Extrapelvic Urinary Extravasation Caused by Retroperitoneal Metastasis of Pulmonary Squamous Cell Carcinoma: A Case Report
Manato Taguchi, Takumi Kiwamoto, Shun Kagaya, Toshihiro Shiozawa, Nobuyuki Hizawa

TL;DR
A rare case of urinary leakage caused by cancer spread in a lung cancer patient is reported, highlighting the importance of early diagnosis for better treatment outcomes.
Contribution
This is the first reported case of extrapelvic urinary extravasation caused by retroperitoneal metastasis of pulmonary squamous cell carcinoma.
Findings
Extrapelvic urinary extravasation was diagnosed due to retroperitoneal metastasis in a patient with stage IVB lung cancer.
Placement of a double-J ureteral stent resolved the patient's pain and allowed continuation of chemotherapy.
This rare condition was not previously documented in the literature.
Abstract
A 52-year-old man with pulmonary squamous cell carcinoma, clinically staged as cTxN3M1c (stage IVB), received four cycles of first-line chemotherapy with cisplatin plus TS-1 followed by seven cycles of second-line nivolumab. Subsequent imaging revealed progressive enlargement of cervical lymph nodes, left adrenal metastasis, and retroperitoneal metastases. Over several days, he developed left flank and back pain and presented to the emergency department. An emergent contrast-enhanced abdominal computed tomography (CT) demonstrated contrast extravasation from the upper left ureter, left ureteral obstruction caused by retroperitoneal metastasis, and mild hydronephrosis. He was diagnosed with extrapelvic urinary extravasation and underwent placement of a polymeric double-J ureteral stent. His pain resolved promptly thereafter, allowing initiation of third-line chemotherapy. Extrapelvic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
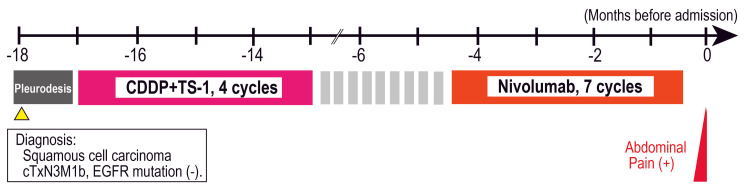 Figure 1
Figure 1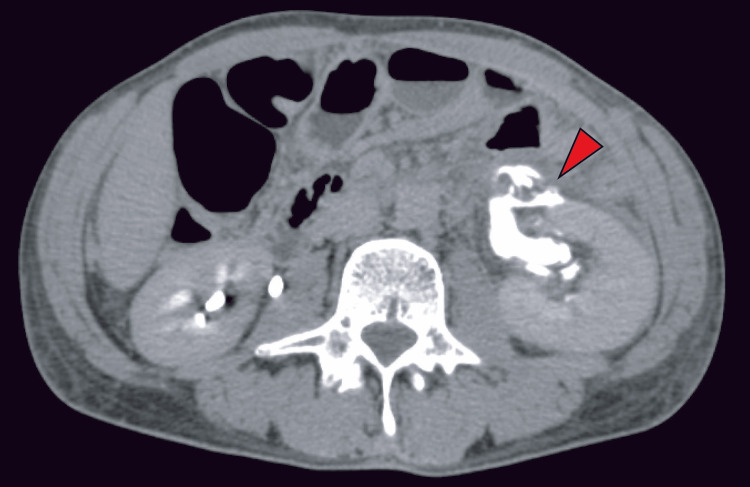 Figure 2
Figure 2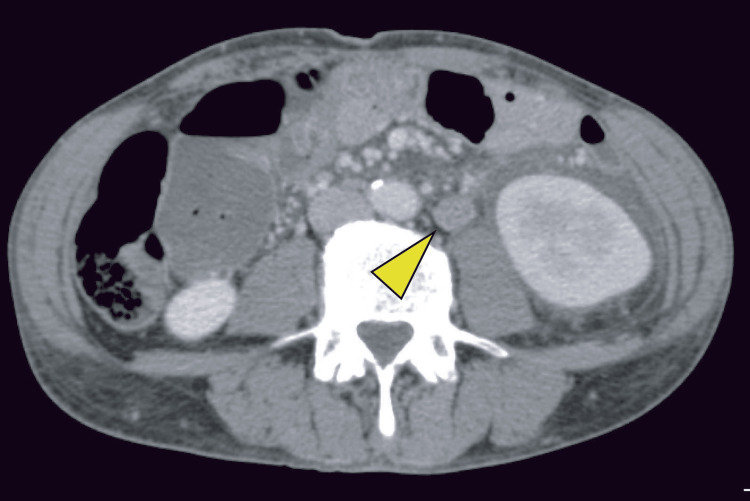 Figure 3
Figure 3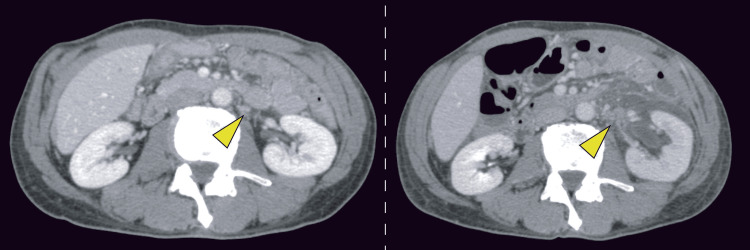 Figure 4
Figure 4 Figure 5
Figure 5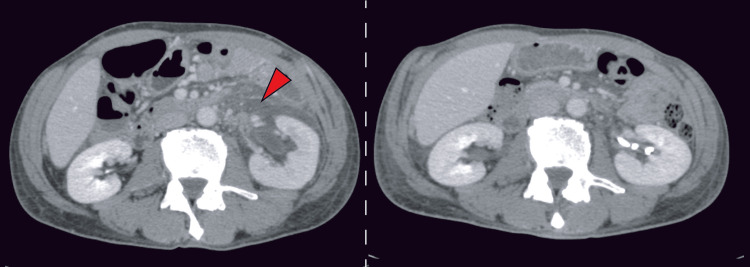 Figure 6
Figure 6| Parameter (Unit) | Value | Reference range |
| Blood test | ||
| WBC (/μL) | 8400 | 4500-9000 |
| Neu (%) | 89.9 | 49-62 |
| Lym (%) | 9.7 | 25-45 |
| Eos (%) | 0.2 | 1-5 |
| Baso (%) | 0 | 0-1 |
| RBC (×10⁴/µL) | 430 | 427-570 |
| Hb (g/dL) | 13.3 | 14-18 |
| Hct (%) | 38.7 | 40-52 |
| Plt (×10⁴/µL) | 25.1 | 15-35 |
| Alb (g/dL) | 3.5 | 3.8-5.3 |
| AST (U/L) | 30 | 8-38 |
| ALT (U/L) | 13 | 4-44 |
| LDH (U/L) | 206 | 106-211 |
| ALP (U/L) | 273 | 104-338 |
| γ-GTP (IU/L) | 26 | 12-63 |
| T-Bil (mg/dL) | 0.6 | 0.3-1.2 |
| Na (mEq/L) | 138 | 135-147 |
| Cl (mEq/L) | 102 | 98-108 |
| K (mEq/L) | 4.7 | 3.6-5 |
| BUN (mg/dL) | 10.2 | 8-20 |
| Cre (mg/dL) | 0.86 | 0.61-1.04 |
| eGFR (mL/min) | 73.6 | 60-100 |
| CRP (mg/dL) | 2.26 | 0-0.2 |
| Ca (mg/dL) | 8.9 | 8.6-10.1 |
| Parameter (Unit) | Value | Reference Range |
| Blood test | ||
| WBC (/μL) | 10200 | 4500-9000 |
| Neu (%) | 90.1 | 49-62 |
| Lym (%) | 9.4 | 25-45 |
| Eos (%) | 0.4 | 1-5 |
| Baso (%) | 0.1 | 0-1 |
| RBC (×10⁴/µL) | 421 | 427-570 |
| Hb (g/dL) | 12.8 | 14-18 |
| Hct (%) | 38 | 40-52 |
| Plt (×10⁴/µL) | 25.6 | 15-35 |
| Alb (g/dL) | 3.1 | 3.8-5.3 |
| AST (U/L) | 40 | 8-38 |
| ALT (U/L) | 12 | 4-44 |
| LDH (U/L) | 322 | 106-211 |
| ALP (U/L) | 253 | 104-338 |
| γ-GTP (IU/L) | 24 | 12-63 |
| T-Bil (mg/dL) | 0.9 | 0.3-1.2 |
| Na (mEq/L) | 136 | 135-147 |
| Cl (mEq/L) | 100 | 98-108 |
| K (mEq/L) | 4,3 | 3.6-5 |
| BUN (mg/dL) | 10 | 8-20 |
| Cre (mg/dL) | 0.96 | 0.61-1.04 |
| eGFR (mL/min) | 65.3 | 60-100 |
| CRP (mg/dL) | 7.88 | 0-0.2 |
| Ca (mg/dL) | 8.5 | 8.6-10.1 |
| Urinalysis | ||
| pH | 6.5 | 4.6-7.5 |
| Specific gravity | 1.009 | 1.015-1.025 |
| Protein | negative | negative |
| Glucose | negative | negative |
| Occult blood | negative | negative |
| Nitrite | negative | negative |
| Urine WBC (qualitative) | negative | negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUreteral procedures and complications · Chemotherapy-related skin toxicity · Methemoglobinemia and Tumor Lysis Syndrome
Introduction
Urinary extravasation is an uncommon condition characterized by the radiological demonstration of urine or contrast material outside the renal collecting system. In most cases, it is associated with trauma, iatrogenic manipulation, or obstructive pathology [1,2]. When extravasation occurs in the absence of recent instrumentation, trauma, prior surgery, destructive renal disease, or external compression, it is referred to as spontaneous urinary extravasation [1-3]. Spontaneous urinary extravasation is thought to occur when impaired urinary flow elevates intrapelvic pressure, producing microscopic tears in the urothelium at the fornix, through which urine seeps into the peripelvic or perirenal fat. The fornix is the most common site of rupture, followed by the upper ureter when pressure exceeds a critical level reported from 20 to 75 mmHg [4]. Urinary leakage may subsequently lead to the formation of a urinoma [5]. On imaging, the delayed phase of contrast-enhanced computed tomography (CT) scan is particularly valuable, as the distribution of contrast leakage often allows localization of the rupture site [1]. Most reported cases involve spontaneous rupture associated with ureteral calculi; in contrast, cases caused by malignant ureteral obstruction are relatively uncommon [6].
Here, we describe an extremely rare case of urinary extravasation caused by ureteral obstruction from retroperitoneal dissemination of pulmonary squamous cell carcinoma during systemic chemotherapy. Ureteral obstruction caused by lung cancer metastasis is itself uncommon [7], and to our knowledge, no previous reports have described urinary extravasation secondary to retroperitoneal metastasis of pulmonary squamous cell carcinoma. With the increasing use of immunotherapy and molecular targeted agents, survival among patients with lung cancer has improved, and clinicians may encounter this condition more frequently. It should therefore be considered in the differential diagnosis of abdominal or flank pain in patients with advanced lung cancer.
Case presentation
A 52-year-old man presented to the emergency department with progressively worsening low back pain. He had been undergoing treatment for pulmonary squamous cell carcinoma for 18 months (Figure 1).
Clinical courseClinical course diagram showing the timeline from the initial presentation 18 months prior to admission through diagnosis and the administration of chemotherapy up to second-line treatment, culminating in the onset of abdominal pain.EGFR - epidermal growth factor receptor
At age 50, he had been diagnosed with pulmonary squamous cell carcinoma, clinically staged as cTxN3M1c stage IVB (metastases to the right iliac bone, left perigastric lymph nodes, and malignant pleural effusion), with no epidermal growth factor receptor (EGFR) gene mutation detected by PCR-based assay. He received four cycles of first-line chemotherapy with cisplatin plus TS-1, achieving stable disease as the best response. However, the disease recurred eight months after completion of treatment, and seven cycles of nivolumab were administered as second-line therapy. The best response to second-line treatment was also stable disease. An evaluation CT performed one week prior to presentation revealed enlargement of para-aortic lymph nodes in the suprarenal region, left adrenal metastasis, newly identified retroperitoneal metastases, and vertebral bone metastases; therefore, initiation of third-line therapy was being planned. At the time of imaging, no evident hydronephrosis was observed. In addition, worsening cancer-related pain associated with malignant pleuritis had required initiation of regular oral oxycodone one month prior, in addition to etodolac.
Several days before admission, his left low back pain worsened despite increasing the regular dose of oxycodone and using additional rescue doses, eventually resulting in pain severe enough to impair his ability to stand. This prompted an emergency department visit. At presentation, he was alert, with a low-grade fever (37.4°C), while his blood pressure, heart rate, and oxygenation were stable. The Eastern Cooperative Oncology Group (ECOG) performance status was 1. His abdomen was flat and soft, but he had severe spontaneous pain in the left flank, making even light palpation intolerable. Laboratory evaluation showed mild inflammatory changes (white blood cells 8400/μL with 82.5% segmented neutrophils, C-reactive protein 2.26 mg/dL), while renal function remained preserved (blood urea nitrogen 10.2 mg/dL, creatinine 0.86 mg/dL, Table 1).
Chest radiography showed right-dominant pleural effusion due to malignant pleuritis, without significant interval worsening compared to prior CT, and no free air was detected. An upright abdominal radiograph revealed no abnormalities. Based on these findings, inadequate pain control due to progression of the primary disease was suspected, and he was admitted for analgesia.
On hospital day two, however, he developed a fever of 39.3°C and worsening left back pain. Although chills or rigors were absent, left costovertebral angle tenderness and rebound tenderness were present. Laboratory testing showed further inflammatory elevation (white blood cells 10,200/μL with 80.2% segmented neutrophils, C-reactive protein 7.88 mg/dL, Table 2), although urinalysis was normal. Blood and urine cultures obtained at that time were negative, and urine cytology revealed no malignant cells.
Contrast-enhanced CT demonstrated urinary extravasation from the left upper ureter in the delayed phase (Figure 2). In addition, a soft-tissue density suggestive of tumor progression was observed adjacent to the left ureter (Figure 3).
Delayed-phase contrast-enhanced abdominal CT on hospital day twoRed arrows indicate the site of contrast medium extravasation. Delayed-phase contrast-enhanced CT demonstrated extravasation of contrast material from the left renal pelvis into the left perirenal space.
Contrast-enhanced abdominal CT on hospital day twoYellow arrows indicate newly developed retroperitoneal metastasis adjacent to the left ureter.
A CT scan obtained one week prior to admission had revealed left adrenal metastasis and retroperitoneal metastatic lesions (Figure 4); however, these lesions had progressed, and hydronephrosis had subsequently developed.
Contrast-enhanced abdominal CTCT obtained one week before admission (left panel) and on hospital day two (right panel). Yellow arrows indicate retroperitoneal metastatic lesions.
Based on these findings, the patient was diagnosed with urinary extravasation secondary to ureteral obstruction caused by encasement of the ureter by retroperitoneal tumor invasion resulting from progression of lung squamous cell carcinoma.
Following diagnosis, the patient was treated with antibiotics and underwent placement of a polymeric double-J ureteral stent (Figure 5), resulting in substantial symptom improvement. Combination chemotherapy with cisplatin and vinorelbine as third-line therapy was initiated on hospital day 19.
Plain abdominal radiograph obtained after placement of a double-J ureteral stent
A follow-up CT scan performed one month after stent placement showed improvement in both the perirenal fluid collection and hydronephrosis, (Figure 6), allowing discharge. After discharge, the ureteral stent was left in place, and third-line chemotherapy was continued. Thereafter, no deterioration in urinary outflow or renal function was observed, and stent exchanges performed every three months were uneventful; therefore, a polymeric double-J ureteral stent was continuously used. Following completion of third-line therapy, the patient was managed with observation alone for three months, after which disease recurrence was noted. Fourth-line therapy with docetaxel plus ramucirumab, fifth-line therapy with irinotecan monotherapy, and sixth-line therapy with amrubicin monotherapy were administered but were ineffective. He died of disease progression one year after discharge.
Contrast-enhanced abdominal CT after treatmentContrast-enhanced abdominal CT on hospital day two (left panel) and one month after ureteral stent placement (right panel). The perirenal fluid collection around the left kidney (red arrow) and hydronephrosis observed on hospital day two showed marked improvement after stent placement.
Discussion
In the present case, retroperitoneal dissemination of lung squamous cell carcinoma was considered to have caused ureteral compression, leading to ureteral obstruction. In a report by Gershman et al. in 2011, urolithiasis was identified as the most frequent cause of renal forniceal rupture, accounting for approximately 74.1% of cases, whereas malignant extrinsic ureteric compression was relatively uncommon, comprising only 8.3% [6]. Furthermore, Artiles et al. reported that the most frequent causes of malignant ureteral obstruction were prostate (17.6%), bladder (16.5%), and rectal cancer (11.7%), while lung cancer was rare, accounting for only 1.6% of cases [7]. Only a single case of retroperitoneal metastasis from pulmonary squamous cell carcinoma has been reported [8]. To the best of our knowledge, no cases of urinary extravasation caused by lung squamous cell carcinoma have been reported. Araya et al. recently reported three cases of malignant ureteral obstruction caused by retroperitoneal metastases from lung adenocarcinoma [9]. In their series, two patients harbored EGFR mutations, suggesting that prolonged survival achieved with targeted therapies may allow lung cancer to metastasize to uncommon sites. Although the present case was squamous cell carcinoma, disease control was maintained for a relatively long period for stage IV squamous cell carcinoma, indicating that similar conditions predisposing to unusual metastatic patterns may have been present.
Imaging studies are useful for the diagnosis of urinary extravasation. Contrast-enhanced CT can demonstrate perirenal fluid collection and ureteral dilatation. In the delayed phase of contrast-enhanced CT, the site of rupture can often be identified based on the extent of contrast leakage; however, when urinary leakage is accompanied by an inflammatory response, patients may present with fever and pain, making differentiation from acute pyelonephritis or renal colic difficult and potentially delaying diagnosis [1]. In the present case, CT revealed perirenal fluid collection around the left kidney, leading to the diagnosis of urinary extravasation.
The management of urinary extravasation primarily consists of treatment of the underlying cause and urinary tract drainage [10]. Because urinary tract obstruction can lead to irreversible renal damage and may preclude the administration of systemic therapy; therefore, prompt decompression by ureteral stent placement or percutaneous nephrostomy is essential to preserve renal function and enable continuation of cancer treatment [11-13]. In the present case, worsening retroperitoneal metastases from lung cancer during chemotherapy led to the development of urinary extravasation, and urinary drainage was therefore achieved by placement of a ureteral polymeric double-J ureteral stent. As a result, the perirenal fluid collection decreased, symptoms improved, and the patient was able to proceed to third-line therapy. The prognosis of lung squamous cell carcinoma has improved with the widespread use of immunotherapy and the expansion of treatment options [14]. This improvement in survival should be considered a potential factor increasing the incidence of rare complications at distant metastatic sites, such as those with limited responsiveness to chemotherapy, as observed in the present case.
Conclusions
We reported a case of extrapelvic urinary extravasation caused by retroperitoneal metastasis of pulmonary squamous cell carcinoma. To our knowledge, no previous cases of extrapelvic urinary extravasation associated with pulmonary squamous cell carcinoma have been reported. With improvements in the long-term prognosis of pulmonary squamous cell carcinoma, clinicians should consider extrapelvic urinary extravasation secondary to retroperitoneal metastasis as a potential cause when patients with an expected long-term survival present with acute abdominal symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spontaneous urinary extravasation: an overlooked cause of acute abdomen in ED Am J Emerg Med Lien WC Chen WJ Wang HP Liu KL Hsu CC 3473492420061663570910.1016/j.ajem.2005.09.016 · doi ↗ · pubmed ↗
- 2Spontaneous extravasation of contrast medium during intravenous urography. Report of fourteen cases and a review of the literature Clin Radiol Cooke GM Bartucz JP 8793251974442443310.1016/s 0009-9260(74)80105-4 · doi ↗ · pubmed ↗
- 3Spontaneous renal extravasation during intravenous urography Am J Roentgenol Radium Ther Nucl Med Schwartz A Caine M Hermann G Bittermann W 274098196610.2214/ajr.98.1.275913699 · doi ↗ · pubmed ↗
- 4Spontaneous ureteral rupture diagnosis and treatment Case Rep Radiol Pampana E Altobelli S Morini M Ricci A D'Onofrio S Simonetti G 851859201320132445538110.1155/2013/851859 PMC 3884862 · doi ↗ · pubmed ↗
- 5Renal cysts and urinomas Semin Intervent Radiol Lee J Darcy M 3803912820112320463610.1055/s-0031-1296080 PMC 3312170 · doi ↗ · pubmed ↗
- 6Causes of renal forniceal rupture BJU Int Gershman B Kulkarni N Sahani DV Eisner BH 1909191110820112173669010.1111/j.1464-410X.2011.10164.x · doi ↗ · pubmed ↗
- 7The challenging management of malignant ureteral obstruction: analysis of a series of 188 cases Curr Urol Artiles Medina A Laso García I González Tello F 34421820243850515610.1097/CU 9.0000000000000183 PMC 10946639 · doi ↗ · pubmed ↗
- 8Synchronous thyroid and colon metastases from epidermoid carcinoma of the lung: case report Sao Paulo Med J Azevedo CR Cezana L Moraes ES Begnami MD Paiva Júnior TF Dettino AL Fanelli MF 37137412820102130816210.1590/S 1516-31802010000600011 PMC 10948072 · doi ↗ · pubmed ↗