Septic arthritis due to Corynebacterium propinquum: first report of isolation from synovial fluid in a native joint
Rudolf Kotula, Anna Kotula, Nagarjuna Reddy Cheemarla

TL;DR
This paper reports the first case of septic arthritis caused by Corynebacterium propinquum in a native joint, emphasizing the importance of proper diagnostic techniques.
Contribution
The first documented isolation of Corynebacterium propinquum from synovial fluid in a native joint septic arthritis case.
Findings
Corynebacterium propinquum was isolated from synovial fluid using enrichment culture techniques.
The patient showed clinical improvement after treatment with daptomycin and ceftriaxone.
The case underscores the need for accurate identification and clinical correlation to distinguish true infection from contamination.
Abstract
Septic arthritis of native joints remains an uncommon but serious clinical condition affecting approximately two per 100,000 individuals annually. The synovial membrane, being highly vascular and lacking a protective basement membrane, is particularly susceptible to hematogenous bacterial seeding, especially in patients with pre-existing joint disease. Corynebacterium propinquum, typically regarded as a respiratory commensal, has rarely been implicated in deep-seated infections. We report the first known case of C. propinquum isolated from synovial fluid in a patient with native knee septic arthritis. The 59-year-old female had a history of bilateral knee osteoarthritis and recent intra-articular corticosteroid injections. Initial synovial fluid cultures were negative; however, enrichment using aerobic blood culture bottles, followed by subculture, yielded C. propinquum identified by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
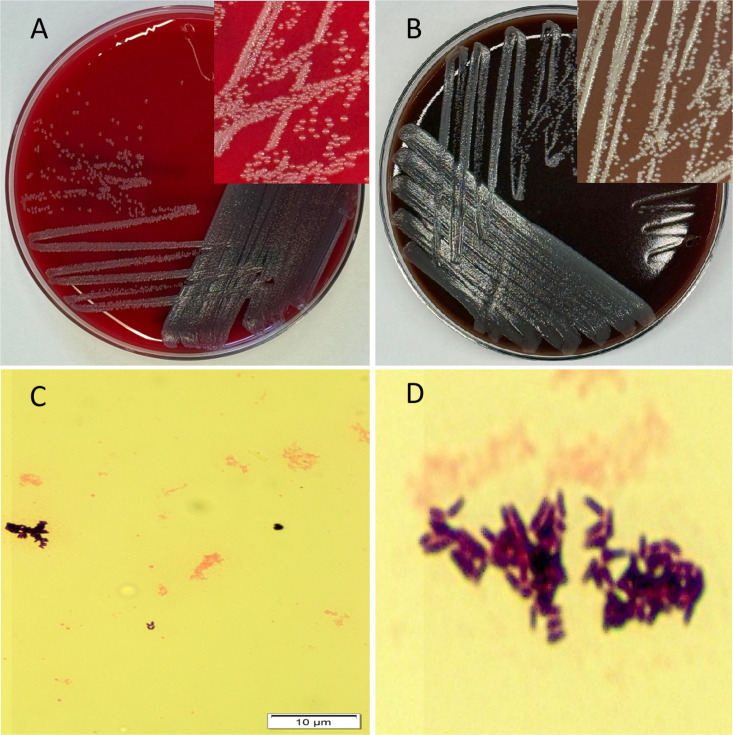 Fig 1
Fig 1| Antimicrobial agent | MIC (µg/mL) | Interpretation |
|---|---|---|
| Ceftriaxone | 0.12 | Susceptible |
| Clindamycin | ≥4 | Resistant |
| Doxycycline | ≤0.25 | Susceptible |
| Erythromycin | 4 | Resistant |
| Gentamicin | ≤2 | Susceptible |
| Levofloxacin | 0.5 | Not reported |
| Linezolid | 0.5 | Susceptible |
| Trimethoprim–sulfamethoxazole | ≥4/76 | Resistant |
| Meropenem | ≤0.016 | Susceptible |
| Penicillin | ≤0.03 | Susceptible |
| Vancomycin | 0.5 | Susceptible |
| Case | Reference | Country | No. of patients | Age (yrs) | Sex | Clinical syndrome | Risk/host factors | Culture source | Identification method | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Jangda et al. ( | USA | 1 | 48 | M | Prosthetic mitral-valve endocarditis | Prosthetic valve; RA | Blood culture | Phenotypic methods (MALDI-TOF not reported) | Empiric vancomycin, cefepime, gentamicin → targeted ceftriaxone | Survived |
| 2 | Kuriakose et al. ( | USA | 1 | 63 | M | Native-valve | T2DM, COPD, brain infarction | Blood culture | NR | Empiric | Survived |
| 3 | Motomura et al. ( | Japan | 3 | NT | NT | Respiratory infections | Elderly adults (per abstract) | Sputum | Biochemical | NT | NT |
| 4 | Kawasaki et al. ( | Japan | 1 | 7 | F | Native tricuspid-valve infective endocarditis | Ventricular septal defect (VSD), ventriculoatrial communication, | Blood culture | API Coryne biochemical | Ceftriaxone + gentamicin → ampicillin + | Clinical cure after prolonged therapy |
| 5 | Fernández-Vecilla et al. ( | Spain | 1 | 64 | M | Late-onset endophthalmitis | T2DM, proliferative diabetic retinopathy w/ diabetic macular edema | Aqueous humor, vitreous humor, and vitrectomy cassette | 16S rDNA sequencing | Intravitreal vancomycin + ceftazidime and intracameral cefuroxime at presentation; systemic oral ciprofloxacin plus topical moxifloxacin and dexamethasone/tobramycin eye drops | Partial recovery of vision |
| 6 | Megdich et al. ( | Tunisia | 1 | 52 | M | Native-valve infective endocarditis | Acute articular rheumatism | Blood cultures | Biochemical tests + 16S rRNA sequencing | Vancomycin → valve surgery | Survived |
| 7 | Yukari et al. ( | Japan | 1 | 84 | F | Microbial keratitis after AM transplantation | AM graft; chronic ocular disease; steroid drops | Corneal | MALDI-TOF MS (score 2.371) | Gentamicin + gatifloxacin | Improved (vision unchanged) |
| 8 | Present case | USA | 1 | 59 | F | Native knee septic arthritis | Repeated intra-articular | Synovial fluid (aerobic bottle only) | MALDI-TOF MS (FDA-cleared library) | Daptomycin → ceftriaxone | Full recovery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiphtheria, Corynebacterium, and Tetanus · Orthopedic Infections and Treatments · Intramuscular injections and effects
INTRODUCTION
Septic arthritis is a medical emergency that can result in rapid joint destruction and permanent disability if not promptly diagnosed and treated. While Staphylococcus aureus and Streptococcus species are the most frequently isolated pathogens, infections due to Corynebacterium species are rare and often overlooked because they are typically considered commensal skin flora. Among these, Corynebacterium propinquum, a species commonly found in the upper respiratory tract, has infrequently been reported as a cause of invasive disease. We describe the first known case of C. propinquum septic arthritis in a native joint and review the relevant literature.
CASE PRESENTATION
A 59-year-old woman with a history of severe bilateral knee osteoarthritis presented with acute worsening of right knee pain, swelling, and restricted range of motion. Her medical history included multiple intra-articular corticosteroid injections, reportedly over 10, with the most recent administered 2 weeks prior to the symptom onset. She had also returned from travel to Mexico within the past month. Despite chronic joint issues, she remained ambulatory and had returned to her orthopedic specialist due to progressive symptoms. Physical examination revealed significant right knee effusion, warmth, erythema, and tenderness with limited flexion. Laboratory studies showed leukocytosis (peak white blood cell 12.2 × 10^3^/μL; reference range 4–11 × 10^3^/μL), elevated C-reactive protein (92.6 mg/L; reference range 0–5 mg/L), and platelet count of 477,000/μL (reference range 150–450 × 10^3^/μL). Antinuclear antibodies were negative. Ultrasound of the lower extremity ruled out deep vein thrombosis.
Three synovial fluid specimens were available for microbiologic evaluation. Two aspirates were obtained in the outpatient orthopedic clinic several days apart, and a third specimen was collected intraoperatively at the time of arthroscopic irrigation and debridement. All three specimens underwent identical laboratory processing.
Arthrocentesis revealed elevated synovial white blood cell counts (ranging between 14,180 and 30,090 cells/μL; reference range 0–200 cells/μL), with uric acid crystals noted on one occasion. Direct Gram stains showed many white blood cells but no organisms. Each specimen was processed according to our institutional synovial fluid culture protocol. Fluid was inoculated onto Remel (Lenexa, KS) tryptic soy agar with 5% sheep blood (TSA-5%) and chocolate agar (both 35°C, 5% CO_₂_), MacConkey agar and thioglycolate broth (35°C**,** ambient air), and an anaerobic CDC blood agar plate (Remel) incubated at 35°C in an anaerobic jar/bag. In addition, when volume permitted, equal aliquots (1–10 mL per bottle; minimum 1 mL) were inoculated into BD Bactec Plus Aerobic F and BD Bactec Lytic Anaerobic F bottles and monitored on the BD BACTEC System; specimens ≤3 mL were cultured only on solid media. Plates were held as follows: aerobic blood agar 3 days**,** anaerobic blood agar 5 days**,** and thioglycolate broth 5 days with subculture as indicated. Blood culture bottles were incubated per instrument protocol (up to 5 days). In all three samples, only the aerobic blood culture bottle(s) flagged positive. No growth was observed on direct plates, thioglycolate broth, or anaerobic cultures. The aerobic blood-culture bottles became positive at 2, 3, and 4 days, respectively, yielding a median time-to-positivity of 3 days (range, 2–4 days). Blind Gram stains of the anaerobic media confirmed the absence of growth.
Subcultures from the positive aerobic blood culture bottles yielded small, non-hemolytic gray colonies on blood agar after 48 h of incubation in 5% CO_₂_. No anaerobic growth was observed. Identification was performed using the Bruker MALDI Biotyper CA System (Bruker Daltonics GmbH, Germany) operating with the FDA-cleared reference library claim 4 (MALDI Biotyper CA System software), which yielded a high-confidence identification of Corynebacterium propinquum (score 2.13). No RUO database or Vitek MS System was used, and confirmatory gene sequencing was not performed. Gram stain of the isolate showed club-shaped, palisading gram-positive bacilli in a characteristic picket-fence/pickup-sticks arrangement consistent with Corynebacterium spp. morphology. For documentation purposes, representative colony morphology was photographed from a fresh subculture of the archived isolate (Fig. 1).
Morphology and growth characteristics of C. propinquum. (A) Growth on blood agar under aerobic conditions showing small gray, non-hemolytic colonies. (B) Growth on chocolate agar under aerobic conditions from the stocked isolate. Inset: magnified view of colony morphology. (C) Gram stain of the isolate (100× magnification). (D) Zoomed-in view of the Gram stain highlighting palisading coryneform bacilli arranged in a classic picket-fence/pickup-stick arrangement.
The isolate was referred to ARUP Laboratories (Salt Lake City, Utah) for antimicrobial susceptibility testing by broth microdilution (Sensititre System from Trek Diagnostics), with results interpreted using CLSI M45 (3rd edition) breakpoints for Corynebacterium species. The organism was susceptible to ceftriaxone (MIC 0.12 µg/mL), doxycycline (≤0.25 µg/mL), gentamicin (≤2 µg/mL), linezolid (0.5 µg/mL), meropenem (≤0.016 µg/mL), penicillin (≤0.03 µg/mL), and vancomycin (0.5 µg/mL) and resistant to clindamycin (≥4 µg/mL), erythromycin (4 µg/mL), and trimethoprim-sulfamethoxazole (≥4/76 µg/mL). Levofloxacin MIC was 0.5 µg/mL; no categorical interpretation was available because CLSI M45 does not provide breakpoints for fluoroquinolones in Corynebacterium species. Detailed MIC results are summarized in Table 1.
Figure 1 illustrates the growth and morphology of the isolate. Panels A and B show colony morphology (gray colonies) on aerobic blood agar and chocolate agar from a fresh subculture of the archived isolate (inset: magnified view); Panel C demonstrates the Gram stain morphology with typical coryneform bacilli; and Panel D shows a magnified view of palisading bacilli arranged in a characteristic picket-fence/pickup-sticks pattern.
The patient was evaluated in the Outpatient Infectious Diseases Clinic, after which she was admitted the following day for surgical management. She underwent right knee arthroscopic irrigation and debridement on the day of admission. Intravenous daptomycin (6 mg/kg every 24 h) was initiated at that time and continued for approximately 2 weeks with weekly creatine kinase monitoring, all of which remained within reference limits. Therapy was then transitioned to intravenous ceftriaxone (2 g every 24 h) to complete a total of 6 weeks of parenteral antimicrobial treatment. She experienced full symptom resolution and returned to baseline joint function by the end of therapy.
DISCUSSION
Corynebacterium propinquum is a non-diphtherial, gram-positive bacillus that resides primarily in the upper respiratory tract and has historically been regarded as a commensal organism. In recent years, however, it has emerged as a potential opportunistic pathogen, particularly in immunocompromised hosts or when isolated from normally sterile body sites (1–7).
From a microbiologic standpoint, Corynebacterium propinquum belongs to the group of nondiphtherial corynebacteria that are typically nonlipophilic and nonfermentative, consistent with descriptions of the C. pseudodiphtheriticum group (8–10). This contrasts with clinically important lipophilic, nonfermentative species, such as C. jeikeium and C. urealyticum, which require lipid supplementation, grow slowly, and are frequently multidrug-resistant (8–10). In comparison, C. striatum is nonlipophilic but fermentative and has emerged as a multidrug-resistant nosocomial pathogen, including as a documented cause of bone and joint infections and native-joint septic arthritis (11). By contrast, C. minutissimum is nonlipophilic and fermentative but is primarily associated with superficial skin infections, such as erythrasma, rather than invasive disease (8–10). Within this broader taxonomic context, published invasive C. propinquum isolates have generally demonstrated broader antimicrobial susceptibility than C. jeikeium or C. striatum, which aligns with the relatively susceptible phenotype observed in our case.
In this report, we describe the isolation of C. propinquum from the synovial fluid of a patient with native joint septic arthritis, a highly unusual and, to our knowledge, previously unreported clinical scenario. Importantly, the organism was isolated consistently from three separate synovial fluid specimens, each yielding growth solely in aerobic blood culture bottles, while direct plating and thioglycolate enrichment remained negative. This pattern suggests a low organism burden or a degree of fastidiousness not typically attributed to C. propinquum and highlights the clinical utility of inoculating synovial fluid into blood culture bottles to increase the diagnostic yield.
In fact, the preferential recovery of this isolate from aerobic blood culture bottles aligns with published evidence supporting the use of blood culture systems as enrichment media for synovial fluid. Multiple studies have demonstrated that inoculating synovial fluid into blood culture bottles increases the diagnostic yield for both native and prosthetic joint infections by improving recovery of fastidious or low-inoculum organisms. Font-Vizcarra et al. showed that blood culture flasks significantly enhanced recovery of pathogens from synovial fluid in prosthetic joint infections compared with direct plating alone (12). Similarly, the 2018 International Consensus Meeting (ICM) on Musculoskeletal Infection recommends inoculation of synovial fluid into aerobic and anaerobic blood culture bottles to improve sensitivity, especially when only small volumes are available (13). These data support our findings and reinforce that enrichment systems can be critical for detecting uncommon pathogens, such as Corynebacterium propinquum (12–14).
The repeated isolation of the same organism from a sterile site supports its etiologic significance in this case. While coryneform bacteria are often considered contaminants, especially when isolated from non-sterile sites, the context here is critical. The organism was recovered from a sterile compartment on multiple occasions in a symptomatic patient with classic clinical findings of septic arthritis. Such concordant evidence strengthens the case for true infection rather than colonization or contamination (1–7).
Our isolate of C. propinquum demonstrated a generally favorable susceptibility profile (ceftriaxone 0.12 µg/mL, penicillin ≤0.03 µg/mL, vancomycin 0.5 µg/mL) consistent with previously published cases of this species in invasive infections, which also reported broad susceptibility to β-lactams and glycopeptides (1, 3, 5, 7, 15). In contrast, C. striatum and other nondiphtherial Corynebacterium species have emerged as frequently multidrug-resistant pathogens, with decreased susceptibility to many β-lactams, macrolides, fluoroquinolones, and trimethoprim-sulfamethoxazole, although vancomycin largely retains activity (15, 16). Hence, while our patient’s isolate demonstrated an ‘expected’ phenotype for C. propinquum, this underscores the importance of species-level identification and AST given the broader genus may not behave the same way. Given the increasing recognition of resistance among nondiphtherial corynebacteria, susceptibility testing is warranted when such organisms are recovered from sterile sites.
From a diagnostic standpoint, Gram stain morphology was also informative: palisading, club-shaped gram-positive bacilli arranged in irregular, angular clusters provided a strong presumptive clue, reinforcing the importance of early microscopy in guiding organism workup. Growth on blood agar, along with lack of anaerobic growth, was consistent with the organism’s known aerobic physiology.
The recovery of this organism was made possible by modern species-level identification techniques. While tools, such as MALDI-TOF MS, are now routine in clinical microbiology laboratories, their broad implementation has greatly improved recognition of previously underappreciated or misidentified species as potential pathogens. C. propinquum may have been similarly overlooked in past cases of septic arthritis before the adoption of these technologies.
To place our case in context, we reviewed prior reports of C. propinquum infections (Table 2). Although uncommon, these infections have occurred across diverse clinical settings and syndromes, suggesting that the organism’s rarity likely reflects underrecognition rather than true scarcity. Reported cases collectively support its ability to cause disease in both immunocompromised and immunocompetent hosts when isolated from sterile body sites.
This case underscores the diagnostic challenges posed by unusual or fastidious organisms recovered from sterile fluids such as synovial aspirates. C. propinquum, while often regarded as a commensal, can cause clinically meaningful infections when isolated repeatedly in an appropriate clinical context. The use of enrichment culture and MALDI-TOF MS facilitated accurate detection and timely identification. Greater awareness, continued case reporting, and standardized susceptibility testing will be essential to define its epidemiology, virulence potential, and antimicrobial resistance patterns.
In conclusion, our findings contribute to the growing evidence that non-diphtherial Corynebacterium species, including C. propinquum, should not automatically be dismissed as contaminants. Rather, their presence in multiple concordant cultures from a compatible clinical syndrome should prompt careful evaluation and correlation with host factors and infection site.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jangda U, Upadhyay A, Bagheri F, Patel NR, Mendelson RI. 2016. Corynebacterium propinquum: a rare cause of prosthetic valve endocarditis. Case Rep Med 2016:1391789. doi:10.1155/2016/139178927891149 PMC 5116497 · doi ↗ · pubmed ↗
- 2Motomura K, Masaki H, Terada M, Onizuka T, Shimogama S, Furumoto A, Asoh N, Watanabe K, Oishi K, Nagatake T. 2004. Three adult cases with Corynebacterium propinquum respiratory infections in a community hospital. kansenshogakuzasshi 78:277–282. doi:10.11150/kansenshogakuzasshi 1970.78.27715103912 · doi ↗ · pubmed ↗
- 3Kuriakose K, Rutland J, Watts TE, Chatterjee K, Rochlani Y, Burns M. 2017. A rare case of Corynebacterium propinquum endocarditis in a native valve. J Med Cases 8:137–140. doi:10.14740/jmc 2795 w · doi ↗
- 4Fernández-Vecilla D, Blasco-Palacio PB, Pérez-Ramos IS, Unzaga-Barañano MJ. 2023. Corynebacterium propinquum, a rare cause of late endophtalmitis. Enferm Infecc Microbiol Clin (Engl Ed) 41:518–519. doi:10.1016/j.eimce.2023.03.00437024377 · doi ↗ · pubmed ↗
- 5Kawasaki Y, Matsubara K, Ishihara H, Nigami H, Iwata A, Kawaguchi K, Fukaya T, Kawamura Y, Kikuchi K. 2014. Corynebacterium propinquum as the first cause of infective endocarditis in childhood. J Infect Chemother 20:317–319. doi:10.1016/j.jiac.2013.10.01324486166 · doi ↗ · pubmed ↗
- 6Yukari Y, Shimizu T, Hayashi T, Hara Y, Igarashi A, Yamagami S. 2025. A case of Corynebacterium propinquum microbial keratitis after amniotic membrane transplantation. BMC Ophthalmol 25:314. doi:10.1186/s 12886-025-04159-940426083 PMC 12107768 · doi ↗ · pubmed ↗
- 7Megdich Z, Ferjani A, Ferjani S, Kanzari L, Fakhfakh A, Rehaiem A, Boutiba-Ben Boubaker I. 2025. Corynebacterium propinquum: a confounding case of infective endocarditis. Acta Microbiol Immunol Hung 72:68–71. doi:10.1556/030.2025.0253240085156 · doi ↗ · pubmed ↗
- 8Mitchell BI, Markantonis JE. 2025. An underestimated pathogen: Corynebacterium species. J Clin Microbiol 63:e 0155224. doi:10.1128/jcm.01552-2440833082 PMC 12506004 · doi ↗ · pubmed ↗