence for each outcome using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) [23]. Accordingly, results for each outcome will be assessed against five domains: risk of bias, inconsistency, indirectness, imprecision and publication bias [23]. Certainty of evidence will be graded as high, moderate, low or very low and will be presented in a summary of findings table.
Dissemination of results
We plan to submit our findings for presentation at a critical care related conference and for publication within a peer-reviewed journal. We will also publish our extracted data on Open Science Framework at the time of publication.
Patient or public involvement
Our aim is to conduct a systematic review that maximizes impact on people who have survived critical illness. As such, the study team includes a patient partner (CC) to guide our approach and conduct. To date, our patient partner has assisted with refining our research questions, eligibility criteria and outcomes of interest [24]. Future roles will include guiding extraction components, interpreting results and identifying future directions from our findings.
Significance
Approximately 40% of people with critical illness develop ICU-acquired weakness [8]. An international multiprofessional expert panel recently proposed a research agenda related to management of ICU-acquired weakness which included a need to understand how follow-up care models can optimize long-term recovery after critical illness [25]. A recent synthesis indicated the potential post-hospital rehabilitation has to improve physical function in survivors of critical illness [12], however, eligibility was limited to those who required invasive mechanical ventilation, which represents about one-third of ICU patients [14]. Our review will provide a comprehensive synthesis of how post-hospital rehabilitation can influence long-term recovery of survivors of critical illness by including studies which enrolled all patients who were admitted to the ICU for at least 24 hours. Our approach should provide a broad understanding of the impact of post-hospital rehabilitation on survivors of critical illness.
Supporting information
S1 FilePRISMA-P Checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marshall JC, Bosco L, Adhikari NK, Connolly B, Diaz JV, Dorman T, et al. What is an intensive care unit? A report of the task force of the World Federation of Societies of Intensive and Critical Care Medicine. J Crit Care. 2017;37:270–6. doi: 10.1016/j.jcrc.2016.07.015 27612678 · doi ↗ · pubmed ↗
- 2Zimmerman JE, Kramer AA, Knaus WA. Changes in hospital mortality for United States intensive care unit admissions from 1988 to 2012. Crit Care. 2013;17(2):R 81. doi: 10.1186/cc 12695 23622086 PMC 4057290 · doi ↗ · pubmed ↗
- 3Kho ME, Connolly B. From Strict Bedrest to Early Mobilization: A History of Physiotherapy in the Intensive Care Unit. Crit Care Clin. 2023;39(3):479–502. doi: 10.1016/j.ccc.2023.01.003 37230552 · doi ↗ · pubmed ↗
- 4Hiser SL, Fatima A, Ali M, Needham DM. Post-intensive care syndrome (PICS): recent updates. J Intensive Care. 2023;11(1):23. doi: 10.1186/s 40560-023-00670-7 37221567 PMC 10202754 · doi ↗ · pubmed ↗
- 5Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40(2):502–9. doi: 10.1097/CCM.0b 013e 318232 da 75 21946660 · doi ↗ · pubmed ↗
- 6Fazzini B, Märkl T, Costas C, Blobner M, Schaller SJ, Prowle J, et al. The rate and assessment of muscle wasting during critical illness: a systematic review and meta-analysis. Crit Care. 2023;27(1):2. doi: 10.1186/s 13054-022-04253-0 36597123 PMC 9808763 · doi ↗ · pubmed ↗
- 7Fan E, Dowdy DW, Colantuoni E, Mendez-Tellez PA, Sevransky JE, Shanholtz C, et al. Physical complications in acute lung injury survivors: a two-year longitudinal prospective study. Crit Care Med. 2014;42(4):849–59. doi: 10.1097/CCM.0000000000000040 24247473 PMC 3959239 · doi ↗ · pubmed ↗
- 8Appleton RT, Kinsella J, Quasim T. The incidence of intensive care unit-acquired weakness syndromes: A systematic review. J Intensive Care Soc. 2015;16(2):126–36. doi: 10.1177/1751143714563016 28979394 PMC 5606476 · doi ↗ · pubmed ↗