Association of peripheral and CSF zinc levels with Parkinson's disease: A systematic review and meta-analysis
Rasoul Hossein Zadeh, Reza Hossein Zadeh, Sajjad Hajihosseini, Anahita Rahmati, Yasamin Moeinipour, Omid Salimi, Zahra Rastegar, Ali Molavi, Fateme Sedghi, Nasibeh Zerangian, Mahsa Asadi Anar, Alaleh Alizadeh, Haleh Alizadeh, Niloofar Deravi

TL;DR
This study finds that Parkinson's disease patients have lower zinc levels in blood, but not in cerebrospinal fluid, suggesting a possible link between zinc deficiency and the disease.
Contribution
The study provides a comprehensive meta-analysis of zinc levels in Parkinson's disease across different biological matrices and geographic regions.
Findings
PD patients have significantly lower serum and plasma zinc levels compared to controls.
Cerebrospinal fluid zinc levels show no significant difference in PD patients.
High heterogeneity in results suggests variability due to geographic and methodological factors.
Abstract
The possible involvement of numerous chemical elements in the pathogenesis of neurodegenerative diseases has long been studied by researchers, yet no clear consensus regarding the concentration of Zinc (Zn) and the onset of Parkinson's disease (PD) has emerged. The objective of this study was to conduct a robust meta-analysis to clarify the association between Zn levels across different biological matrices and Parkinson’s disease. A comprehensive literature search was conducted across six databases up to April 2024. We included 29 case-control studies reporting Zn concentrations in serum, plasma, and cerebrospinal fluid (CSF) and performed subgroup analyses by biological matrix, continent, and detection method to extend and update previous meta-analyses on this topic. Statistical meta-analysis was performed using STATA v18 software, calculating the weighted mean difference (WMD) and 95…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
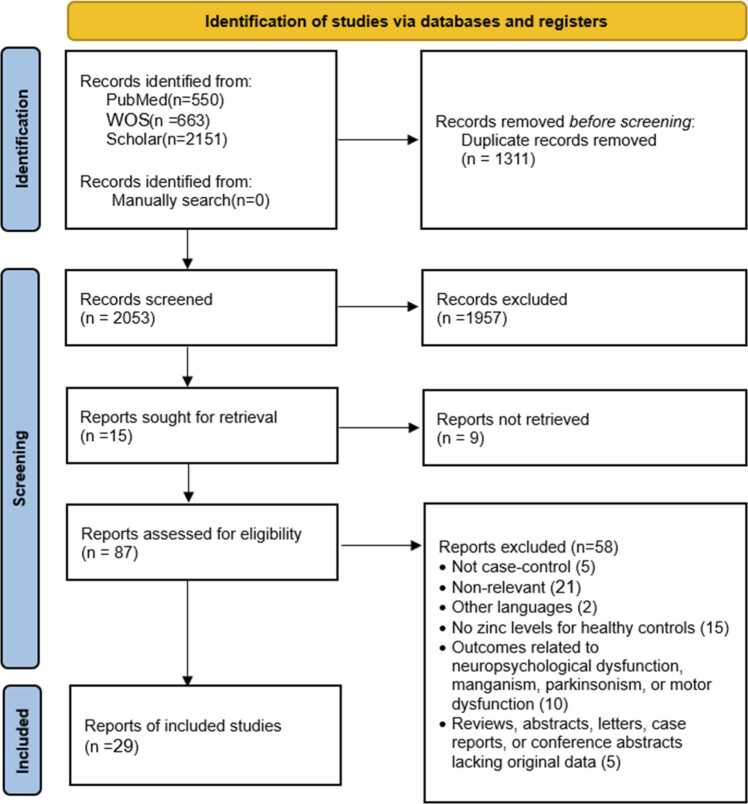 Figure 1
Figure 1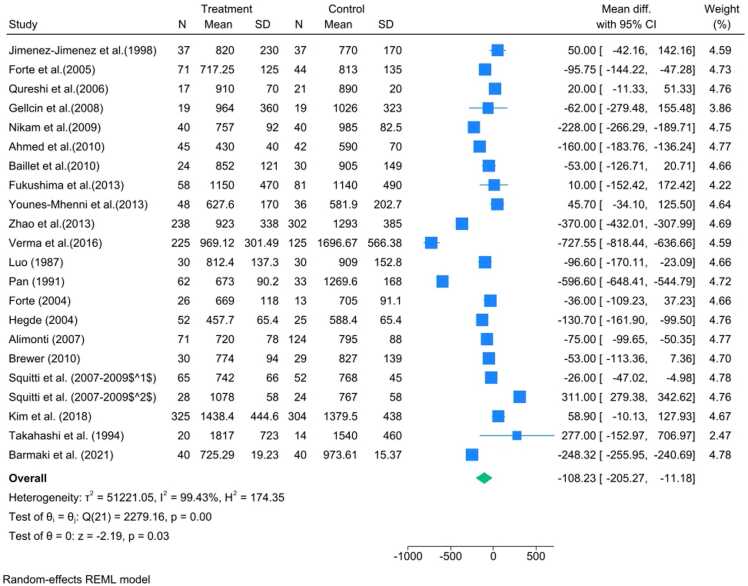 Figure 2
Figure 2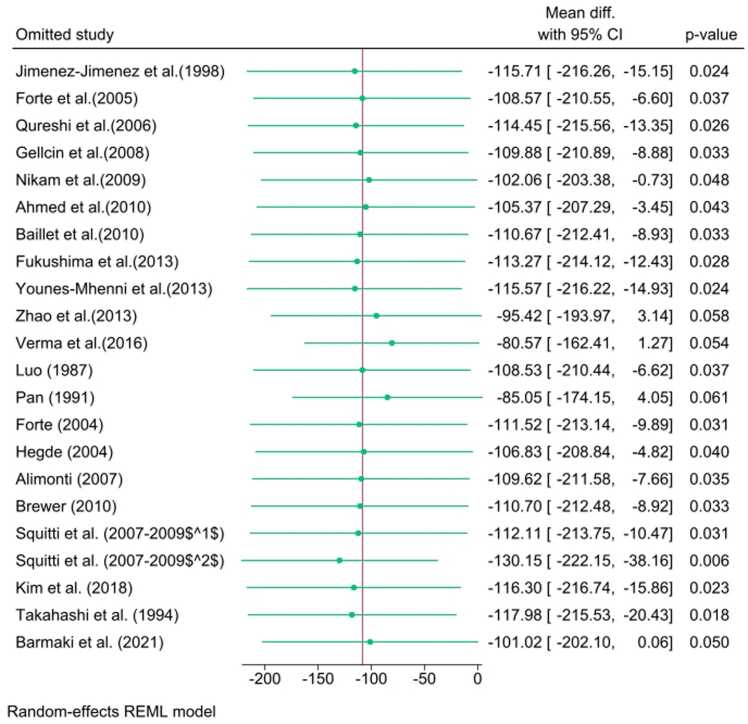 Figure 3
Figure 3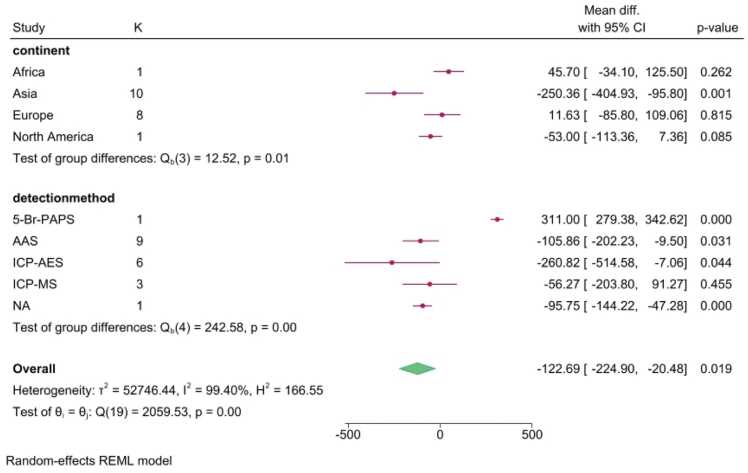 Figure 4
Figure 4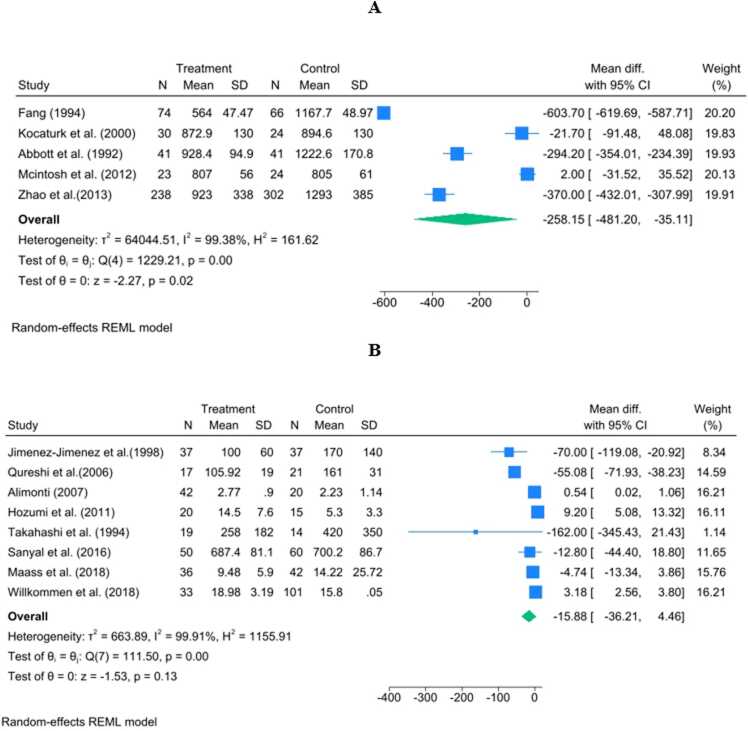 Figure 5
Figure 5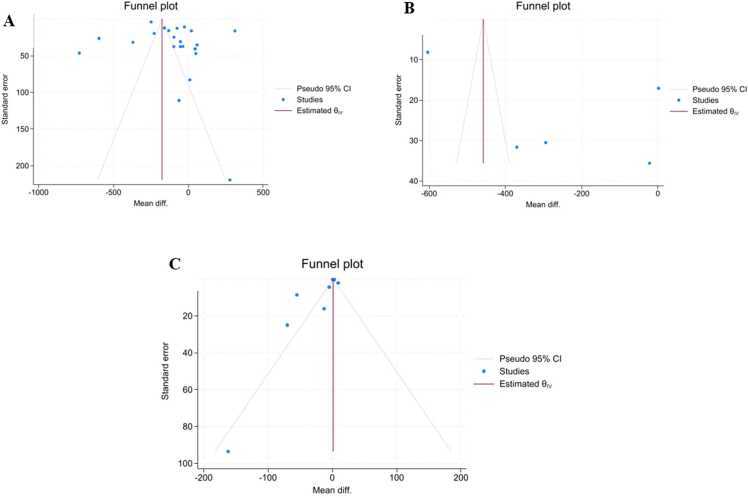 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrace Elements in Health · Parkinson's Disease Mechanisms and Treatments · Heavy Metal Exposure and Toxicity
Introduction
1
Parkinson's disease (PD), originally described by James Parkinson in 1817 and later studied by Jean-Martin Charcot, is a progressively advancing disorder of the central nervous system characterized by motor symptoms such as tremors, rigidity, and bradykinesia (Goetz, 2011, Airavaara et al., 2020). As the disease progresses, patients may also experience difficulty with postural stability. Prevalence of PD has been estimated to be approximately 0.5–1 % in the population aged 65–69 and increased to 1–3 % in the population aged 80 and above (Palakurthi and Burugupally, 2019, Khatib, 2022). Pathologically, PD presents as a decrease in dopaminergic cells that reside in the nigrostriatal tract (Airavaara et al., 2020). However, the neurodegenerative process goes beyond the substantia nigra and inhibits neurons in other neural circuits (Antonina Kouli and Kuan, 2018).
PD has been regarded as having a complex involvement with numerous influences by both genetic and environmental factors despite the elusive identification of its definitive etiology (Abbas et al., 2018, Kalia and Lang, 2015). One such environmental factor suggested to be implicated in PD includes the presence of abnormally elevated concentrations of various heavy metals and metalloids such as zinc (Zn) (Bjorklund et al., 2018, Giacoppo et al., 2014, Vinceti et al., 2018). Some epidemiological studies have revealed a correlation between PD and exposure to heavy metals, which may promote the generation of free radicals through processes such as the Fenton–Haber–Weiss reaction (Ball et al., 2019, Raj et al., 2021, Tchounwou et al., 2012, Vellingiri et al., 2022). Such reactive oxygen species (ROS) would potentially induce oxidative stress and cause mitochondrial dysfunction, DNA breaks, protein misfolding, and eventual neurodegenerative consequences (Vellingiri et al., 2022, Al-Harthi et al., 2022, Lee et al., 2023). On the other hand, various heavy metals such as Zn are crucial trace elements and perform as indispensable cofactors for many enzymes. Alterations in the amounts of heavy metals can negatively impact the nervous system and may play a role in the pathological processes found in PD (Atarod et al., 2022, Fraga, 2005, Tomita and Yoshikawa, 2002, Uversky et al., 2001).
Zn has a critical role in various pathways associated with PD, and beyond its general function as a trace mineral (Chen et al., 2025). As one of the cofactors for Cu/Zn superoxide dismutase, Zn plays a role in protecting against oxidative stress and maintaining mitochondrial function and redox homeostasis within dopaminergic neurons (Palma et al., 2020). Abnormal Zn levels raise α-synuclein aggregation and its interactions with other metal-binding proteins as well as potentially contributing to protein misfolding, oxidative stress, and nerve cell susceptibility in PD (Banik et al., 2025). Both chronic deficiency and excess of Zn can negatively affect the central nervous system; thus, this element has a dual effect on the central nervous system through imbalances (Chen et al., 2025, Nakagawa and Yamada, 2023).
Despite the clear biological importance of Zn status in neurodegeneration, existing observational studies linking Zn concentration to PD have produced inconsistent and conflicting results. This lack of agreement has been emphasized in several previous systematic reviews (Du et al., 2017, Sun et al., 2017, Adani et al., 2020), which reported differing effect sizes, especially across various biological matrices (serum, plasma, CSF) and regions. To address this ongoing uncertainty and provide an updated quantitative summary of this association, we conducted a comprehensive systematic review and meta-analysis. Our study updates earlier reviews by combining a larger amount of recent data and conducting detailed subgroup analyses to examine the impact of biological matrix and geographic origin. In contrast to previous meta-analyses that mainly focused on serum Zn or combined limited matrices, we included serum, plasma and CSF, used weighted mean differences expressed in μg/L, and systematically explored heterogeneity by continent and detection method to extend and refine prior evidence. We aimed to characterize the association between Zn levels in the peripheral circulation and CSF and PD risk, thereby assessing the potential of Zn status as a biomarker and highlighting priorities for future mechanistic and longitudinal studies.
Methods
2
Search strategy
2.1
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009), two independent researchers performed searches through different databases including PubMed, Embase, Cochrane Library, Scopus, Web of Science, and Google Scholar. The articles published up to the 20th of April 2024 were included in the search. A combination of Medical Subject Headings (MeSH) and text terms was employed and listed in Table 1. Moreover, we hand-checked the lists of references in the articles included in our analysis and other relevant reviews and meta-analyses to identify other publications.Table 1. Curated Search strategies for each chosen database and result of the searching procedure.Table 1. Data baseSearch strategyresultsPubMed((("Parkinson Disease"[Mesh]) OR ("Parkinson Disease"[Title/Abstract])) OR (parkinson[Title/Abstract])) AND (("Zinc"[Mesh]) OR (zinc[Title/Abstract]))550WOS(TS=("Parkinson Disease")) OR TS= (parkinson) AND TS= (zinc)663Scopus(TITLE-ABS-KEY ( zinc)) AND (TITLE-ABS-KEY (parkinson) OR TITLE-ABS-KEY ("parkinson disease"))2151
Inclusion/exclusion criteria and study selection
2.2
Selection of the articles that were eligible for inclusion relied on a pre-defined set. The inclusion criteria included: being an original research paper for peer review, a human observational study reporting Zn level in serum, plasma or CSF for PD and healthy controls, including English language articles and Parkinson's disease as the outcome. The exclusion criteria included: duplicate publications, studies on animals, and articles lacking original data such as reviews, case reports or abstracts and letters and conference abstracts. We also excluded studies that did not report Zn level for healthy control or whose outcomes were about neuropsychological dysfunction or manganism or parkinsonism or motor dysfunction.
Following the elimination of duplicate publications, all articles underwent screening based on their titles and abstracts to filter out irrelevant topics and articles that did not meet the inclusion criteria. Full texts of the remaining articles were obtained and evaluated by one reviewer. Any uncertainties were addressed through discussion with a second reviewer. When multiple publications stemmed from the same study, the most comprehensive and/or latest paper was considered for inclusion. Reanalyses of data from previously published studies that did not provide new insights on the relationship between Zn and Parkinson's disease were excluded. The study selection procedure is illustrated in Fig. 1.Fig. 1. Flow chart of the study selection procedure. Flow diagram illustrating the search strategy and study selection process conducted in accordance with the PRISMA guidelines. The process began with 3364 records and resulted in the final inclusion of 29 unique case-control studies for quantitative synthesis.Fig. 1
Data extraction
2.3
Two authors independently assessed each candidate article and extracted relevant information, including the surname of the first author, publication year, country or region, study design, sample size, age and gender distribution of participants, method of case identification and control selection, and the technique used for Zn level measurement (e.g., AAS, ICP-MS). Additionally, the average Zn levels and their respective standard deviations (SD) were systematically documented, or accurately approximated from median values, ranges, and sample sizes when not explicitly provided.
Risk of bias assessment
2.4
Joanna Briggs Institute (JBI) (https://jbi.global/critical-appraisal-tools) critical appraisal checklists were used for evaluating the methodological quality of the articles. Two reviewers independently conducted the quality assessment of all included articles. Any discrepancies were deliberated between the two reviewers, and if a consensus could not be reached, a third reviewer intervened to resolve the disagreement.
Statistical analysis
2.5
A meta-analysis was conducted using Zn level data in serum, plasma, or CSF expressed as mean ±SD or standard error of the mean (SEM). The primary outcome was the weighted mean difference (WMD), along with 95 % confidence intervals (CIs). The random-effects model (REML) was utilized to combine the study-specific effect estimates, accounting for the anticipated substantial heterogeneity among studies. Heterogeneity was rigorously assessed using the Chi-square (Q) and I-square (I^2^) tests (Higgins and Thompson, 2002, DerSimonian and Kacker, 2007). A subgroup analysis was performed to investigate the factors contributing to heterogeneity, stratified by continent and detection method. Data points extracted from graphical representations in studies were precisely digitized using WebPlot Digitizer (Automeris LLC, Frisco, Texas) (Rohatgi, 2023). All statistical analyses were performed using STATA statistical software (version 18), with all tests being two-tailed. Statistical significance was predetermined at a p-value < 0.05.
Publication bias assessment
2.6
Publication bias was assessed visually using funnel plots and statistically by employing Begg's rank correlation test and Egger's linear regression test (Duval and Tweedie, 2000a, Duval and Tweedie, 2000b, Egger et al., 1997).
Sensitivity analysis
2.7
To evaluate the robustness of the overall pooled estimates, a sensitivity analysis was carried out using the one-study-removed method to evaluate the impact of a specific study on the overall estimation of effects (Alexander et al., 2000).
Results
3
Study selection and baseline characteristics
3.1
Our systematic search process, executed according to the PRISMA guidelines, yielded an initial total of 3364 records across all databases. Following the removal of 1311 duplicate records, the remaining 2053 articles underwent title and abstract screening. This screening step led to the exclusion of 1957 reports. Subsequently, 15 reports were initially sought for retrieval, although this number was later supplemented by hand-checking and other searches, resulting in 87 full-text articles being assessed for eligibility. Of these, 58 reports were excluded due to reasons such as not being a case-control study, lacking Zn levels for healthy controls, being published in other languages, or lacking original data. The detailed exclusion process is depicted in the PRISMA flow diagram (Fig. 1).
The rigorous selection process ultimately identified 29 unique case-control studies that met all predefined inclusion criteria and were included in the quantitative meta-analysis. These studies incorporated data across three biological matrices: serum, plasma, and cerebrospinal fluid (CSF). The baseline characteristics, including country of origin, sample size, age, gender distribution, and Zn detection method for all 29 included studies, are summarized in Table 2. The methodological quality of these studies, assessed using the JBI checklists, ranged from 8 to 10.Table 2. Summarizes the characteristics of the included studies.Table 2**First Author et al. (Year)Specimen TypeContinentN-CaseAge of Cases (Mean ± SD)****Sex in Cases (Female %)****Zinc in Cases Mean (SD) (μg/L)N-ControlAge of Controls (Mean ± SD)****Sex in Controls (Female %)**Zink in Controls Mean (SD) (μg/L)Detection MethodJBI ScoreJimenez-Jimenez et al. (1998)SerumSpain3765.7 ± 8.862.16 % (23 F/37 N)820 (230)3762.4 ± 17.856.76 % (21 F/37 N)770(170)AAS9/10Forte et al. (2005)SerumItaly7165.5 ± 9.474.65 % (53 F/71 N)717.25 (125)4451.9 ± 4.075.00 % (33 F/44 N)813(135)NA8/10Qureshi et al. (2006)SerumSweden1770 ± 1558.82 % (10 F/17 N)910 (70)2162 ± 1161.90 % (13 F/21 N)890 (20)AAS8/10Gellcin et al. (2008)SerumNorway19NA52.63 % (10 F/19 N)994 (360)19NA51.51 % (51 F/99 N)1026(323)ICP-MS9/10Nikam et al. (2009)SerumIndia4040 −80 (Range)NA757.0 (92)40NANA985(82.5)AAS9/10Ahmed and Santosh (2010)SerumIndia4557.6 ± 937.78 % (17 F/45 N)430 (40)4255.6 ± 3.345.24 % (19 F/42 N)590(70)ICP-MSBaillet et al. (2010)SerumFrance2460.8 ± 6.529.17 % (7 F/24 N)851.9 (121)3060.2 ± 5.163.33 % (19 F/30 N)905(149)AAS8/10Fukushima et al. (2010)SerumChina5863.95 ± 9.4060.34 % (35 F/58 N)1150 (470)8163.65 ± 9.3558.02 % (35 F/81 N)1140(490)ICP-AES9/10Younes-Mhenni et al. (2013)SerumTunisia4865.8 ± 10.245.83 % (22 F/48 N)627.6 (170)3659.7 ± 12.161.11 % (22 F/36 N)581.9(202.7)AAS9/10Zhao et al. (2013)SerumChina23866.6 ± 11.350.84 % (121 F/238 N)923 (338)30265.6 ± 12.249.83 % (151 F/302 N)1293(385)AAS9/10Verma et al. (2016)SerumIndia22556.84 ± 8.8227.11 % (61 F/225 N)969.12 (301.49)12557.24 ± 7.9728.00 % (35 F/125 N)1696.67(566.38)ICP-AES9/10Luo et al. (1987)SerumChina3061.5 ± 8.40.00 % (0 F/30 N)812.4(137.3)30> 450.00 % (0 F/30 N)909(152.8)AAS8/10Pan (1991)SerumChina6255.4 ± 9.137.10 % (23 F/62 N)673(90.2)3352.3 ± 12.863.64 % (21 F/33 N)1269.6(168)ICP-AES8/10Forte et al. (2004)SerumItaly2664.9 ± 10.869.23 % (18 F/26 N)669(118)1363.8 ± 13.761.54 % (8 F/13 N)705(91.1)ICP-AES9/10Hegde et al. (2004)SerumIndia5258.1 ± 4.746.15 % (24 F/52 N)457.7(65.4)2555.4 ± 6.448.00 % (12 F/25 N)588.4(65.4)ICP-AES9/10Alimonti et al. (2007)SerumItaly7165.5 ± 9.425.35 % (18 F/71 N)720(78)12444.8 ± 12.734.68 % (43 F/124 N)795(88)ICP-AES8/10Brewer et al. (2010)SerumUS3067.4 ± 8.240 % (12 F/30 N)774(94)2968.6 ± 669 % (20 F/29 N)827(139)AAS9/10Squitti et al. (2009)SerumItaly2868.3 ± 11.128.57 % (8 F/28 N)1078(58)2466.9 ± 9.554.17 % (13 F/24 N)767(58)5-Br-PAPS8/10Kim et al. (2018)SerumKorea32565.2 ± 8.746.15 % (150 F/325 N)1438.4(444.6)30464.4 ± 9.353.62 % (163 F/304 N)1379.5(438)ICP-MS10/10Barmaki et al. (2021)SerumIran4065.70 ± 6.3232.5 % (13 F/40 N)725.29(19.23)4064.35 ± 3.7545 % (18 F/40 N)973.61(15.37)AAS9/10Takahashi et al. (1994)SerumAsia2061.4 ± 9.3NR1817 ± 7231460.8 ± 8.9NR1540 ± 460PIXE9/10Fang (1994)PlasmaChina7456.2 ± 10.847.30 % (35 F/74 N)564(47.47)6653.7 ± 14.250.00 % (33 F/66 N)1167.7(48.97)AAS9/10Kocaturk et al. (2000)PlasmaTurkey3064.0 ± 0.0NA (NA F/30 N)872.9(130)2461.0 ± 0.0NA (NA F/24 N)894.6(130)NA9/10Abbott et al. (1992)PlasmaUK4162 ± 948.78 % (20 F/41 N)928.4(94.9)4158 ± 948.78 % (20 F/41 N)1222.6(170.8)NA9/10Mcintosh et al. (2012)PlasmaUS2370 ± 952.17 % (12 F/23 N)807(56)2473 ± 658.33 % (14 F/24 N)805(61)NA8/10Jimenez-Jimenez et al. (1998)CSFSpain3765.7 ± 8.862.16 % (23 F/37 N)100(60)3762.4 ± 17.856.76 % (21 F/37 N)170(140)AAS9/10Qureshi et al. (2006)CSFSweden1770 ± 1558.82 % (10 F/17 N)105.92 (19)2162 ± 1161.90 % (13 F/21 N)161 (31)ICP-AES9/10Alimonti (2007)CSFItaly4264.5 ± 10.752.38 % (22 F/42 N)2.77(0.9)2066.2 ± 14.770.00 % (14 F/20 N)2.23(1.14)ICP-MS9/10Hozumi et al. (2011)CSFJapan2068.7 ± 5.855.00 % (11 F/20 N)14.5(7.6)1548.4 ± 22.260.00 % (9 F/15 N)5.3(3.3)ICP-MS10/10Takahashi et al. (1994)CSFJapan1961.4 ± 9.3NA258 (182)1460.8 ± 8.9NA420 (350)PIXE9/10Sanyal et al. (2016)CSFIndia5058.7 ± 12.432.00 % (16 F/50 N)687.4(81.1)6060.1 ± 10.430.00 % (18 F/60 N)700.2(86.7)ICP-MS9/10Maass et al. (2018)CSFGermany3665.5 ± 13.133.33 % (12 F/36 N)9.48(5.9)4267 ± 1142.86 % (18 F/42 N)14.22(25.72)NA9/10Willkommen et al. (2018)CSFGermany3365.1 ± 12.930.30 % (10 F/33 N)18.98(3.19)10144.8 ± 17.362.38 % (63 F/101 N)15.8(0.05)NA10/10
Zinc concentration meta-analysis
3.2
The meta-analysis was performed using the WMD (μg/L) for Zn levels across three matrices to quantify the association between Zn status and Parkinson’s disease (PD) susceptibility.
Zinc in serum
3.2.1
The pooled results for serum Zinc (N=22 data points) revealed a statistically significant reduction in PD patients when contrasted with healthy controls. The overall effect demonstrated a WMD of −108.23 μg/L (95% CI:[−205.27,−11.18]), with a high level of significance (p=0.03). This finding was accompanied by extreme heterogeneity (I2=99.43%), indicating considerable variance across the studies included (Fig. 2).Fig. 2. Forest plot of Zinc levels in serum for Parkinson's disease (PD) patients versus controls. Forest plot displaying the Weighted Mean Difference (WMD) in serum Zinc concentration (μg/L) for individual studies and the pooled estimate. The overall analysis showed a significant reduction in PD patients (WMD=−108.23 μg/L, 95% CI: [−205.27,- 11.18], p=0.03). The analysis was characterized by extreme heterogeneity (I2=99.43%). The diamond represents the pooled effect size under the random-effects REML model.Fig. 2
Subgroup analysis was performed to investigate potential sources of this high heterogeneity. Stratification by continent indicated that the significant Zinc deficit was primarily driven by the Asian subgroup (WMD=−220.69 μg/L, p=0.006). Furthermore, stratification by detection method confirmed a significant reduction in studies utilizing AAS, NA and ICP-AES (Fig. 3).Fig. 3. Sensitivity analysis of serum Zinc levels using the one-study-removed method. Sensitivity plot showing the recalculated pooled WMD in serum Zn concentration after iteratively excluding each study. The plot demonstrates the robustness of the overall finding, as the pooled effect remained statistically significant and consistently negative regardless of which single study was omitted.Fig. 3
Sensitivity analysis, conducted using the one-study-removed method, confirmed the robustness and stability of the overall pooled estimates across all three matrices. The sequential omission of any single study did not significantly alter the primary conclusion of reduced Zn levels in the serum (Fig. 4).Fig. 4. Subgroup plot illustrating the effect of different covariates on the WMD in serum Zinc levels. The analysis confirmed that geographical location was a significant source of heterogeneity, with the Asian subgroup showing the most significant deficit (WMD=−220.69 μg/L, p=0.006). Significant differences were also noted across analytical detection methods (AAS, ICP-AES, and NAFig. 4
Zinc in plasma
3.2.2
The analysis of the plasma matrix (N = 4 studies) corroborated the serum findings, showing a deeper and statistically significant reduction in Zn levels among PD patients. The pooled WMD was −258.15 μg/L (95 % CI:[−481.20,−35.11]), with a significant overall effect (p = 0.02). This analysis was also characterized by extremely high heterogeneity (I2 =99.38 %), primarily reflecting the substantial discrepancies in effect size among the limited number of contributing studies (Fig. 5A).Fig. 5. Forest plots of Zn levels in the plasma and CSF matrices. Forest plots summarizing the WMD in Zn concentration (μg/L) for the plasma and CSF matrices in PD patients versus controls. Panel A shows plasma Zn, with a significantly lower level in PD patients (WMD = −258.15 μg/L, 95 % CI: [−481.20, −35.11], p = 0.02) across four studies. Panel B shows CSF Zn, where no statistically significant overall difference was observed between PD patients and controls (WMD=−15.88 μg/L, 95% CI:[−36.21,4.46], p=0.13) across eight studies.Fig. 5
Zinc in cerebrospinal fluid (CSF)
3.2.3
The combined findings for Zinc levels in CSF (N=8 studies) revealed no statistically significant overall difference between PD patients and healthy controls. The pooled WMD was −15.88 μg/L (95% CI:[−36.21,4.46]), with a non-significant p−value of 0.13. This analysis exhibited the highest level of heterogeneity (I2=99.91%), resulting from the severe directional conflicts reported by individual studies (Fig. 5B).
Publication bias and sensitivity
3.3
Sensitivity analysis, carried out using the one-study-removed method, showed that excluding any single study did not significantly alter the pooled analysis, confirming the robustness of the overall findings across all three matrices.
Publication bias was evaluated using Begg's test and Egger's test, and visually inspected via funnel plots (Fig. 6). Overall, the funnel plots and formal tests did not indicate substantial publication bias, although the Egger’s test result for CSF (p=0.0029) should be interpreted cautiously in light of the limited number of studies and extreme heterogeneity:
- •Serum: Begg's p=0.4298; Egger's p=0.2951.
- •Plasma: Begg's p = 0.8065; Egger's p = 0.3751.
- •CSF: Begg's p=0.5362; Egger's p=0.0029. Fig. 6. Funnel plots illustrating publication bias in the meta-analysis of Zinc levels. Funnel plots visually assessing publication bias for the three biological matrices in the meta-analysis of Zn levels. Panel A shows serum, panel B plasma and panel C CSF. The relative symmetry observed in the funnel plots, together with the formal tests, did not indicate substantial publication bias overall, although the CSF findings should be interpreted cautiously.Fig. 6
Discussion
4
The principal finding of this comprehensive meta-analysis is the consistent and statistically significant reduction in Zn concentration in the peripheral circulation (serum and plasma) of Parkinson's disease (PD) patients compared to healthy controls. Specifically, the pooled WMD of −122.69 μg/L in serum and −258.15 μg/L in plasma demonstrates a substantial systemic deficit, supporting the hypothesis that lower Zn levels are associated with PD and may contribute to oxidative stress, while not establishing a causal role in the disease’s pathogenesis. The strength of this association is corroborated by the absence of significant publication bias in all three matrices (serum: Begg's p = 0.6732, Egger's p = 0.8329).
However, the interpretation of the overall effect is significantly complicated by the extreme heterogeneity (I2 >99 %) observed across all three matrices. Our analysis indicated that only geographical location had a significant impact on this high heterogeneity. Subgroup analysis revealed that the statistically significant Zn deficit was overwhelmingly concentrated in Asian nations (WMD=−250.36 μg/L, p = 0.001), while Western countries did not demonstrate any significant overall relationships. This geographical variation aligns with the findings of other independent meta-analyses, suggesting that regional differences in dietary Zn intake, environmental exposures, or genetic background are pivotal sources of the observed discrepancies. Furthermore, the high heterogeneity was amplified by methodological variances; the significant WMD reductions from AAS and ICP-AES were countered by an opposing, significant increase reported by the single outlier study using the 5-Br-PAPS method (WMD=311.00 μg/L).
In stark contrast to the clear peripheral deficit, the meta-analysis of CSF Zn levels found no statistically significant overall difference (WMD=−11.96 μg/L, p = 0.23). This non-significant finding, coupled with the highest heterogeneity (I2 =99.91 %), is particularly challenging. The profound directional conflict among individual CSF studies—some reporting significant decreases (Qureshi et al., 2006, Jimenez-Jimenez et al., 1998), others reporting significant increases (Alimonti et al., 2007, Hozumi et al., 2011) —suggests a complex Zn compartmentalization issue in the CNS rather than a simple global deficit. This indicates that the peripheral status may not accurately mirror the micro-environmental balance of Zn across the Blood-Brain Barrier (Qi and Liu, 2019).
The observed peripheral Zn deficiency is mechanistically supported by Zn's role as a potent anti-oxidant (Kiouri et al., 2023). Zn is a primary cofactor for antioxidant enzymes such as Superoxide Dismutase (SOD), catalase, and peroxidase. Decreased Zn levels compromise the activity of key antioxidant enzymes like Cu/Zn SOD and reduce Zn metallothionein activity, thereby inducing oxidative stress and elevating free radicals, which leads to cellular deterioration and necrosis in dopaminergic neurons (Sofo et al., 2018, Mariani et al., 2008, Kavian et al., 2022). Additionally, Zn inhibits the production of ROS by competing with redox-active metal ions like Copper (Cu) and Iron (Fe) for binding sites on cellular macromolecules (Qureshi et al., 2006). The age of the PD patient is also a primary complicating factor; our meta-analysis revealed that all included studies, with patient mean ages ranging from 59.3 to 71.66 years, were significantly impacted by age, suggesting a potential role for age in the outcome of heterogeneity (McMillan et al., 2021). Beyond these antioxidant effects, dysregulated Zn homeostasis can modulate α-synuclein aggregation and its interaction with metallothioneins and other metal-binding proteins, potentially influencing mitochondrial dysfunction and neuronal vulnerability in PD (Chen et al., 2025, Nakagawa and Yamada, 2023).
This comprehensive meta-analysis significantly strengthens the evidence for a systemic Zn deficit in PD patients, largely mirroring and extending the findings of previous major meta-analyses. For instance, Du et al (Du et al., 2017). reported a significant reduction in serum Zn (SMD=−0.59) and a reduced Zn level when combining serum and plasma data (SMD=−0.60), results that align closely with our own observation of a statistically significant WMD in both serum and plasma. Similarly, Sun et al (Sun et al., 2017)., focusing solely on serum, found a significant SMD of −0.779 and also highlighted the strong effect observed in Asian studies, which we meticulously confirmed and quantified through our detailed subgroup analysis (WMD=−250.36 μg/L). Our study contributes to this body of work by providing results expressed in μg/L (WMD) from a larger number of studies, offering a more clinically interpretable metric than the SMD used in many earlier reports.
In addition to the corroboration of earlier meta-analyses, there are a number of new contributions made by our work. First, we included a greater number of case-control studies and provided evaluations as of April 2024. Secondly, all studies evaluated Zn in the form of plasma, serum and CSF together to facilitate more clinically relevant pooled effect estimates (WMD expressed as μg/L). Lastly, we were able to show that deficits in peripheral Zn levels are primarily attributed to Asian populations and to certain types of analytical methods through pre-specified subgroup analyses of cases and controls conducted by continent and Zn detection method, and thus we refined previous estimates and produced new hypotheses through the introduction of an increased number of case-control studies and the inclusion into the dataset of other variables associated with peripheral Zn levels.
A crucial point of comparison and innovation in our study lies in the detailed analysis of the CSF compartment, a feature also explored by Adani et al (Adani et al., 2020). While Du et al (Du et al., 2017) observed a non-significant trend toward reduced CSF Zn levels, the contradictory findings and the high I2 (99.91 %) in our analysis demand a more cautious interpretation: the core issue is likely related to dysregulated transport of Zn across the Blood-Brain Barrier (BBB), where Zn transporters ZnTs and ZIPs may be impaired, rather than a simple CNS deficiency. This finding is consistent with the general conclusion of Adani et al. (2020) that methodological factors, including the type of biological sample and detection technique, strongly influence the heterogeneity and final pooled estimates. While peripheral Zn levels seem to be a consistent risk indicator at the systemic level, how CNS Zn is affected remains highly debated and may depend on regional compartmentalization and disease stage. Future studies using advanced imaging or post-mortem analysis are necessary to accurately map Zn distribution and understand the role of Zn-regulating proteins in Parkinson's disease brains. Although our results indicate a systemic Zn deficit in peripheral circulation, maintaining overall Zn balance is crucial, as both deficiency and excess can be detrimental to neuronal integrity. It's equally important to investigate the impacts of Zn overload, which can lead to neurotoxicity and the production of reactive oxygen species. The diverse and often conflicting data in CSF may partly stem from local regulatory issues caused by Zn deficiency or excess within the central nervous system environment.
The results of our meta-analysis are robust at the statistical level, with the sensitivity analysis showing that excluding any single study did not materially change the overall findings. However, we must acknowledge that all studies were case-control investigations (with only one being prospective), which are inherently susceptible to reverse causation. The observed Zn deficit may partly reflect consequences of PD itself like impaired nutritional status or disease-related metabolic changes),rather than a primary etiological risk factor. This potential for bias, along with the lack of detailed data on key confounding factors like disease stage, duration, drug use, and exact gender distribution in the existing literature, necessitates caution in interpreting causation. The limitation of only including English-language studies also introduced selection bias. Further study using robust longitudinal design methodologies will be required to confirm our current results definitively.
Conclusion
5
In conclusion, our evidence demonstrates a consistent association between decreased Zn levels in the peripheral circulation (serum and plasma) and Parkinson’s disease susceptibility, although substantial between-study heterogeneity warrants cautious interpretation. These findings are compatible with a potential contribution of Zn deficiency to oxidative stress in PD, but they do not establish a causal role for Zn imbalance in PD pathogenesis. Our findings reiterate the necessity of large-scale longitudinal cohort studies to validate this association, clarify the direction of causality, and rigorously evaluate whether correcting Zn deficiency has any therapeutic value in the prevention or progression of PD.
List of abbreviations
AASAtomic Absorption SpectrometryBBBBlood-Brain BarrierCIConfidence IntervalCNSCentral Nervous SystemCSFCerebrospinal FluidCuCopperFeIronI^2^I-square test (Heterogeneity statistic)ICP-AESInductively Coupled Plasma-Atomic Emission SpectrometryICP-MSInductively Coupled Plasma-Mass SpectrometryMeSHMedical Subject HeadingsNOSNewcastle-Ottawa ScalePDParkinson's DiseasePRISMAPreferred Reporting Items for Systematic Reviews and Meta-AnalysesQChi-square test (Heterogeneity statistic)REMLRestricted Maximum LikelihoodROSReactive Oxygen SpeciesSDStandard DeviationSEMStandard Error of the MeanSMDStandardized Mean DifferenceSODSuperoxide DismutaseWMDWeighted Mean DifferenceZnZinc
Ethical approval
This systematic review and meta-analysis of previously published studies did not involve human participants or animal subjects. Therefore, an ethical review was not required.
Compliance with ethical standards statement
This systematic review and meta-analysis involved no direct human or animal experimentation, and all data was extracted from previously published studies. Therefore, ethical approval and informed consent were obtained by the original study authors, as per their respective institutional guidelines.
Sources of support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CRediT authorship contribution statement
Ali Molavi: Writing – original draft. Omid Salimi: Writing – original draft. Zahra Rastegar: Writing – original draft. Mahsa Asadi Anar: Writing – original draft. Alaleh Alizadeh: Writing – review & editing, Supervision, Project administration, Conceptualization. Rasoul Hossein Zadeh: Writing – original draft. Fateme Sedghi: Writing – original draft. Nasibeh Zerangian: Writing – original draft. Anahita Rahmati: Writing – original draft. Yasamin Moeinipour: Writing – original draft. Haleh Alizadeh: Writing – review & editing. Reza Hossein Zadeh: Writing – original draft. Niloofar Deravi: Writing – review & editing. Sajjad Hajihosseini: Writing – original draft.
Declaration of Generative AI and AI-assisted technologies in the writing process
AI was used to paraphrase the text.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abbas M.M.Xu Z.Tan L.C.S.Epidemiology of Parkinson's Disease-East Versus West Mov. Disord. Clin. Pract.51201814283036334210.1002/mdc 3.12568 PMC 6174379 · doi ↗ · pubmed ↗
- 2Abbott R.A.Cox M.Markus H.Tomkins A.Diet, body size and micronutrient status in Parkinson's disease Eur. J. Clin. Nutr.461219928798841483417 · pubmed ↗
- 3Adani G.Filippini T.Michalke B.Vinceti M.Selenium and other trace elements in the etiology of Parkinson’s disease: a systematic review and meta-analysis of case-control studies Neuroepidemiology 54120201233145480010.1159/000502357 · doi ↗ · pubmed ↗
- 4Ahmed S.S.Santosh W.Metallomic profiling and linkage map analysis of early Parkinson's disease: a new insight to aluminum marker for the possible diagnosis P Lo S One 562010 e 1125210.1371/journal.pone.0011252 PMID: 20582167; PMCID: PMC 288981920582167 PMC 2889819 · doi ↗ · pubmed ↗
- 5Airavaara M.Parkkinen I.Konovalova J.Albert K.Chmielarz P.Domanskyi A.Back and to the future: from neurotoxin-induced to human Parkinson's disease models Curr. Protoc. Neurosci.9112020 e 8810.1002/cpns.8832049438 · doi ↗ · pubmed ↗
- 6Alexander J.Sutton K.R.A.Jones David R.Sheldon Trevor A.Song Fujian Methods for Meta-Analysis in Medical Research 2000 Wiley
- 7Al-Harthi S.Kharchenko V.Mandal P.Gourdoupis S.JaremkoŁ.Zinc ions prevent α-synuclein aggregation by enhancing chaperone function of human serum albumin Int. J. Biol. Macromol.222Pt B 2022287828873625262210.1016/j.ijbiomac.2022.10.066 · doi ↗ · pubmed ↗
- 8Alimonti A.Bocca B.Pino A.Ruggieri F.Forte G.Sancesario G.Elemental profile of cerebrospinal fluid in patients with Parkinson's disease J. Trace Elem. Med. Biol.21420072342411798081410.1016/j.jtemb.2007.05.001 · doi ↗ · pubmed ↗