Invasive Conidiobolus infection in an immunocompromised pediatric patient in Southern California
Jacky Lu, Samuel M. Goodfellow, Esther Vaugon, Andrew Karnaze, Cristina Costales, Michael A. Smit, Jennifer Dien Bard

TL;DR
A 15-year-old immunocompromised boy in California developed a rare invasive fungal infection caused by Conidiobolus, which was identified through advanced DNA sequencing and treated with antifungal drugs.
Contribution
Reports a rare case of invasive Conidiobolus infection in a pediatric immunocompromised patient in North America.
Findings
Conidiobolus species were identified as the causative agent through plasma cell-free DNA sequencing.
The organism showed high resistance to antifungal agents in vitro.
The patient was successfully treated with posaconazole and trimethoprim-sulfamethoxazole.
Abstract
Conidiobolus species are largely known to cause rhinofacial cellulitis in healthy individuals but can manifest as an invasive infection in immunocompromised patients. Few cases have been described in the literature as they are difficult to diagnose and rarely observed in North America, particularly in the pediatric population. A 15-year-old boy with a history of multiple bone marrow transplants for mixed phenotype acute leukemia presented to the emergency department with febrile neutropenia and chills. His clinical course was complicated by potential Rothia mucilaginosa bacteremia, but imaging revealed a potential invasive pulmonary fungal infection. Following rapid decompensation and admission in the intensive care unit, plasma cell-free DNA sequencing was ordered, identifying Conidiobolus species. The same organism was then isolated in the patient’s sputum culture shortly thereafter.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
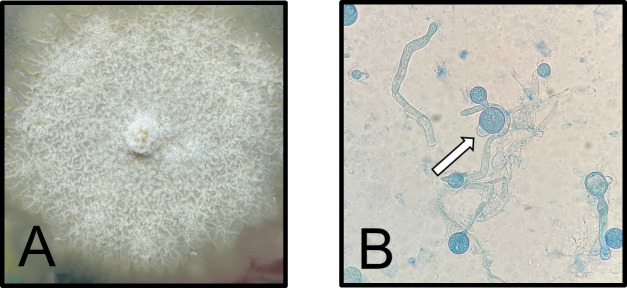 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Mycology · Sinusitis and nasal conditions · Infectious Diseases and Tuberculosis
INTRODUCTION
Conidiobolus belongs to the Entomophthorales group and is closely related to the Mucorales group (1). Historically, these groups both belonged to the phylum Zygomycota. Following a comprehensive phylogenetic study based on multigene sequence analysis, the order Mucorales now falls under the subphyla of Mucoromycotina, while the order Entomophthorales is part of the Entomophthoromycotina subphyla (2). Whereas the Mucorales group is known to cause invasive disease in immunocompromised patients and through direct inoculation during trauma, Conidiobolus species are a known cause of conidiobolomycosis. The most common manifestation is rhinofacial cellulitis, which may lead to chronic facial deformity in immunocompetent hosts (3–5). However, few cases of Conidiobolus invasive infection have been described in the literature, infecting other viscera or the central nervous system and often involving multiple organs (6). Due to their growth requirements of high-level humidity, it has been postulated that pathogenicity may be limited to tropical or subtropical regions (4). Diagnosis generally relies on histological examination of biopsied or resected tissue, as cultures show poor recovery of the causative organism, negative in more than 85% of cases (7). Similar to fungal species in the Mucorales group, the fungal antigen (1,3)-beta-D-glucan test is often negative in Entomophthorales, despite the presence of significant amounts of (1,3)-D-beta-glucan in the cell wall (4), although most cases are localized. Detection of (1,3)-beta-D-glucan in patients with disseminated Conidiobolus infections has been inconsistent and may be species dependent (1, 8). Here, we describe a rare case of invasive Conidiobolus infection in an immunocompromised patient in Southern California.
CASE PRESENTATION
A 15-year-old male presented to the emergency department (ED) with chills and fever (maximum temperature: 39.6°C) in the setting of neutropenia following chemotherapy at an urban academic, pediatric quaternary-care center in Southern California. The patient had received his third bone marrow transplantation (matched unrelated donor peripheral blood stem cell) 20 months prior to hospital admission with leukemic relapse 11 months later and was receiving palliative chemotherapy with azacitidine, venetoclax, and gemtuzumab for active leukemic disease. He has had a history of graft-versus-host disease (GVHD) of the skin (stage 3) after completion of GVHD prophylaxis, 53 days post-transplant, which had since resolved. On admission to the oncology unit, at 9 months after his most recent relapse, he had an absolute neutrophil count of 0.00 and an elevated C-reactive protein level of 22.9 mg/dL (normal level: <0.9 mg/dL). A single blood culture set (aerobic and anaerobic bottles) was collected in the ED, and Rothia mucilaginosa was recovered from a single aerobic blood culture bottle after 13.5 hours of incubation. While the significance of this culture result was unclear, he was started on vancomycin (500 mg, IV intermittent, Q8H) and maintained on cefepime (1,500 mg, IV, Q8H) for broad gram-negative coverage. Prior to hospital admission, he was receiving prophylactic trimethoprim-sulfamethoxazole (400 mg–80 mg oral tablet, PO, BID SaSu) and levofloxacin (250 mg, PO, Q24H). Vancomycin was discontinued after 6 days as the patient showed improvement, and subsequent blood cultures were negative.
Due to his prolonged febrile neutropenia despite broad-spectrum antibiotics, CT scans of the chest, abdomen, and pelvis with contrast were performed, which showed signs of left lower lobe pneumonia. The patient was on room air and not short of breath or tachypneic but was complaining of left flank pain. There was concern that the etiology of the pneumonia could have been R. mucilaginosa (9), given prior blood culture results, versus a fungal etiology. Of note, the patient had already been on therapeutic dosing of isavuconazonium (372 mg, PO, Q24H) for treatment of pulmonary aspergillosis diagnosed 9 months earlier. Therefore, there was concern for the development of resistant pulmonary aspergillosis, given reports of poor compliance with isavuconazonium, versus a new fungal pneumonia. Both serum (1,3)-beta-D-glucan (reference range: <31 pg/mL) and Aspergillus galactomannan were negative (reference range: <0.5 optical density index), and the patient remained stable with no progression of pulmonary symptoms.
However, 2 days after his CT scans, he was transferred to the pediatric intensive care unit (PICU) for hypotension secondary to a suspected gastrointestinal bleed. Due to his prolonged febrile neutropenia despite broad-spectrum antimicrobials, imaging suggestive of invasive fungal infection, and inability to collect bronchioloalveolar lavage (BAL) due to clinical instability, plasma cell-free DNA metagenomic next-generation sequencing (mNGS) testing (Karius Spectrum, Redwood City, CA, USA) was approved by the medical microbiologist. At the time of plasma collection, the patient was empirically treated with isavuconazonium, with proper compliance for at least 13 days since admission. A positive report for Conidiobolus incongruus (2,327 molecules per 100 nL) was received 2 days after collection (day 16 of admission).
Based on previous case reports and the variable resistance of C. incongruus, its detection prompted initiation of liposomal amphotericin B (150 mg, IV, QDay) and IV trimethoprim-sulfamethoxazole ([80 mg–16 mg/mL IV solution] 160 mg, IV, Q8H) and evaluation by otolaryngology. Nasal endoscopic exam was normal, and CT scan of the sinuses did not reveal evidence of rhinosinusitis. Due to his recent GI bleed and ongoing thrombocytopenia, a biopsy was not recommended for the patient’s safety. Ultrasound of the chest showed a large left pleural effusion.
A sputum sample was successfully collected on day 16 of hospitalization (day 3 in PICU) and submitted to the microbiology laboratory for bacterial and fungal cultures. The Gram stain revealed few white blood cells, few squamous epithelial cells, and no organisms seen. Mold was recovered from chocolate agar 48 hours after incubation at 37°C in 5% CO_2_, along with normal respiratory flora. Following subculture to Sabouraud dextrose agar, the mold was macroscopically described as flat, waxy, and buff colored with white aerial hyphae after 3 days of incubation at 30°C in ambient air (Fig. 1A). Microscopic examination with lactophenol blue revealed unbranched non-septate hyphae resembling the Mucorales group. Conidia with prominent papillae were also observed (Fig. 1B). The mold was reported as Conidiobolus spp. solely based on microscopic morphology. Testing by MALDI-TOF MS (MALDI Biotyper, Bruker) was attempted but was unsuccessful in yielding sufficient spectra score for pathogen identification, highlighting the difficulty of identifying uncommon molds by this method. The isolate was sent to the University of Texas Health, South Texas Reference Laboratories in San Antonio for antifungal susceptibility testing and confirmation by ITS sequencing, which identified the organism to the genus level. In vitro susceptibility testing revealed the following minimum inhibitory concentration (MIC): amphotericin B (MIC, 1 mcg/mL), itraconazole (MIC, >16 mcg/mL), posaconazole (MIC, >16 mcg/mL), and isavuconazole (MIC, >16 mcg/mL). There are no available clinical breakpoints from the Clinical and Laboratory Standards Institute (CLSI) or European Committee on Antimicrobial Susceptibility Testing (EUCAST).
Conidiobolus spp. isolated from sputum. (A) Macroscopic examination of mold grown on Sabouraud dextrose agar after 3 days at 30°C. (B) Lactophenol blue preparation of mold examined at ×40. Conidia with prominent papillae were observed (arrow).
Given the prognosis of invasive fungal infection, a multidisciplinary care team made the decision to de-escalate harmful medical interventions, including IV liposomal amphotericin B, and focus on comfort care. The patient was ultimately discharged on trimethoprim-sulfamethoxazole (160 mg PO, TID), posaconazole (300 mg PO, QD), and prophylactic levofloxacin (250 mg PO, QD) on day 26 of hospital admission. The patient is being followed by the outpatient clinic.
DISCUSSION
There have been only 10 cases of invasive Conidiobolus spp. (including C. incongruus, C. coronatus, and C. lamprauges) infection described in the literature since 2020 (6). However, the true number of invasive cases is likely underreported as this organism is notoriously difficult to recover by culture, and infections largely occur in underresourced regions (4). Of the 10 invasive cases reviewed by Stavropoulou et al., which encompasses all the cases since the one we are reporting, 7 had multiorgan with pulmonary involvement (8, 10–16). The prognosis of invasive disease caused by Conidiobolus spp. is poor, with 7 of the 10 invasive cases being fatal (1, 8, 12–15, 17), 3 of which were in children (10, 16, 17). The majority of these patients had some form of immunosuppression (1, 6, 8, 14–17), and five were patients in the United States (10, 13–17). There is no consensus for treatment, although a high level of in vitro azole resistance has been reported (18, 19). Treatment for both invasive and chronic rhinofacial diseases has included combinations of azoles, amphotericin B, trimethoprim-sulfamethoxazole, potassium iodide, terbinafine, hyperbaric oxygen, and surgical debridement, with varying success (6, 15, 20). Our patient was prescribed IV liposomal amphotericin B and trimethoprim-sulfamethoxazole, but due to progression of the oncological disease, the decision was made to proceed with comfort care, and the patient was thus transitioned to broad-spectrum oral azole.
Conidiobolus is found in the soil and water, and therefore the significance of Conidiobolus detection from plasma cell-free DNA mNGS was unclear, as potential laboratory contamination could not be ruled out. Recovery of the organism from the patient’s sputum sample collected 3 days later supported its significance as the cause of the patient’s pulmonary disease. Detection of cell-free DNA in the plasma may be representative of angioinvasion, but a tissue biopsy would be required to confirm this. Interestingly, this organism is not generally known to be angioinvasive (5, 21).
There are conflicting reports on the utility of plasma cell-free DNA mNGS to aid in the diagnosis of infections, including invasive fungal infections (22–24). In our institution, the test may be considered in patients where direct source specimens of infected tissue or viscera, such as BAL, are unattainable. In this case, the test was deemed appropriate for the patient as invasive fungal infection was highly suspected, and a BAL collection was deemed high risk. The speed of the test is noteworthy, as a result was provided within 2 days from specimen collection. It is important to also note that sputum culture was successful at recovering the pathogen within 2 days of incubation as well, highlighting that conventional, standard of care testing is often sufficient in many cases if appropriate, high-quality specimens can be collected.
Conclusions
Here we describe a rare case of invasive pulmonary disease caused by Conidiobolus species in an immunocompromised adolescent. A combination of traditional culture and molecular approaches aided in the diagnosis of this infection. Invasive disease caused by Conidiobolus is likely underestimated due to limitations in recovery by culture; treatment and outcome remain inconsistent.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wüppenhorst N, Lee M-K, Rappold E, Kayser G, Beckervordersandforth J, de With K, Serr A. 2010. Rhino-orbitocerebral zygomycosis caused by Conidiobolus incongruus in an immunocompromised patient in Germany. J Clin Microbiol 48:4322–4325. doi:10.1128/JCM.01188-1020861341 PMC 3020825 · doi ↗ · pubmed ↗
- 2Hibbett DS, Binder M, Bischoff JF, Blackwell M, Cannon PF, Eriksson OE, Huhndorf S, James T, Kirk PM, Lücking R, et al.. 2007. A higher-level phylogenetic classification of the Fungi. Mycol Res 111:509–547. doi:10.1016/j.mycres.2007.03.00417572334 · doi ↗ · pubmed ↗
- 3Shaikh N, Hussain KA, Petraitiene R, Schuetz AN, Walsh TJ. 2016. Entomophthoramycosis: a neglected tropical mycosis. Clin Microbiol Infect 22:688–694. doi:10.1016/j.cmi.2016.04.00527109491 · doi ↗ · pubmed ↗
- 4Vilela R, Mendoza L. 2018. Human pathogenic entomophthorales. Clin Microbiol Rev 31:e 00014-18. doi:10.1128/CMR.00014-1830158298 PMC 6148186 · doi ↗ · pubmed ↗
- 5Prabhu RM, Patel R. 2004. Mucormycosis and entomophthoramycosis: a review of the clinical manifestations, diagnosis and treatment. Clin Microbiol Infect 10:31–47. doi:10.1111/j.1470-9465.2004.00843.x 14748801 · doi ↗ · pubmed ↗
- 6Stavropoulou E, Coste AT, Beigelman-Aubry C, Letovanec I, Spertini O, Lovis A, Krueger T, Burger R, Bochud PY, Lamoth F. 2020. Conidiobolus pachyzygosporus invasive pulmonary infection in a patient with acute myeloid leukemia: case report and review of the literature. BMC Infect Dis 20:527. doi:10.1186/s 12879-020-05218-w 32698804 PMC 7374966 · doi ↗ · pubmed ↗
- 7Hernandez MJ, Landaeta W, Salazar BN, Vargas J, Rodriguez-Morales AJ. 2007. Subcutaneous zygomycosis due to Conidiobolus incongruus. Int J Infect Dis 11:468–470. doi:10.1016/j.ijid.2007.01.00117331786 · doi ↗ · pubmed ↗
- 8Kimura M, Yaguchi T, Sutton DA, Fothergill AW, Thompson EH, Wickes BL. 2011. Disseminated human conidiobolomycosis due to Conidiobolus lamprauges. J Clin Microbiol 49:752–756. doi:10.1128/JCM.01484-1021147951 PMC 3043483 · doi ↗ · pubmed ↗