Hyperammonemia syndrome due to Pluralibacter gergoviae bacteremia in an immunocompromised patient: case report
Rami Waked, Jonathan Huang, Lucy S. Witt, Eileen M. Burd

TL;DR
A rare bacterium, Pluralibacter gergoviae, caused severe ammonia buildup and brain issues in a lung transplant patient on ECMO, expanding known infection-related hyperammonemia.
Contribution
Expands the clinical understanding of infection-related hyperammonemia to include Pluralibacter gergoviae as a potential cause.
Findings
Pluralibacter gergoviae bacteremia was associated with severe hyperammonemia and encephalopathy in an immunocompromised lung transplant patient.
The isolate was confirmed to be urease positive, potentially contributing to ammonia production.
Successful treatment involved antimicrobial therapy and hyperammonemia management, leading to clinical improvement.
Abstract
Pluralibacter gergoviae is a rare, opportunistic, urease-producing gram-negative organism infrequently implicated in invasive infections. Reports in organ transplant or extracorporeal membrane oxygenation (ECMO) settings are exceedingly uncommon. This case is distinctive for describing P. gergoviae bacteremia potentially associated with severe hyperammonemia and encephalopathy in a lung transplant recipient on prolonged ECMO support, expanding the clinical spectrum of infection-related hyperammonemia beyond the traditionally recognized Ureaplasma and Mycoplasma species. A 32-year-old woman with cystic fibrosis underwent bilateral lung transplantation while on ECMO for refractory hypoxemic respiratory failure. Her post-operative course was complicated by multiorgan failure, Candida parapsilosis fungemia, and later, surgical site infection. During the fourth month of hospitalization, P.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
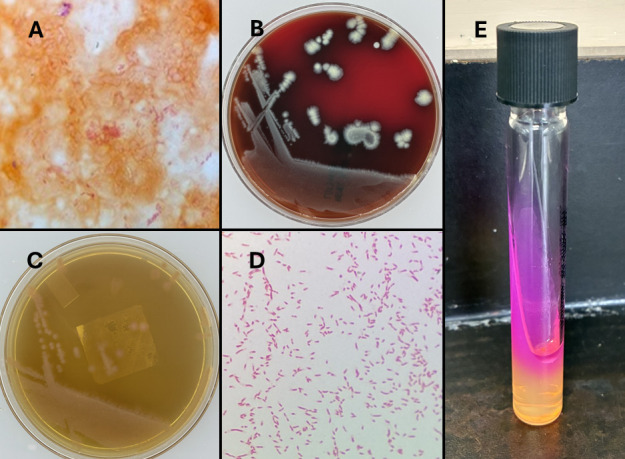 Fig 1
Fig 1| Antibiotic | MIC (μg/mL) | Interpretation |
|---|---|---|
| Cefazolin | ≥32.0 | Resistant |
| Cefepime | 2.0 | Susceptible |
| Cefpodoxime | ≥8.0 | Resistant |
| Ceftazidime | 4.0 | Susceptible |
| Ceftazidime + avibactam | 2.0 | Susceptible |
| Ceftriaxone | 0.5 | Susceptible |
| Ciprofloxacin | ≤0.06 | Susceptible |
| Ertapenem | ≤0.12 | Susceptible |
| Levofloxacin | ≤0.12 | Susceptible |
| Meropenem | ≤0.25 | Susceptible |
| Piperacillin + tazobactam | 16.0 | Susceptible-dose dependent |
| Tobramycin | ≤1.0 | Susceptible |
| Trimethoprim + sulfamethoxazole | ≤20.0 | Susceptible |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetabolism and Genetic Disorders · Infections and bacterial resistance · Antibiotic Resistance in Bacteria
INTRODUCTION
Pluralibacter gergoviae is a gram-negative, oxidase-negative, nitrate-positive, urease-positive, fermentative, rod-shaped organism belonging to the family Enterobacteriaceae (1, 2). Formerly classified as Enterobacter gergoviae due to its biochemical similarity to Enterobacter species, it has been reclassified into the genus Pluralibacter and is now designated as P. gergoviae (1). This organism has been identified as a contaminant in cosmetic products, as a colonizer of the human oral cavity, and as a cause of nosocomial outbreaks and bloodstream infections (3–8).
Hyperammonemia syndrome is a life-threatening complication in lung transplant recipients characterized by elevated serum ammonia and altered mentation. Mycoplasma and Ureaplasma infections are well-established contributors through ammonia overproduction (9–11). While not as common, the association of hyperammonemia syndrome with urease-producing Enterobacterales has been increasingly recognized (9, 12–16).
CASE PRESENTATION
A woman in her 30s with a history of cystic fibrosis complicated by chronic hypoxemic respiratory failure requiring home supplemental oxygen and pancreatic insufficiency was admitted to the hospital with acute hypoxemic respiratory failure necessitating endotracheal intubation upon arrival to the emergency department. Her medical history was notable for recurrent pulmonary infections with Pseudomonas aeruginosa and methicillin-resistant Staphylococcus aureus and chronic malnutrition requiring percutaneous gastrostomy tube placement.
Initial hospital course
A respiratory pathogen PCR panel (BIOFIRE Respiratory 2.1 Panel; bioMérieux, Durham, NC) was positive for respiratory syncytial virus and rhinovirus. Tracheal aspirate culture yielded methicillin-susceptible S. aureus, prompting the use of intravenous cefazolin 2 g every 8 hours, and inhaled tobramycin was continued for prior P. aeruginosa.
Despite targeted therapy, the patient remained profoundly hypoxemic and mechanical ventilator dependent. She was transitioned to veno-venous extracorporeal membrane oxygenation (ECMO) and eventually underwent an urgent off-pump bilateral orthotopic lung transplant around 6 weeks after admission. The patient was cytomegalovirus and Epstein–Barr virus seropositive. She was started on an immunosuppressive regimen with methylprednisolone, tacrolimus, and basiliximab. She also received atovaquone 1,500 mg once daily, inhaled amphotericin B, ganciclovir 5 mg/kg every 24 hours, and posaconazole 300 mg daily prophylaxis.
Post-operative course
The post-operative period was marked by significant complications. The patient developed low ECMO flow state necessitating conversion to central veno-arterial ECMO cannulation. Subsequently, she experienced intra-abdominal compartment syndrome with bowel ischemia, multiorgan failure, and an expanding retroperitoneal hematoma, which required lumbar artery embolization.
During this time, imaging demonstrated an evolving right lower lobe cavitary consolidation consistent with lung abscess, as well as a persistent right pleural air leak. Chest computed tomography revealed findings concerning for a bronchopleural fistula, for which the patient underwent operative intervention. Her course was further complicated by severe acute kidney injury requiring initiation of renal replacement therapy.
Late hospital course
At the fourth to fifth month of hospitalization, the patient remained on ECMO support. Her initial surgical wound became infected with cultures growing P. gergoviae, Candida parapsilosis, and vancomycin-resistant Enterococcus. Blood cultures obtained later grew P. gergoviae in one of two bottles after approximately 46 hours of incubation (Fig. 1A through D). Rapid identification using the BIOFIRE BCID2 PCR panel (bioMérieux) detected Enterobacterales, and species-level identification of P. gergoviae was achieved by matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry (confidence level 99.9%, bioMérieux). Antimicrobial susceptibility testing on the VITEK 2 system (bioMérieux) demonstrated resistance to cefpodoxime and cefazolin and dose-dependent susceptibility to piperacillin-tazobactam (see Table 1 for complete susceptibility results). This isolate was confirmed to be urease positive (Fig. 1E).
(A) Gram stain of positive blood culture showing gram-negative bacilli. (B and C) Pluralibacter gergoviae growth on blood agar and MacConkey agar, respectively, at 24 hours of incubation. (D) Gram stain from colonies on culture media showing gram-negative bacilli and some coccobacilli. (E) Positive urease test showing pink-red coloration change, indicating an alkaline change.
Hyperammonemia episode
Around the time of the P. gergoviae bacteremia, the patient developed acute encephalopathy. Laboratory evaluation revealed a markedly elevated plasma ammonia level of 262 µmol/L (reference range ≤53 µmol/L), consistent with hyperammonemia syndrome. At the time, she was receiving intravenous eravacycline 1 mg/kg every 12 hours, isavuconazole 372 mg daily, and meropenem 1g every 8 hours for her infections. There was no radiologic or clinical evidence of hepatic cirrhosis. Thyroid function tests demonstrated subclinical hypothyroidism. The neurocritical care service was consulted, and non-hepatic causes of hyperammonemia were considered, including infection-related hyperammonemia secondary to P. gergoviae bacteremia, medication-induced effects (tacrolimus), and nutritional factors. Molecular testing for Mollicutes (Mycoplasma and Ureaplasma) was performed using multiple modalities. Mycoplasma pneumoniae was assessed on the bronchoalveolar lavage (BAL) specimen using the in-house BIOFIRE FILMARRAY Pneumonia Panel (bioMérieux), which was negative. In addition, a Ureaplasma/Mycoplasma PCR was performed on the BAL at ARUP Laboratories (Salt Lake City, UT), and this also yielded negative results.
Therapeutic management included oral rifaximin 400 mg three times daily, lactulose two to three times daily, acetohydroxamic acid, and zinc supplementation, in addition to antibiotics. Serial monitoring showed gradual normalization of ammonia levels, accompanied by improvement in mental status and resolution of encephalopathy within 2 weeks from initiation of targeted antibiotic therapy. Repeat blood cultures in the subsequent days did not show any bacterial growth. Two weeks of antibiotic therapy were completed in total. Based on susceptibility results, meropenem was discontinued, and ceftriaxone 2g IV daily was initiated; however, due to subsequent hemodynamic instability, renally dosed meropenem was reintroduced. These adjustments reflect how antimicrobial agents (including dosage and selection) were modified in direct response to the P. gergoviae culture result and evolving clinical status.
DISCUSSION
P. gergoviae has been implicated as a causative pathogen in multiple clinical syndromes, including bacteremia (1–3), pulmonary infection (4, 5), urinary tract infection (4, 6), and endophthalmitis (7). In the present case, P. gergoviae was isolated from both surgical wound and bloodstream cultures in a lung transplant recipient. Distinguishing between colonization and true infection with this organism can be challenging, particularly in critically ill or immunocompromised hosts; however, the temporal association of positive cultures with clinical deterioration and compatible infectious findings in this patient supported its pathogenic role rather than colonization. The use of modern molecular diagnostic tools, including MALDI-TOF mass spectrometry and multiplex blood culture identification panel, was essential for the rapid and accurate identification of this uncommon Enterobacterales species. Infections caused by this organism have been most frequently described in transplant recipients (4, 6), patients with hematologic malignancies (3), and in neonatal outbreak settings (1, 2).
Hyperammonemia syndrome has been reported as a post-lung transplant complication, most often attributed to Ureaplasma or Mycoplasma species infections of the allograft (10). In a single-center study, the prevalence of hyperammonemia syndrome was 3.9% in lung transplant patients compared to 0.1% in other solid organ recipients (9). While this complication occurs with a mean onset of 11 days post-transplantation (11), hyperammonemia developed approximately 4 months after transplant in this recipient. Recognizing infection-associated hyperammonemia is crucial in critically ill and transplant patients, as early treatment of the infectious source and prompt metabolic management are key to preventing neurologic complications and improving outcomes.
In this case, P. gergoviae bacteremia was temporally associated with the onset of marked hyperammonemia and encephalopathy in the absence of hepatic dysfunction or mollicute detection, suggesting a possible contribution to the metabolic disturbance. However, molecular assays have imperfect sensitivity and do not uniformly detect all Ureaplasma and Mycoplasma species. Notably, the patient was receiving eravacycline at the time of testing, which has excellent activity against Mollicutes, further reducing the likelihood of an undetected mollicute infection. P. gergoviae is a urease-producing organism, confirmed by a positive urease test in this case (Fig. 1E) (8). The enzymatic breakdown of urea by urease generates ammonia and carbon dioxide as byproducts, leading to increased systemic ammonia levels. Additional contributing factors may include the use of immunosuppressive agents such as tacrolimus and cyclosporine, which have been shown to alter the expression of genes responsible for urea clearance (16, 17).
P. gergoviae demonstrates variable susceptibility to β-lactams, fluoroquinolones, aminoglycosides, and tetracycline derivatives (18). Reported resistance mechanisms include extended-spectrum β-lactamases and carbapenemases such as NDM, IMP, and KPC, underscoring the importance of antimicrobial susceptibility testing for definitive therapy (1, 3, 4, 6, 19). In this case, the isolate was susceptible (except for resistance to cefpodoxime and cefazolin), which supported de-escalation from empiric broad-spectrum coverage (meropenem) to a targeted regimen (ceftriaxone) guided by in vitro data.
Although reports of P. gergoviae infection in transplant or ECMO patients are rare, a few prior cases offer useful context. One similar case described colonization with P. gergoviae in a recent lung transplant recipient (4). In another case series, P. gergoviae outbreak was described among kidney transplant recipients (6). Separately, a case report of septic shock caused by KPC-producing E. gergoviae (i.e., prior nomenclature) in a neutropenic patient with leukemia illustrates the ability of the organism to cause fulminant invasive disease in immunocompromised hosts (3). Compared to these prior reports, our case is distinctive in several ways: it involves a lung transplant recipient on prolonged ECMO support, and the isolate was pan susceptible rather than carbapenemase harboring.
This case highlights P. gergoviae as an emerging opportunistic pathogen capable of causing invasive infection and possibly metabolic complications in profoundly immunocompromised hosts, including lung transplant recipients supported with ECMO. The temporal association between P. gergoviae bacteremia and marked hyperammonemia in the absence of hepatic dysfunction underscores the importance of recognizing infection-associated hyperammonemia, particularly with urease-producing organisms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Oliveira CTF, Saad BAA, Lacerda MLGG, Conte BS, de Oliveira SM do VL, Venturini J, Paniago AMM, de Miranda RV da SL, Valadão TB, da Costa LV, Souza GVD, Santos DR de S, Forsythe SJ, Volpe-Chaves CE, Brandão MLL. 2025. Bloodstream infections by multidrug-resistant Pluralibacter gergoviae in premature neonates in Central-West Brazil: report of two cases. Diagn Microbiol Infect Dis 112:116798. doi:10.1016/j.diagmicrobio.2025.11679840096800 · doi ↗ · pubmed ↗
- 2Ganeswire R, Thong KL, Puthucheary SD. 2003. Nosocomial outbreak of Enterobacter gergoviae bacteraemia in a neonatal intensive care unit. J Hosp Infect 53:292–296. doi:10.1053/jhin.2002.137112660126 · doi ↗ · pubmed ↗
- 3Satlin MJ, Jenkins SG, Chen L, Helfgott D, Feldman EJ, Kreiswirth BN, Schuetz AN. 2013. Septic shock caused by Klebsiella pneumoniae carbapenemase-producing Enterobacter gergoviae in a neutropenic patient with leukemia. J Clin Microbiol 51:2794–2796. doi:10.1128/JCM.00004-1323761145 PMC 3719649 · doi ↗ · pubmed ↗
- 4Weiss ZF, Hoffmann M, Seetharaman S, Taffner S, Allerd M, Luo Y, Pearson Z, Baker MA, Klompas M, Bry L, Pecora N. 2022. Nosocomial Pluralibacter gergoviae isolates expressing NDM and KPC carbapenemases characterized using whole-genome sequencing. Antimicrob Agents Chemother 66:e 0109322. doi:10.1128/aac.01093-2236121219 PMC 9578427 · doi ↗ · pubmed ↗
- 5Kesieme EB, Kesieme CN, Akpede GO, Okonta KE, Dongo AE, Gbolagade AM, Eluehike SU. 2012. Tension pneumatocele due to Enterobacter gergoviae pneumonia: a case report. Case Rep Med 2012:808630. doi:10.1155/2012/80863023056055 PMC 3466021 · doi ↗ · pubmed ↗
- 6Freire MP, de Oliveira Garcia D, Cury AP, Spadão F, Di Gioia TSR, Francisco GR, Bueno MFC, Tomaz M, de Paula FJ, de Faro LB, Piovesan AC, Rossi F, Levin AS, David Neto E, Nahas WC, Pierrotti LC. 2016. Outbreak of IMP-producing carbapenem-resistant Enterobacter gergoviae among kidney transplant recipients. J Antimicrob Chemother 71:2577–2585. doi:10.1093/jac/dkw 16527197663 · doi ↗ · pubmed ↗
- 7Chen KJ, Yang KJ, Sun CC, Yeung L. 2009. Traumatic endophthalmitis caused by Enterococcus raffinosus and Enterobacter gergoviae. J Med Microbiol 58:526–528. doi:10.1099/jmm.0.008482-019273651 · doi ↗ · pubmed ↗
- 8Davin-Regli A, Lavigne JP, Pagès JM. 2019. Enterobacter spp.: update on taxonomy, clinical aspects, and emerging antimicrobial resistance. Clin Microbiol Rev 32:00002–00019. doi:10.1128/CMR.00002-19PMC 675013231315895 · doi ↗ · pubmed ↗