Prebiotics, probiotics, and synbiotics and maternal mental health during pregnancy and postpartum period: a systematic review
Sandra Martín-Peláez, Luis Miguel Martín-delosReyes, Naomi Cano-Ibáñez

TL;DR
This review examines whether prebiotics, probiotics, and synbiotics can help prevent depression and anxiety in pregnant and postpartum women without prior mental health issues.
Contribution
The study is the first systematic review to evaluate the potential of gut microbiota-targeted dietary interventions in preventing maternal mental health disorders.
Findings
Probiotics showed small but significant reductions in depressive and anxiety symptoms during pregnancy.
One trial found significantly lower depressive scores in the probiotic group postpartum.
No studies on prebiotics or synbiotics were found, and evidence remains limited due to heterogeneity.
Abstract
Depression and anxiety are common during pregnancy and postpartum, affecting both mothers’ and offspring health. Emerging research suggests gut microbiota may influence these conditions, providing a potential non-pharmacological approach for primary prevention, particularly in women without a prior mental health diagnosis. To assess the effect of prebiotics, probiotics, and synbiotics as dietary interventions targeting gut microbiota for preventing mental health disorders during pregnancy and postpartum in women without diagnosed mental health disorders. The protocol was prospectively registered in PROSPERO (CRD42024576678). A comprehensive search of MEDLINE, EMBASE, CINAHL, The Cochrane Library (CENTRAL), Scopus, and Web of Science from inception to March 2025, without language restriction. Randomized controlled trials (RCTs) involving pregnant or early postpartum women without a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
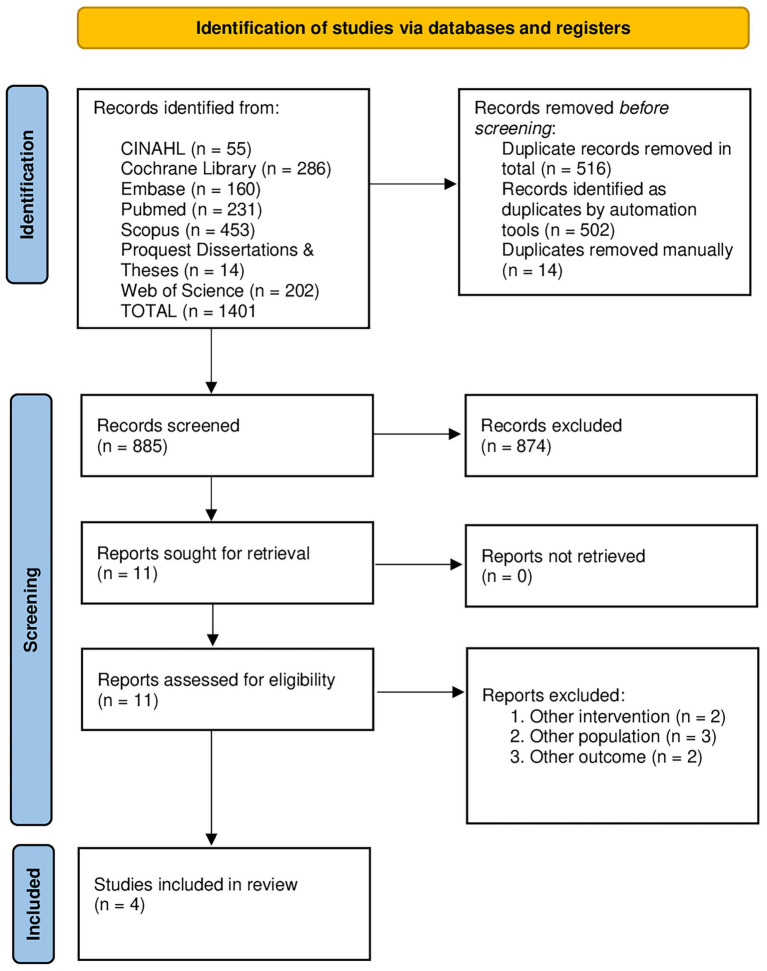 Figure 1
Figure 1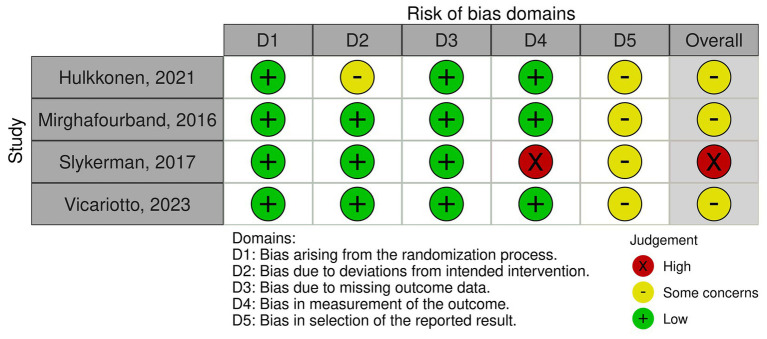 Figure 2
Figure 2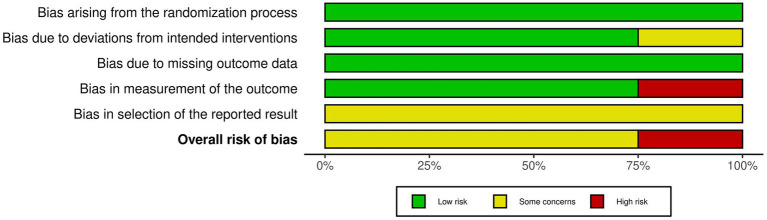 Figure 3
Figure 3| Author, year | Country | RCT design | Population | ||
|---|---|---|---|---|---|
| Sample Size (intervention/Control) | Inclusion criteria | Exclusion criteria | |||
| Hulkkonen et al. ( | Finland | Double-blind, 2×2 factorial parallel groups | 1) Age: Not specified | Multifetal pregnancy, the presence of inflammatory, metabolic or gastrointestinal diseases diagnosis or history of coagulopathy, and use of anticoagulants. The women who became pregnant again before 12 months postpartum were excluded from the postpartum analyses | |
| Mirghafourvand et al. ( | Iran | Triple-blind, two parallel groups | 1) Age: >18 years | Receiving any treatment in less than a week before the study, having mental retardation or metabolic disease (hypothyroidism), Hirschsprung disease, spinal anomalies, anorectal pathology, inflammatory of bowel disease, previous gastrointestinal surgery and use of fermented dairy products containing probiotics 2 weeks prior to the study | |
| Slykerman et al. ( | New Zealand | Double-blind, two center | 1) Age: >16 years | Women were excluded from the study if aged < 16 years, planning to move outside the study centers during study duration, planning on taking probiotics, or if they had serious medical or health problems related to the pregnancy | |
| Vicariotto et al. ( | Italy | Double-blind, multicenter, two parallel groups | 1) Age 18–50 years old | 1) Subjects who do not meet the inclusion criteria | |
| Author, year | Intervention | Control** | Mental health outcomes | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Type | Bacterial strains | Dose | Duration | Type | Type | Test | Period | Results | |
| Hulkkonen et al. ( | Fish oil and Probiotics* | 1 capsule/day containing 10^10 CFU per strain | Enrolment (≤18 GW) to 6 months postpartum | Placebo for the probiotics: capsule containing microcrystalline cellulose | Depressive and anxiety symptoms | EPDS (Ediburgh Posnatal Depression Scale) | Early pregnancy and late pregnancy and at three, six and 12 months postpartum | No differences among intervention groups and placebo | |
| Mirghafourvand et al. ( | Probiotics | 300 grams of yogurt containing 4.8 × 10^10 CFU (combined strains), 100 g x three times a day | Four weeks | Conventional yogurt, identical appearance | Quality of life | SF-36 (Quality of life questionnaire) | At baseline and at the end of week 6 | No differences among intervention group and placebo | |
| Slykerman et al. ( | Probiotic | 1 capsule/day containing 6 × 10^9 CFU | Enrolment until birth and, from birth up till 6 months post-birth whilst breastfeeding | Capsules containing corn-derived maltodextrin, identical appearance | Depressive and anxiety symptoms | EPDS (Ediburgh Posnatal Depression Scale) | Mothers (baseline and after 6 months or 12 months after delivery) completed the surveys based on how they remember they felt when their child was 1–2 months old | Depression: The intervention group reported significantly lower scores (7.7 ± 5.4) than placebo (9.0 ± 6.0). | |
| Vicariotto et al. ( | Probiotics and plus multivitamin food supplement | 1 capsule/day containing 4 × 10^9 CFU/day (2 × 10^9 CFU for each strain) | 90 days | The same capsules without the probiotic strains (identical appearance) | Postpartum depression symptoms | EPDS (Ediburgh Posnatal Depression Scale) | 45 days after the beginning of the treatment and final visit (i.e., 90 days after the beginning of the treatment) | At day 45, the intervention group showed a significantly lower mean score (9.0 ± 4.8) compared to the control group (12.1 ± 5.9) ( | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGut microbiota and health · Maternal Mental Health During Pregnancy and Postpartum · Tryptophan and brain disorders
Introduction
1
Maternal mental health disorders affect about one in five women during pregnancy and the first postpartum year, with depression and anxiety being most common conditions (1). These disorders are linked to adverse outcomes for both maternal well-being and infant development (2). Although pharmacotherapy is a mainstay treatment, concerns about maternal and fetal safety have increased interest in alternative approaches (3). Non-pharmacological interventions, such as cognitive-behavioural therapy and exercise, have shown potential benefits (4). Recent studies suggest a relationship between maternal mental health disorders and the gut microbiota through the gut–brain axis (5). The gut microbiota influences the central nervous system via autonomic, hormonal and immune pathways and has been associated with psychological disorders (6–8). Pregnancy induces physiological changes in gut microbiota composition (9, 10), while environmental disturbances may negatively affect maternal biology and mental health (11, 12). Maternal microbiota perturbations may influence offspring development through microbiota-derived fetal programming and early-life microbial transmission from mother to infant (13, 14).
Importantly, gut microbiota composition is modifiable through lifestyle factors, particularly diet. Dietary patterns, specific nutrients, and microbiota-targeted interventions such as probiotics, prebiotics and synbiotics have shown mental health benefits (15–18). Despite growing interest in microbiota-targeted interventions, evidence on their role in primary prevention of maternal mental health problems remains limited (19–21). In this context, prevention refers to interventions applied in women without a prior clinical diagnosis, aimed at reducing symptom severity or the risk of progression to clinically relevant disorders, rather than preventing formally diagnosed conditions. Previous systematic reviews have reported heterogeneous findings and methodological limitations, and none incorporated prebiotic or synbiotic interventions (19, 20). Moreover, their methodological quality assessed using AMSTAR-2 was low (Supplementary material 1). These limitations justify the need for an updated systematic review to evaluate current evidence and identify research gaps.
This systematic review aims to evaluate the available evidence and identify research gaps regarding the effect of prebiotics, probiotics, and synbiotics as dietary interventions targeting gut microbiota to prevent mental health disorders during pregnancy and postpartum in women without diagnosed mental health disorders.
Methods
2
This systematic review was carried out in accordance to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (22). A protocol for this review was registered in the International prospective register of systematic reviews (PROSPERO ID: CRD42024576678).
Search strategy and selection criteria
2.1
A comprehensive bibliographic search was conducted (Supplementary material 2) across the electronic databases, MEDLINE, EMBASE, CINAHL, The Cochrane Library (CENTRAL), Scopus, Proquest Dissertations and Theses, and Web of Science Core Collection, from inception to March 2025. The search strategy, developed by a health sciences librarian (CHC), focused exclusively on randomized controlled trials (RCTs), excluding animal studies. No restrictions on language or publication date were applied.
Only randomized controlled trials (RCTs) evaluating prebiotic, probiotic, and/or synbiotic supplementation (PPS) conducted in pregnant women without a diagnosis of mental health disorder were included. The absence of a mental health disorder was defined according to the inclusion criteria of each individual trial and was generally based on self-report and/or the absence of a prior clinical diagnosis, rather than on structured psychiatric interviews. The presence of subthreshold depressive or anxiety symptoms was not an exclusion criterion in most studies, which is consistent with a primary prevention framework but limits conclusions regarding clinically diagnosed disorders.
The intervention of interest was PPS, alone or in combination compared to treatment as usual, standard advice or a placebo control group. The primary outcomes reviewed were measures of maternal mental health (well-being, anxiety, depression, stress, mood, nervous, obsession, etc. For more terms used, see Supplementary material 2) during pregnancy and the postpartum period. As secondary outcomes, health problems and changes in the gut microbiota of the mother or offspring were reviewed. Review articles, editorials, letters, case series, case reports, quasi-experimental studies and observational studies were excluded from the review.
After duplicates were removed, the selection process was conducted in two phases: first, titles and abstracts were screened for relevance, followed by a review of the full text to ensure that the inclusion criteria were met. Two independent reviewers (LMMR and SMP) carried out the screening process with the help of the Rayyan application (23). Disagreements between reviewers were resolved by discussion or, when necessary, by consulting a third reviewer to reach consensus (NCI). Reasons for exclusion were further documented (Supplementary material 3).
Data extraction
2.2
Data extraction was performed by two independent reviewers (LMMR and SMP) using a standardized form. The following information was collected for each included study: study characteristics (author, year of publication, setting, sample size), participant characteristics (age, gestational stage), intervention details (type, dose, duration of probiotics, prebiotics or synbiotics intervention in experimental and control group), primary outcome (type of mental disorder and measurement tool), secondary outcomes (type of health disorder/changes in maternal or newborn gut microbiota and measurement tool). Reported side effects or adverse reactions were also recorded. All reported mean differences (MDs) correspond to individual study estimates, as reported in the original publications. Results were synthesized using a structured narrative approach, with findings presented at the individual study level.
Discrepancies between reviewers (LMMR and SMP) were resolved by discussion. When consensus was not reached, a third reviewer (NCI) was consulted to ensure accurate and comprehensive data extraction.
The quality of the included studies was assessed using the Risk of Bias 2 (ROB2) tool (24). This tool assesses the risk of bias in RCTs in five domains: Randomization process, Deviations from intended interventions, Missing outcome data, Outcome measurement, and Selection of reported outcome. Each domain was classified as “low risk,” “some concern,” or “high risk” based on the criteria described in the ROB2 tool. The overall risk of bias for each study was determined by considering the ratings across all domains. This quality assessment was performed by two independent reviewers (LMMR and SMP), and disagreements between reviewers were resolved by discussion or, when necessary, by consulting a third reviewer to reach consensus (NCI).
Evidence synthesis
2.3
We tabulated the findings and constructed graphs as appropriate. Due to small number of studies, statistical synthesis was not performed.
Results
3
A total of 1,401 records were identified through database searches. After screening titles and abstracts, 11 records were assessed for eligibility. Of these, 6 were excluded based on predefined inclusion criteria, remaining 5 full-text articles for further evaluation. Ultimately, after removal of one study because it included women diagnosed with a mental health disorder, 4 studies met all inclusion criteria and were included in this systematic review (Figure 1).
PRISMA 2020 flow diagram for the systematic reviews including searches of databases, registers, and other sources.
Characteristics and quality of included studies
4
The included studies were carried out in New Zealand (25), Finland (26), Iran (27), and Italy (28). The publication dates ranged from 2016 to 2023. The total number of participants varied from 60 (27) to 439 (26), with a cumulative total of 1,342 women included in this review. The gestational age at the start of the trials did not exceed 28 weeks, and the participants’ ages ranged from 16 (25) to 50 years (28) (Table 1). The four RCTs included probiotics in the interventions. The probiotic strains used were Lactobacillus rhamnosus HN001 (25, 26), Bifidobacterium animalis ssp. lactis 420 (26), Limosilactobacillus reuteri PBS072 (28), Bifidobacterium breve BB077 (28), Lactobacillus acidophilus La-5 and Bifidobacterium lactic Bb-12 (27). The probiotic daily dose varied from 4 × 10^9^ CFU (28) to 4.8 × 10^10^ CFU (27), administered in capsules with the exception of one study, which used yogurt as probiotic vehicle (27). Intervention duration ranged from 4 weeks (27) to 48 weeks (25), and occurred during pregnancy only (27), both pregnancy and postpartum (25, 26) or only postpartum (28). From the four studies, three investigated mental health as primary outcome (25, 26, 28). The mean intervention follow-up rated from 12 to 24 months (Table 2).
Of the included studies, one was classified as a high risk (Figure 2), the remaining 3 studies were classified as moderate. Among the ROB2 domains (Figure 3), the most frequent critical weakness identified was the risk of bias in the selection of the reported outcome.
Risk of bias assessment of the included studies across individual domains and overall judgment.
Summary of overall risk of bias across domains for the included studies.
Primary outcomes
4.1
Depressive (n = 3) and anxiety (n = 2) symptoms were the most frequently assessed outcomes, measured using tools such as the Edinburgh Postnatal Depression Scale (EPDS) (25, 26, 28), the State Trait Anxiety Inventory-6 (STAI-6) (25) and the Symptom Checklist-90 (SCL-90) (26). In addition, one study measured quality of life using the quality-of-life questionnaire (SF-36) (27), which assesses aspects such as emotional problems, emotional well-being and related domains (Table 2).
Regarding depressive or anxiety symptoms during pregnancy, one study (26) found not statistically significant differences between intervention Lactobacillus rhamnosus HN001 plus Bifidobacterium animalis ssp. lactis 420 and control groups, although minor variations were observed at 12 months of follow-up in EPDS test scores between the intervention groups containing fish oil and placebo versus probiotics and placebo (MD = −1.12, p = 0.039). In contrast, another study (25) reported significant reductions in depression mean differences (MD) scores in the intervention group (Lactobacillus rhamnosus HN001) compared to the control [MD = −1.2 95% CI (−2.3, −0.1)] and anxiety mean scores [MD = −1.0 95% CI (−1.9, −0.2)]. Regarding postpartum depression, one study (28) reported that at day 45, the intervention group (Limosilactobacillus reuteri PBS072 plus Bifidobacterium breve BB077) showed a significantly lower mean score (9.0 ± 4.8) compared to the control group (12.1 ± 5.9) (p < 0.001) and at day 90 (7.0 ± 3.3 vs. 10.8 ± 6.2, p < 0.001) (Table 2). Another study (27) showed not significant differences between intervention (Lactobacillus acidophilus La-5 plus Bifidobacterium animalis subsp. lactis Bb-12) and control groups regarding quality of life.
Secondary outcomes
4.2
From the 4 studies included in the review, only one (28) reported information about the secondary outcomes. Using the Breastfeeding Self-Efficacy Scale—Short Form (BSES-SF), they found that 45 and 90 days after the beginning of the intervention, breastfeeding quality and the baby’s crying/fussing significantly improved in the probiotic group. At 45 days postpartum, 81% of mothers in the intervention group reported improvement in crying/fussing events compared with 42% in the control group, while at 90 days postpartum the corresponding figures were 78 and 43%, respectively. In addition, the mean daily number of crying/fussing events was significantly lower in the probiotic group compared with the control group at both time points (p < 0.001).
Discussion
5
The evidence obtained in this study on the effect of prebiotics, probiotics, and synbiotics for preventing maternal mental health disorders is limited and heterogeneous. Only four RCTs met inclusion criteria, all focused on probiotics, highlighting a major research gap regarding prebiotics and synbiotics (19, 20). Importantly, by explicitly including prebiotics and synbiotics in the research question and search strategy, this review provides an updated assessment of the current evidence base and clearly demonstrates the absence of eligible RCTs for these interventions in perinatal mental health. While two trials reported improvements in depressive and anxiety symptoms (25, 28) others found no significant effects on mental health outcomes or quality of life (26, 27), in line with previous systematic reviews showing mixed results (19–21).
Importantly, the available evidence pertains to symptom-based outcomes rather than clinically diagnosed mental health disorders. Most studies allowed the presence of subthreshold symptoms and relied on self-reported measures rather than structured diagnostic interviews. Therefore, findings should be interpreted within a primary prevention framework focused on symptom reduction, rather than prevention of diagnosed mental health disorders.
Although secondary outcomes were reported in only one included trial, breastfeeding-related outcomes and infant crying/fussing are indirectly relevant to maternal mental health in the postpartum period. Postpartum depressive symptomatology has been consistently associated with less favorable infant-feeding outcomes, including breastfeeding difficulties and lower breastfeeding self-efficacy (29, 30). Moreover, evidence from systematic reviews and cohort studies indicates that excessive or inconsolable infant crying is associated with maternal depressive and anxiety symptoms, suggesting bidirectional and stress-mediated pathways (31–33). Nevertheless, because these secondary outcomes were reported in only one included trial, they should be interpreted cautiously and cannot be generalized.
Methodological heterogeneity likely explains these discrepancies, including wide variation in participant age (25, 28), intervention duration (27), probiotic strains and doses (34), and outcome measures. Some strains, such as Lactobacillus rhamnosus HN001 showed promising effects (25), but findings remain inconclusive due to limitations such as retrospective data collection and high dropout rates (26, 35). Other strains demonstrated benefits in specific populations or contexts (28, 36–40), suggesting context- and strain-specific effects.
Additional limitations include lack of standardized dosing (41), inadequate control of antibiotic use by participants in RCTs (25, 26, 28), reliance on self-reported adherence (42, 43), high microbiota variability (44, 45), heterogeneity in psychological instruments with varying validity (25, 26, 46–52) and absence of structured clinical interviews (53). Together, these issues underscore the need for well-designed, standardized RCTs to clarify the role of probiotics in maternal mental health.
Strengths and limitations
5.1
This systematic review followed PRISMA guidelines and was prospectively registered in PROSPERO, ensuring transparency and reproducibility. The search strategy was comprehensive, developed with a health sciences librarian, and applied across multiple databases without language or date restrictions. Study selection, data extraction, and risk of bias assessment (ROB2) were performed independently by two reviewers, with disagreements resolved by a third reviewer.
Limitations mainly reflect the scarcity and heterogeneity of the available evidence. Only four RCTs were identified, all evaluating probiotics, with no eligible trials assessing prebiotics or synbiotics. Differences in probiotic strains, doses, intervention duration, and outcome measures limited comparability across studies and precluded meta-analysis. Finally, the limited geographic representation may reduce generalizability to other populations and settings.
Conclusion
6
Current evidence on the effect of probiotics for preventing mental health disorders during pregnancy and postpartum is limited and heterogeneous, with no RCTs evaluating prebiotics or synbiotics. Although some studies report symptoms reductions, heterogeneity in strains, doses, intervention duration, and measurement tools limit conclusions. Well-designed and adequately powered RCTs are needed where maternal depressive and anxiety symptoms are primary outcomes, using standardized and strain-specific interventions, appropriate doses and durations, and harmonized assessment tools. Future trials should also explicitly evaluate prebiotics and synbiotics, as these remain major evidence gaps in perinatal mental health research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Guide for integration of perinatal mental health in maternal and child health services. Geneva: World Health Organization (2022).
- 2Rogers AM Youssef GJ Teague S Sunderland M Le Bas G Macdonald JA . Association of maternal and paternal perinatal depression and anxiety with infant development: a longitudinal study. J Affect Disord. (2023) 338:278–88. doi: 10.1016/j.jad.2023.06.020, 37302506 · doi ↗ · pubmed ↗
- 3Costa B Vale N. Advances in psychotropic treatment for pregnant women: efficacy, adverse outcomes, and therapeutic monitoring. J Clin Med. (2024) 13:398. doi: 10.3390/jcm 13154398, 39124665 PMC 11312735 · doi ↗ · pubmed ↗
- 4Hidayati NO Nuraeni A Nurhidayah I Rhamelani P Nurjanah LS Yani P . Effect of non-Pharmachological therapies for pregnant women with mental disorder: a narrative review: effect of non-Pharmachological therapies for pregnant women with mental disorder: a narrative review. J Surya Med. (2024) 10:376–83. doi: 10.33084/jsm.v 10i 1.7239 · doi ↗
- 5Song J Zhou B Kan J Liu G Zhang S Si L . Gut microbiota: linking nutrition and perinatal depression. Front Cell Infect Microbiol. (2022) 12:932309. doi: 10.3389/fcimb.2022.932309, 36093196 PMC 9459161 · doi ↗ · pubmed ↗
- 6Valles-Colomer M Falony G Darzi Y Tigchelaar EF Wang J Tito RY . The neuroactive potential of the human gut microbiota in quality of life and depression. Nat Microbiol. (2019) 4:623–32. doi: 10.1038/s 41564-018-0337-x, 30718848 · doi ↗ · pubmed ↗
- 7Sanada K Nakajima S Kurokawa S Barceló-Soler A Ikuse D Hirata A . Gut microbiota and major depressive disorder: a systematic review and meta-analysis. J Affect Disord. (2020) 266:1–13. doi: 10.1016/j.jad.2020.01.102, 32056863 · doi ↗ · pubmed ↗
- 8Simpson CA Diaz-Arteche C Eliby D Schwartz OS Simmons JG Cowan CS. The gut microbiota in anxiety and depression–a systematic review. Clin Psychol Rev. (2021) 83:101943. doi: 10.1016/j.cpr.2020.10194333271426 · doi ↗ · pubmed ↗