Improving the diagnosis of central nervous system infections: experience with the off-label use of FA-BCID2
Giulia Menchinelli, Margherita Cacaci, Damiano Squitieri, Giulia De Angelis, Maurizio Sanguinetti, Brunella Posteraro

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
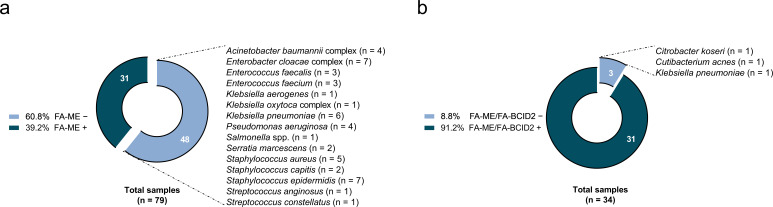 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Peripheral Neuropathies and Disorders · Infectious Encephalopathies and Encephalitis
LETTER
Multiplex PCR panels for central nervous system (CNS) infections are widely used but have well-recognized limitations: the FilmArray Meningitis/Encephalitis (FA-ME) panel (bioMérieux, Marcy l’Étoile, France) is strong for “ruling in” yet limited for “ruling out,” and negative results do not exclude infection (1–3).
We report our experience with the off-label use of the FilmArray Blood Culture Identification 2 (FA-BCID2) panel (bioMérieux) on cerebrospinal fluid (CSF), focusing on bacterial pathogens relevant to hospital-acquired (HA) CNS infections and late-onset neonatal meningitis (e.g., Klebsiella pneumoniae, Enterobacter cloacae complex, Acinetobacter baumannii complex, and coagulase-negative staphylococci) in contrast to FA-ME, which primarily targets community-acquired (CA) bacteria (4). Previous small studies on FA-BCID/BCID2 in CSF have reported promising performance (5–7).
This study was performed at a large tertiary-care university hospital with neurosurgical services and analyzed two periods, that is, before and after implementation of FA-BCID2. We included all culture-positive bacterial meningitis cases for which at least one FilmArray assay (FA-ME or FA-BCID2) was performed: 79 cases in the pre-implementation period and 34 in the post-implementation period. These cases represented 11.2 (79/703) and 9.5% (34/358) of all CSF samples for which a FilmArray assay was performed for suspected meningitis in the respective periods. In the post-implementation period, infectious disease specialists requested molecular testing for suspected meningitis by phone and indicated whether the case was adult CA or HA or neonatal early- versus late-onset using standard clinical and epidemiological criteria consistent with the corresponding published definitions (8, 9). Based on this classification, CSF samples were tested with FA-ME for CA/viral differential diagnoses and with FA-BCID2 for suspected HA infections. FA-BCID2 was used off-label directly on CSF (no enrichment) after internal verification using contrived/spiked CSF and known-positive samples.
In the pre-implementation period (May 2018–April 2023), FA-ME was the only molecular assay used; there were 79 culture-confirmed bacterial meningitis cases (HA 41, CA 28, neonatal 10), and FA-ME detected the pathogen in 31/79 (39.2%). The 48 FA-ME-negative results represented missed opportunities for early targeted antimicrobial therapy. In the post-implementation period (May 2023–June 2025), a combined algorithm with FA-ME and FA-BCID2 was adopted; culture-positive cases were 34 (HA 16, CA 13, late-onset neonatal 5), with an overall molecular detection of 31/34 (91.2%). Excluding the 13 CA cases (all correctly detected by FA-ME), 14/16 (87.5%) HA and 4/5 (80.0%) neonatal late-onset cases were correctly detected by FA-BCID2. Notably, two neurosurgical patients—one with K. pneumoniae, the other with Cutibacterium acnes meningitis—tested negative with FA-BCID2 and were confirmed only by 16S rRNA PCR/sequencing, while Citrobacter koseri meningitis in a neonate was missed as an off-panel pathogen. The corresponding pathogen distributions and detection rates by period and category are shown in Fig. 1.
(a) Pathogen distribution in CSF culture-positive cases detected by the FilmArray Meningitis/Encephalitis (FA-ME) panel (May 2018–April 2023). (b) Pathogen distribution after implementation of the combined FA-ME + FilmArray Blood Culture Identification 2 (FA-BCID2) panel algorithm (May 2023–June 2025). “+” and “–” indicate positive and negative molecular assay results, respectively.
While the molecular detection rate improved markedly, the clinical impact of this strategy (e.g., faster initiation of targeted therapy or improved patient outcomes) was not assessed in this study.
In conclusion, our data suggest that the combined use of FA-ME and FA-BCID2 assays may improve the molecular diagnosis of HA bacterial meningitis and late-onset neonatal meningitis. However, false negatives and off-panel organisms underscore that these panels should complement, rather than replace, conventional culture and highlight the need for molecular assays specifically tailored to nosocomial CNS infections. Revisiting diagnostics in this field means not only introducing new assays but also rethinking the scope and adaptation of existing ones.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Olie SE, Andersen CØ, van de Beek D, Brouwer MC. 2024. Molecular diagnostics in cerebrospinal fluid for the diagnosis of central nervous system infections. Clin Microbiol Rev 37:e 0002124. doi:10.1128/cmr.00021-2439404267 PMC 11629637 · doi ↗ · pubmed ↗
- 2Trujillo-Gómez J, Tsokani S, Arango-Ferreira C, Atehortúa-Muñoz S, Jimenez-Villegas MJ, Serrano-Tabares C, Veroniki AA, Florez ID. 2022. Biofire Film Array Meningitis/Encephalitis panel for the aetiological diagnosis of central nervous system infections: a systematic review and diagnostic test accuracy meta-analysis. E Clinical Medicine 44:101275. doi:10.1016/j.eclinm.2022.10127535198914 PMC 8851290 · doi ↗ · pubmed ↗
- 3Vetter P, Schibler M, Herrmann JL, Boutolleau D. 2020. Diagnostic challenges of central nervous system infection: extensive multiplex panels versus stepwise guided approach. Clin Microbiol Infect 26:706–712. doi:10.1016/j.cmi.2019.12.01331899336 · doi ↗ · pubmed ↗
- 4Smit LFE, Wessels E, Boers SA, Claas ECJ. 2025. Revisiting diagnostics: rapid diagnosis of neurological infections. Clin Microbiol Infect 31:899–900. doi:10.1016/j.cmi.2025.01.02039863070 · doi ↗ · pubmed ↗
- 5López-Amor L, García-Prieto E, Fernández-Suárez J, Escudero D, Vázquez F, Fernández J. 2020. Evaluation of a commercial multiplex PCR for diagnosis of central nervous system (CNS) nosocomial infections. J Microbiol Methods 171:105865. doi:10.1016/j.mimet.2020.10586532057898 · doi ↗ · pubmed ↗
- 6Leitner E, Hoenigl M, Wagner B, Krause R, Feierl G, Grisold AJ. 2016. Performance of the Film Array Blood culture identification panel in positive blood culture bottles and cerebrospinal fluid for the diagnosis of sepsis and meningitis. GMS Infect Dis 4:Doc 06. doi:10.3205/id 00002430671320 PMC 6301725 · doi ↗ · pubmed ↗
- 7Candel FJ, Salavert M, Cantón R, Del Pozo JL, Galán-Sánchez F, Navarro D, Rodríguez A, Rodríguez JC, Rodríguez-Aguirregabiria M, Suberviola B, Zaragoza R. 2024. The role of rapid multiplex molecular syndromic panels in the clinical management of infections in critically ill patients: an experts-opinion document. Crit Care 28:440. doi:10.1186/s 13054-024-05224-339736683 PMC 11687037 · doi ↗ · pubmed ↗
- 8Tunkel AR, Hasbun R, Bhimraj A, Byers K, Kaplan SL, Scheld WM, van de Beek D, Bleck TP, Garton HJL, Zunt JR. 2017. 2017 Infectious Diseases Society of America's clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Crit Care 64:e 34–e 65. doi:10.1093/cid/ciw 861PMC 584823928203777 · doi ↗ · pubmed ↗