Disseminated Mycobacterium intracellulare subsp. chimaera infection, undiagnosed for years, highlights the enduring clinical utility of “old school” microbiological testing and a robust differential
Ayesha Khan

TL;DR
A rare Mycobacterium infection in a patient with a history of heart surgery went undiagnosed for years, highlighting the importance of traditional microbiological testing and clinical suspicion.
Contribution
The case emphasizes the enduring value of conventional microbiological methods in diagnosing complex, delayed-onset infections.
Findings
Disseminated Mycobacterium intracellulare subsp. chimaera infections can remain undiagnosed for years without proper clinical suspicion.
Traditional culture-based testing can be more timely and cost-effective than next-generation sequencing for diagnosing such infections.
Delayed diagnosis can lead to severe complications, such as central nervous system involvement.
Abstract
Disseminated Mycobacterium intracellulare subsp. chimaera (MC) infections are rare, slow-progressing, and easily overlooked, particularly when a patient’s history of prior cardiac surgery is not incorporated into the diagnostic evaluation. In a recent ASM Case Reports article (1:e00003-25, 2025, https://doi.org/10.1128/asmcr.00003-25), Ladines-Lim et al. describe a disseminated MC infection in a patient with prior aortic and mitral valve replacement that remained undiagnosed for over 4 years. Conventional microbiological testing was not pursued early in the course of illness because the history of cardiopulmonary bypass was not linked with the constellation of unexplained symptoms. This case urges clinicians to remain vigilant and suspect MC in patients with prior open-chest cardiac surgery who present with gradually worsening, systemic symptoms. Since 2013, global outbreaks of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
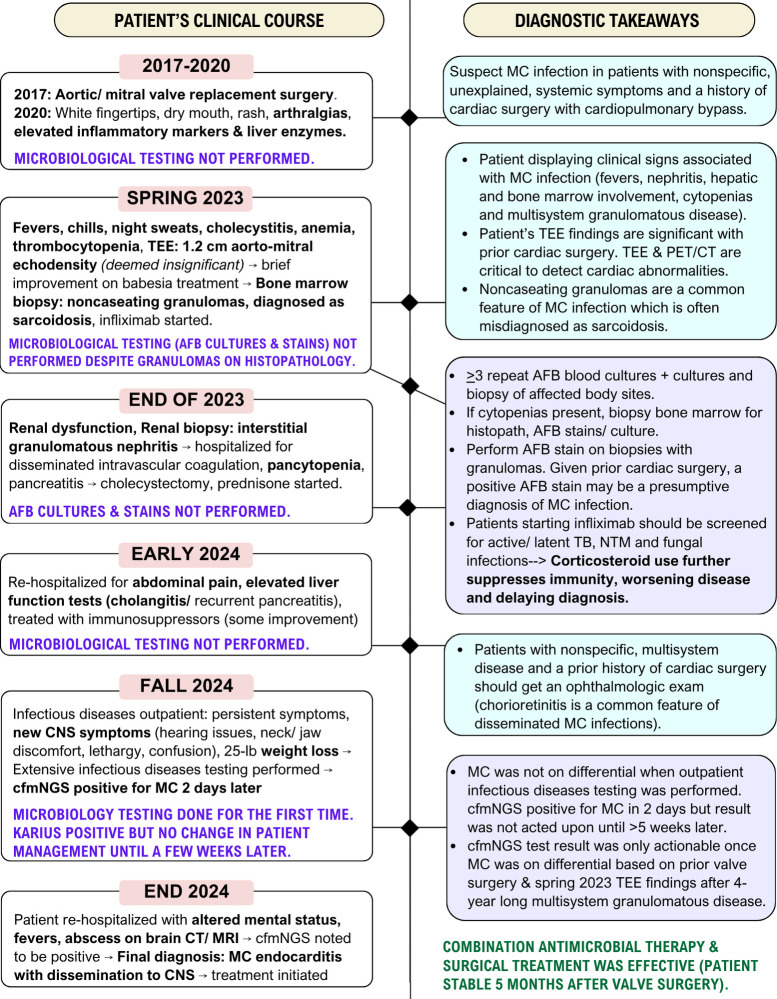 Fig 1
Fig 1| Category | |
|---|---|
| Exposure | History of open-chest cardiac surgery with cardiopulmonary bypass (prosthetic implantations carry the highest risk) |
| Time from surgery to onset of symptoms | Reported average 1.5–3 years, up to 6–7 years |
| Cardiac manifestations |
Endocarditis related to prostheses (prosthetic heart valve, prosthetic graft infection, mechanical circulatory support device) Myocarditis Pseudoaneurysm formation Localized sternal/thoracic wound infection (less common) Mediastinitis |
| Extracardiac or extrathoracic manifestations |
Bloodstream infection/disseminated infection (common) Bone marrow involvement Splenomegaly Bone infection (arthritis, osteomyelitis, spinal involvement) Pneumonitis Hepatitis Nephritis Chorioretinitis (common sign of disseminated infection) Cerebral vasculitis |
| Clinical symptoms |
Recurrent, prolonged fevers of unknown origin Malaise, lethargy Weight loss Night sweats, chills Arthralgias/myalgias Cough, dyspnea (less common) Chest pain (less common) |
| Physical findings |
Frequently normal Heart murmur Hepatosplenomegaly Signs of localized sternal surgical site infection Chorioretinitis (common in disseminated infections) |
| Laboratory findings |
Lymphopenia Thrombocytopenia Anemia Elevated liver enzymes Elevated inflammatory markers |
| Histopathological findings |
Granulomatous infection with multiorgan involvement (noncaseating granulomas and foamy, enlarged macrophages are common on biopsies but not specific to MC and can be seen in Variable AFB smear results |
| Common misdiagnosis | Sarcoidosis |
| Recommended imaging |
Transesophageal echocardiography (more sensitive than transthoracic echocardiography) Positron emission tomography and computed tomography often needed to detect prosthetic valve or aortic graft involvement and determine extent of dissemination |
| Initial microbiological testing is recommended |
AFB culture and histopathology on specimens from other involved body sites (tissue/fluid/abscess, explanted prosthetic material, purulent material in sternal/localized infections) AFB stains on specimens sent for culture and histopathology |
| Follow-up or second-line microbiological testing if it is accessible (guided by a clinical hypothesis and robust differential) |
If cultures grow an organism identified as Direct from sample, targeted, mycobacterial sequencing can be performed on fresh tissue/fluid (preferred) or formalin-fixed paraffin-embedded tissue (highest yield when AFB and/or noncaseating granulomas are seen on specimen) Metagenomic sequencing-based test (Karius) |
| Other high-yield testing is recommended |
Bone marrow biopsy if cytopenias are present Ophthalmologic examination (chorioretinal lesions are a common finding in disseminated MC infection) |
| Antimicrobial susceptibility testing |
General recommendations: Should be performed at experienced and/or reference laboratories If not performed at baseline, isolates should be saved in the event of a recurrent/refractory infection Recommended MIC testing: Clarithromycin (predicts susceptibility to azithromycin, correlates relatively well with treatment outcomes) Amikacin (to optimize dosing) |
| Antimicrobial therapy (often used in conjunction with surgical treatment) |
Combination therapy with 3–4 agents: Macrolide, rifamycin, ethambutol, and amikacin (if tolerated) Second-line agents (if isolate is resistant to macrolides or amikacin, toxicity to first-line agents, or refractory infections): Preferred: Clofazimine (FDA-approved but not commercially available in the United States, requires compassionate use approval and access to drug from the manufacturer) Options with limited clinical data and/or risk of elevated MICs |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Tuberculosis Research and Epidemiology · Medical Device Sterilization and Disinfection
COMMENTARY
In a paper published in ASM Case Reports, Ladines-Lim et al. (1) describe a striking case of disseminated Mycobacterium intracellulare subsp. chimaera (MC) infection in a patient with prior open-chest cardiac surgery. The infection was undiagnosed for over 4 years, despite progressive multisystem disease, because MC was not included in the differential diagnosis, and conventional microbiological testing was not performed. Only after repeated hospitalizations and worsening disease—including central nervous system (CNS) involvement—was the diagnosis confirmed with cell-free metagenomic next-generation sequencing (cfmNGS). This delayed diagnosis underscores the importance of linking unexplained systemic symptoms with prior cardiopulmonary bypass (CPB) exposure, particularly in light of well-documented global outbreaks of delayed-onset, invasive MC infections associated with contaminated heater-cooler devices (HCDs) (2–4). Many hospitals and centers in low-resource settings encounter severe systemic inequities and barriers to replace and monitor such equipment (5).
The patient’s clinical course (2020–2024) highlights key diagnostic pitfalls (Fig. 1). Noncaseating granulomas were identified on biopsy, but acid-fast staining and culture were not performed, leading to a misdiagnosis of sarcoidosis and inappropriate immunosuppressive therapy. A transesophageal echocardiogram later revealed aortic-mitral abnormalities suggestive of endocarditis, but these findings were initially dismissed. When the outpatient cfmNGS test returned positive for MC, there was no immediate follow-up. The result was only acted upon weeks later, after the patient was rehospitalized with worsening CNS involvement.
This sequence of events shows that even advanced diagnostics have limited utility and impact on patients when not anchored to a robust clinical differential, and that delays in follow-up can render otherwise actionable results ineffectual. Importantly, if “old school” microbiological testing, such as mycobacterial (acid fast bacilli; AFB) cultures and stains, had been ordered earlier—guided by a exposure-driven differential—a diagnosis likely could have been established sooner, prompting earlier initiation of therapy. These conventional testing tools are cost-effective, are widely accessible, and can provide clinically actionable results when deployed appropriately (6, 7) (Fig. 1 and Table 1).
Overview of the patient case described by Ladines-Lim et al. with clinical course of illness summarized on the left, and key diagnostic takeaways on the right. Bolded words (black font) are clinical features and findings associated with Mycobacterium intracellulare subsp. chimaera (MC) infections (2, 3, 6, 7). Blue boxes indicate high-yield diagnostic tools based on telltale clinical signs that can facilitate a timely diagnosis. Purple boxes indicate recommended microbiological testing.
Figure 1 summarizes the patient’s clinical course alongside diagnostic takeaways, while Table 1 outlines typical clinical features of MC infection, high-yield testing, and treatment considerations (2, 3, 8). In addition to case series and outbreak investigations, the 2020 International Society of Cardiovascular Infectious Diseases guidelines are a valuable resource (2, 3, 6, 7, 10–15).
CLINICAL TAKEAWAYS
Patients with MC infection often present with nonspecific, slowly progressive symptoms, such as fevers, cytopenias, hepatic or renal involvement, and arthralgias (6, 7) (Table 1). Ophthalmologic exam and cardiac imaging may provide early clues. A transesophageal echocardiogram and nuclear imaging with positron emission tomography and computed tomography scans are often required to detect prosthetic valve involvement or graft infections. However, extrathoracic symptoms can precede cardiac abnormalities, and normal imaging cannot rule out MC infection. MC infections are often misdiagnosed as sarcoidosis due to multisystem granulomatous inflammation, contributing to delayed diagnosis (16–18). These subtleties reinforce the need for vigilance in patients with prior CPB exposure, including those presenting with suspected autoimmune disorders. Management is complex and often requires prolonged multidrug therapy with surgical intervention (3, 6). Culture-based methods have the advantage of enabling phenotypic antimicrobial susceptibility testing (19). Clarithromycin susceptibility testing, which can also predict susceptibility to azithromycin, has been shown to correlate with treatment outcomes (19–22).
MICROBIOLOGY TESTING TAKEAWAYS
Timely microbiological testing is essential for optimal diagnosis and management of MC infections. AFB blood cultures have ~70%–90% sensitivity, with enhanced yield when ≥3 sets are obtained (2, 3, 12, 15, 17). Sampling of multiple involved body sites increases sensitivity. Tissue biopsies should be sent for histopathology, AFB culture, and AFB stains. Negative stain does not rule out MC. Noncaseating granulomas remain a common histopathological feature of MC infections (11, 17, 23, 24). Targeted broad-range mycobacterial sequencing may be useful on fresh tissue and when organisms are visualized in histopathology samples, but is costly and not widely available.
Definitive mycobacterial species identification requires sequencing (16S-23S ITS, rpoB, hsp65) (25). However, in practice, isolation of MAC from blood, tissue, or prosthetic material in a patient with prior CPB exposure is often sufficient to initiate treatment. While culture turnaround times are long, early suspicion enables timely testing, balancing delays with the accessibility and affordability of traditional microbiological methods.
NEXT-GENERATION SEQUENCING ASSAYS
This case also offers broader lessons on the role of NGS in clinical practice. Although rapidly advancing NGS technologies hold great promise, their clinical utility is highly contextual. NGS assays should be reserved for select scenarios: diagnosis of elusive infections in high-risk patients, scenarios where front-line testing is unrevealing, when conventional testing is unlikely to detect the suspected pathogen or suffers from long turnaround times (26).
The value of rapid cfmNGS tests is diminished if results are not interpreted effectively and acted upon promptly. Access and cost also remain major barriers to clinical implementation, limiting availability of NGS assays to well-resourced academic medical centers, and insurance coverage is inconsistent (27). Studies on universal, unchecked utilization of NGS show low diagnostic yield and lack of clinical utility (28–30). NGS tests are prone to overuse and misuse, which risks financial burden for patients and undermines confidence in such assays.
Diagnostic stewardship— thoughtful test selection grounded in a robust differential, ordered in the right clinical context, and interpreted through close collaboration between clinicians and microbiologists—is essential for maximizing the benefit of NGS assays. This case shows that NGS is only as useful as the clinical reasoning that guides its use.
CONCLUSIONS
Since 2013, global outbreaks of invasive MC infections have been linked to contaminated HCDs used during cardiac surgery (6, 12, 31). MC infections can manifest years after exposure and carry mortality rates of 50%–70% (7, 15, 19). Despite warnings from the US Food and Drug Administration and recommended mitigation measures, the implicated devices (LivaNova) remain in use, and the infection control measures required to replace or decontaminate them may not be feasible in resource-limited settings (6). Clinicians should maintain a high index of suspicion for MC in patients with prior open-chest cardiac surgery who present with nonspecific systemic symptoms. Early suspicion guides appropriate testing, timely treatment, and improved outcomes.
Importantly, this case reminds us that traditional “old-school” microbiological testing- cultures, stains, and histopathology- remain indispensable. These widely accessible, cost-effective tools often yield clinically actionable results when guided by a rationale differential (Table 1). Continued efforts to refine and optimize these fundamental diagnostic tests remain essential, particularly for underserved communities that bear a disproportionate burden of infectious diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ladines-Lim JB, Yang W-T, Tebas P, O’Donnell J, Koenig H, Kreider E, Dyer K, Anwar M, Rodriguez E, Patel S, Rodino K, Glaser L, Richterman A. 2025. Delayed diagnosis of disseminated Mycobacterium intracellulare subsp. chimaera infective endocarditis via cell-free metagenomic next-generation sequencing: a case report. ASM Case Rep 1:e 00003–25. doi:10.1128/asmcr.00003-2541244979 PMC 12530230 · doi ↗ · pubmed ↗
- 2Hasse B, Hannan MM, Keller PM, Maurer FP, Sommerstein R, Mertz D, Wagner D, Fernández-Hidalgo N, Nomura J, Manfrin V, et al.. 2020. International society of cardiovascular infectious diseases guidelines for the diagnosis, treatment and prevention of disseminated Mycobacterium chimaera infection following cardiac surgery with cardiopulmonary bypass. J Hosp Infect 104:214–235. doi:10.1016/j.jhin.2019.10.00931715282 · doi ↗ · pubmed ↗
- 3Kasperbauer SH, Daley CL. 2019. Mycobacterium chimaera infections related to the heater–cooler unit outbreak: a guide to diagnosis and management. Clin Infect Dis 68:1244–1250. doi:10.1093/cid/ciy 78930371755 · doi ↗ · pubmed ↗
- 4Achermann Y, Rössle M, Hoffmann M, Deggim V, Kuster S, Zimmermann DR, Bloemberg G, Hombach M, Hasse B. 2013. Prosthetic valve endocarditis and bloodstream infection due to Mycobacterium chimaera. J Clin Microbiol 51:1769–1773. doi:10.1128/JCM.00435-1323536407 PMC 3716099 · doi ↗ · pubmed ↗
- 5Chandrasekar H, Hoganson DM, Lachenauer CS, Newburger JW, Sandora TJ, Saleeb SF. 2022. Mycobacterium chimaera outbreak management and outcomes at a large pediatric cardiac surgery center. Ann Thorac Surg 114:552–559. doi:10.1016/j.athoracsur.2021.07.07434454904 · doi ↗ · pubmed ↗
- 6Tan NY, Tarabochia AD, De Simone DC, De Simone CV, Wilson JW, Bagameri G, Bennett CE, Abu Saleh OM. 2021. Updated experience of Mycobacterium chimaera infection: diagnosis and management in a tertiary care center. Open Forum Infect Dis 8:ofab 348. doi:10.1093/ofid/ofab 34834377729 PMC 8339283 · doi ↗ · pubmed ↗
- 7Julian KG, Crook T, Curley E, Appenheimer AB, Paules CI, Hasse B, Diekema DJ, Daley CL, de Sanctis J, Hellinger WC, Levin A, Mc Sherry G, Freer C, Whitener CJ. 2020. Long-term follow-up of post-cardiac surgery Mycobacterium chimaera infections: a 5-center case series. J Infect 80:197–203. doi:10.1016/j.jinf.2019.12.00731863789 · doi ↗ · pubmed ↗
- 8Mason M, Gregory E, Foster K, Klatt M, Zoubek S, Eid AJ. 2022. Pharmacologic management of Mycobacterium chimaera infections: a primer for clinicians. Open Forum Infect Dis 9:ofac 287. doi:10.1093/ofid/ofac 28735866101 PMC 9297092 · doi ↗ · pubmed ↗