Comorbidity profiles of non-tuberculous mycobacteria infections in China: 12 years’ experience
Chaohong Wang, Yiheng Shi, Bin Yang, Sibo Long, Weibing Lin, Dahong Su, Yan Zhao, Hao Li, Junhua Pan, Guirong Wang

TL;DR
NTM infections in Beijing are rising, linked to comorbidities like malnutrition and lung disease, with distinct patterns by species and gender.
Contribution
Identifies species-specific and gender-specific comorbidity profiles for NTM infections in China over 12 years.
Findings
NTM infections are strongly associated with malnutrition, bronchiectasis, and liver disease.
M. intracellulare is more linked to diabetes and malnutrition compared to M. abscessus.
NTM cases show stronger ties to lung damage and immunosuppression than tuberculosis.
Abstract
Nontuberculous mycobacteria (NTM) are of increasing public health concern. This study aimed to determine the most relevant comorbidities of NTM in Beijing, China, over a 12-year period. A retrospective analysis was performed on all 505 NTM patients diagnosed in Beijing Chest Hospital, Capital Medical University, from January 2010 to December 2021. Species identification, demographic characteristics, and comorbidities were analyzed using electronic medical records. The demographic characteristics and clinical comorbidity differences between NTM and tuberculosis (TB) patients were also analyzed. The number of patients infected with NTM in Beijing, China, has increased yearly. A total of 520 NTM were isolated from 505 inpatients, but only 465 were identified to the species level. M. intracellulare (43.44%, 202/465) and M. abscessus (128/465, 27.52%) predominated. NTM infection was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
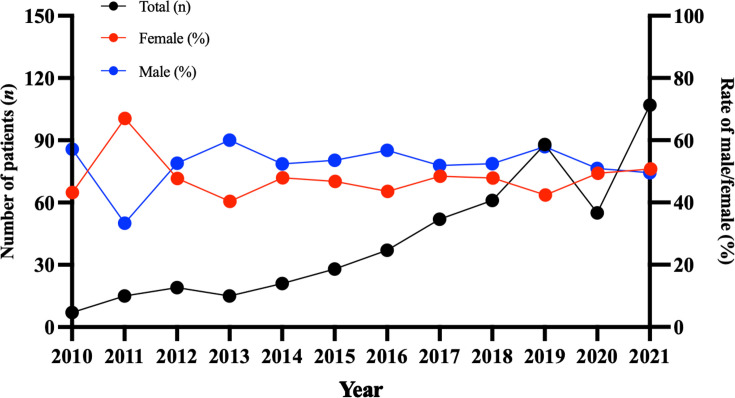 Fig 1
Fig 1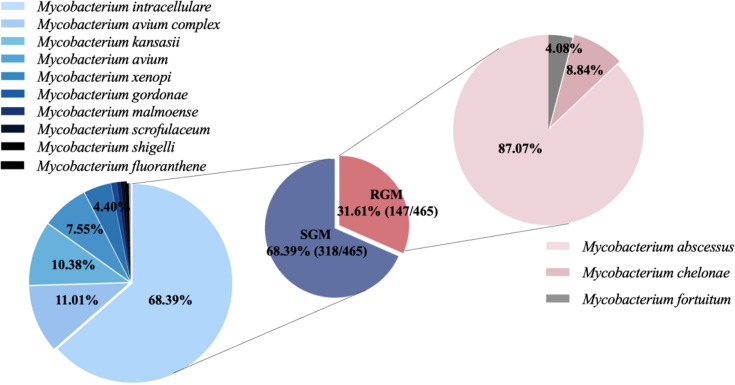 Fig 2
Fig 2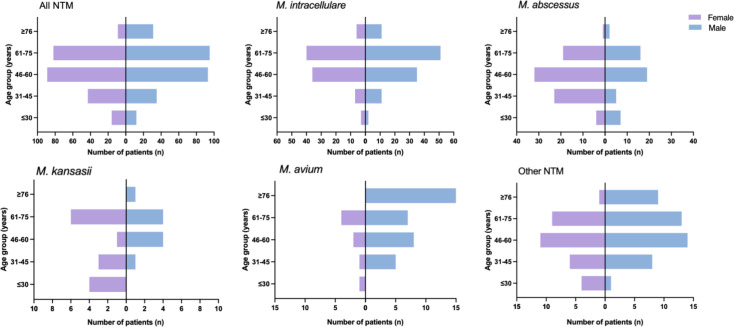 Fig 3
Fig 3| Specimen source | Sub-total, | Total, |
|---|---|---|
| Pulmonary | 506 (97.68) | |
| Sputum | 407 (78.57) | |
| BALF | 71 (13.73) | |
| Lung biopsy | 28 (5.41) | |
| Extra-pulmonary | 6 (1.16) | |
| Skin/soft tissue | 5 (0.97) | |
| Lymph node | 1 (0.19) | |
| Unknown | 6 (1.16) |
| NTM species | Sub-total, | Total, |
|---|---|---|
| Slowly Growing Mycobacteria | 318 (68.39) | |
| | 202 (43.44) | |
| | 35 (7.53) | |
| | 33 (7.10) | |
| | 24 (5.16) | |
| | 14 (3.01%) | |
| | 3 (0.65%) | |
| | 2 (0.43%) | |
| | 2 (0.43%) | |
| | 1 (0.22%) | |
| | 1 (0.22%) | |
| | 1 (0.22%) | |
| Rapidly Growing Mycobacteria | 147 (31.61) | |
| | 128 (27.52) | |
| | 13 (2.80) | |
| | 6 (1.29%) | |
| Total | 465 (100%) |
| Characteristics | |
|---|---|
| Age (years): median (IQR) | 59 (48.5–67) |
| Gender (male): | 266 (52.67%) |
| BMI (kg/m2): median (IQR) | 19.53 (17.28–21.97) |
| Previous history of PTB: | 118 (23.37%) |
| Co-morbidities: | 435 (86.14%) |
| Co-morbidities (pulmonary): | |
| Bronchiectasis | 126 (24.95%) |
| Pulmonary fungal infection | 54 (10.69%) |
| COPD | 33 (6.53%) |
| Silicosis | 9 (1.78%) |
| Pulmonary heart disease | 9 (1.78%) |
| Pneumoconiosis | 5 (0.99%) |
| Co-morbidities (non- pulmonary): | |
| Malnutrition | 217 (42.97%) |
| Liver disease | 157 (31.09%) |
| Diabetes mellitus | 63 (12.48%) |
| Hypertension | 58 (11.49%) |
| Coronary heart disease | 45 (8.91%) |
| Immunological disease | 45 (8.91%) |
| Malignancy | 21 (4.16%) |
| Kidney disease | 17 (3.37%) |
| Cerebrovascular disease | 14 (2.77%) |
| Nervous system diseases | 3 (0.59%) |
| Bronchiectasis | 48 (23.76) | 39 (30.47) | 4 (12.12) | 4 (16.67) | 5 (35.71) | 5 (38.46) |
| Pulmonary fungal infection | 28 (13.86) | 9 (7.03) | 1 (3.03) | 4 (16.67) | 3 (21.43) | 0 (0.00) |
| COPD | 15 (6.44) | 7 (5.47) | 4 (12.12) | 1 (4.17) | 2 (14.29) | 0 (0.00) |
| Silicosis | 5 (2.48) | 1 (0.78) | 0 (0.00) | 1 (4.17) | 0 (0.00) | 0 (0.00) |
| Pulmonary heart disease | 3 (1.49) | 1 (0.78) | 0 (0.00) | 1 (4.17) | 0 (0.00) | 0 (0.00) |
| Pneumoconiosis | 2 (1.00) | 0 (0.00) | 1 (3.03) | 1 (4.17) | 0 (0.00) | 0 (0.00) |
| Malnutrition | 102 (50.50)* | 43 (33.59)* | 17 (51.52) | 8 (33.33) | 8 (57.14) | 3 (23.08) |
| Liver disease | 70 (34.65) | 33 (25.78) | 16 (48.48) | 6 (25.00) | 7 (50.00) | 5 (38.46) |
| Diabetes mellitus | 30 (14.85)* | 6 (4.69)* | 6 (18.18) | 4 (16.67) | 3 (21.43) | 2 (15.38) |
| Hypertension | 22 (10.89) | 19 (14.84) | 2 (6.06) | 2 (8.33) | 2 (14.29) | 1 (7.69) |
| Coronary heart disease | 17 (8.42) | 4 (3.13) | 5 (15.15) | 2 (8.33) | 1 (7.14) | 1 (7.69) |
| Immunological disease | 21 (10.40) | 9 (7.03) | 1 (3.03) | 1 (4.17) | 3 (21.43) | 1 (7.69) |
| Malignancy | 8 (3.96) | 6 (4.69) | 1 (3.03) | 1 (4.17) | 0 (0.00) | 0 (0.00) |
| Kidney disease | 5 (2.48) | 6 (4.69) | 0 (0.00) | 3 (12.50) | 1 (7.14) | 0 (0.00) |
| Cerebrovascular disease | 4 (1.98) | 4 (3.13) | 3 (9.09) | 0 (0.00) | 1 (7.14) | 0 (0.00) |
| Nervous system diseases | 2 (1.00) | 1 (0.78) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) |
| NTM ( | TB ( | Z/χ2 | Effect size (95% CI) | ||
|---|---|---|---|---|---|
| Age (years): median (IQR) | 59 (48.5-67) | 48 (28-63) | −11.247 | <0.000 | 11 |
| Gender (male): | 266 (52.67%) | 18,619 (64.06%) | 27.876 | <0.000 | 0.62 (0.52–0.75) |
| Comorbidities: | |||||
| Bronchiectasis | 126 (24.95%) | 842 (2.91%) | 762.459 | <0.000 | 11.14 (8.93–13.83) |
| Pulmonary fungal infection | 54 (10.69%) | 625 (1.47%) | 161.471 | <0.000 | 5.45 (3.99–7.33) |
| COPD | 33 (6.53%) | 460 (1.59%) | 74.251 | <0.000 | 4.35 (2.92–6.28) |
| Silicosis | 9 (1.78%) | 182 (0.63%) | – | 0.006 | 2.88 (1.29–5.63) |
| Pulmonary heart disease | 9 (1.78%) | 145 (0.50%) | – | 0.001 | 3.62 (1.61–7.12) |
| Pneumoconiosis | 5 (0.99%) | 130 (0.45%) | – | 0.082 | 2.23 (0.71–5.36) |
| Malnutrition | 217 (42.97%) | 8,850 (29.56%) | 36.611 | <0.000 | 1.72 (1.43–2.06) |
| Liver disease | 157 (31.09%) | 8,789 (30.39%) | 0.170 | 0.680 | 1.04 (0.86–1.26) |
| Diabetes mellitus | 63 (12.48%) | 5,254 (18.17%) | 10.558 | 0.001 | 0.65 (0.49–0.84) |
| Hypertension | 58 (11.49%) | 4,320 (14.94%) | 4.489 | 0.034 | 0.74 (0.55–0.98) |
| Coronary heart disease | 45 (8.91%) | 1,719 (5.94%) | 7.947 | 0.005 | 1.56 (1.12–2.13) |
| Immunological disease | 45 (8.91%) | 599 (2.07%) | 109.331 | <0.000 | 4.65 (3.31–6.40) |
| Malignancy | 21 (4.16%) | 1,567 (5.42%) | 1.484 | 0.223 | 0.76 (0.47–1.18) |
| Kidney disease | 17 (3.37%) | 1,239 (4.28%) | 0.981 | 0.322 | 0.78 (0.45–1.27) |
| Cerebrovascular disease | 14 (2.77%) | 902 (3.12%) | 0.181 | 0.670 | 0.89 (0.48–1.52) |
| Nervous system diseases | 3 (0.59%) | 40 (0.14%) | – | 0.037 | 4.34 (0.86–13.69) |
- —Prevention and Control of Emerging and Major Infectious Diseases-National Science and Technology Major Project
- —Beijing Municipal Health and Health Technology Achievements and Appropriate Technology Promotion Project
- —Autonomous Region Science and Technology Support Program for Regional Innovation and Development
- —Beijing Tongzhou Municipal Science & Technology Commission
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Tuberculosis Research and Epidemiology · Medical Research and Treatments
INTRODUCTION
Nontuberculosis mycobacteria (NTM), a large group of mycobacteria distinct from Mycobacterium tuberculosis complex and Mycobacterium leprosy (1), are ubiquitous in natural environments such as soil and water (2, 3). Historically, NTM infections received little clinical attention because they are not transmitted from person to person and were often neglected as laboratory contamination (4, 5). However, the clinical significance of NTM has grown substantially, driven by advances in laboratory diagnostic technology, global population aging, and the increased population of immunocompromised hosts (6). Consequently, many recent reports concerned with morbidity and mortality of NTM have dramatically increased worldwide, particularly in countries with a high burden of tuberculosis (TB) (7), most of which are closely related to infectious diseases (8–10). Now recognized as one of the major emerging pathogens (11), NTM commonly causes pulmonary infections like Mycobacterium tuberculosis. The clinical symptoms and signs are often indistinguishable from those of TB, frequently leading to misdiagnosis as multidrug-resistant TB (12).
As a result, the diagnosis and treatment of NTM disease is challenging for clinicians (13). Host-pathogen interactions are pivotal in determining disease susceptibility, with factors such as age, sex, body mass index (BMI), and underlying comorbidities often affecting outcomes (14, 15).
In China, data on the demographic characteristics and clinical comorbidities of non-tuberculosis patients remain limited. A comprehensive analysis is especially needed for Beijing, the nation’s political and economic center. Hence, this retrospective study aimed to characterize the most relevant demographic characteristics and clinical comorbidities of NTM diseases in Beijing to provide a valuable reference for improving timely diagnosis and treatment.
MATERIALS AND METHODS
Species identification
The retrospective study included patients with NTM infections at Beijing Chest Hospital, Capital Medical University (Beijing, China), between January 2010 and December 2021 (a 12-year period). A total of 520 NTM specimens from 505 patients’ pulmonary and non-pulmonary sites were analyzed. The specimens obtained from ‘pulmonary sites’ included sputum, bronchial lavage fluid (BALF), and lung biopsy tissue. The ‘non-pulmonary’ site specimens included skin/soft tissue and lymph nodes. Direct smears were prepared from the above-separated specimens, stained with auramine, and observed by light-emitting diode microscopy.
After processing with NALC/NaOH and centrifugation, the supernatant of 500 μL was transferred into a 7 mL MGIT tube (Becton, Dickinson and Company, USA), and/or 100 μL was transferred onto LJ medium (Encode Medical Engineering Co., Ltd, China). LJ tubes were incubated at 37°C and examined weekly for growth for a maximum of 8 weeks, and MGIT tubes were cultured in the automated BACTEC MGIT 960 Mycobacteria culture system (BD), which usually reports positive results from two to four weeks and reports negative results after 42 days. All of the culture-positive isolates were primarily identified as M. tuberculosis complex (MTBC) by MPT64 antigen detection (Kaili Biotech kit, Hangzhou Innovation Biotech). Isolates that were initially identified as not MTBC by the MPT64 antigen testing were further identified to the species level using target DNA sequencing. We identified the isolates to species level by target DNA sequencing, including 16S rRNA, rpoB, hsp65, and the internal transcribed spacer region of the 16S-23S rRNA region (ITS) (16, 17). Genomic DNA was isolated from isolates by using the boiling method. There were 70 mycobacterial reference strains stored in the biobank in Beijing Chest Hospital (Beijing, China), which were obtained either from the American Type Culture Collection or the German Collection of Microorganisms. Multigene sequence similarity for the clinical isolates was determined in comparison with the reference sequences in our biobank or the multigene database using the basic local alignment search tool. Values above 99% sequence similarity for 16S rRNA and 97% similarity for hsp65, rpoB, and ITS genes were used for species distinction.
Data collection and statistical analysis
The demographic information and clinical data of the patients were collected by electronic medical record system. The American Thoracic Society/Infectious Disease Society of America criteria were used to define cases of pulmonary or extrapulmonary site (6). For each NTM patient, we analyzed their age, gender, BMI, lab examination results, and comorbidities. Categorical variables were expressed as counts (percentages). Differences in frequencies were compared using the χ^2^ test or Fisher’s exact test. Continuous variables were expressed as median with 25–75th interquartile range (IQR), and the difference was assessed using the Mann-Whitney U test. We considered that P < 0.05 means statistical significance. SPSS version 25.0 and GraphPad Prism version 9.4.1 were utilized to conduct these statistical analyzes.
RESULTS
Prevalence of NTM and species distribution
Among 29,834 mycobacterial cases from January 2010 to December 2021 in Beijing Chest Hospital, 520 clinical NTM strains were isolated from 505 patients, of which 465 strains were identified as specific species. The annual number of NTM infections increased 15-fold from 7 cases (2011) to 107 cases (2021) (Fig. 1).
Number of diseases infected by NTM during the 12-year period (2010–2021).
During the 12-year study period, 14 patients were simultaneously infected with two or more NTM. The specimen types and detected species were shown in [Tables 1 and 2](#T1 T2). Among all analyzed NTM isolates, respiratory specimens were predominant (506/518, 97.68%), including sputum samples (407/518, 78.57%), BALF (71/518, 13.73%), and lung biopsy tissue (28/518, 5.41%). 13 patients (2.57%) had two or more specimens with a positive result. The isolation rate of slowly growing mycobacteria (SGM) is higher than that of rapidly growing mycobacteria (Fig. 2), and the top three prevalent species were M. intracellulare (202, 43.44%), M. abscessus (128, 27.52%) and M. kansasii (33, 7.10%) (Table 2).
Frequency of species isolated from NTM patients during the study period.
Demographic data and laboratory testing of the study patients
According to the etiological results, 505 patients with NTM disease were included in this analysis. The median age of the cohort was 59 (48.5–67) with the majority of patients (71.09%, 359/505) aged between 46 and 75 years (Table 3 and Fig. 3). The cohort included 266 (52.67%, 266/505) male patients. At inclusion, most male and female patients had slim figures with a median BMI of 19.53 kg/m^2^ (17.28–21.97) (Table 3 and Fig. 3). By comparing the two groups with the highest isolation rate, 54.46% (110/202) of male patients were infected with M. intracellulare and only 38.28% (49/128) were infected with M. abscessus. From an age point of view, the most affected age category infected with M. intracellulare was 61–75 years old, while it was younger in patients infected with M. abscessus, mostly 46–60 years old.
Age and sex distribution of patients with NTM during the study period.
Simultaneously, we recorded the erythrocyte sedimentation rate () of inpatients infected with NTM, 60.15% (246/409) of them had higher values.
Comorbidities of NTM pulmonary disease
Among 505 NTM patients, 70 cases (13.86%) had no associated complications. Most patients had pre-existing lung disease or diseases related to nutritional deficiency. The most common comorbidity of NTM infection was malnutrition (217/505, 42.97%), liver disease (157/505, 31.09%), and bronchiectasis (126/505, 24.95%), followed by previous TB (118/505, 23.37%), diabetes mellitus (63/505, 12.48%), hypertension (58/505, 11.49%), and pulmonary fungal infection (54/505, 10.69%) (Table 3). In addition, we found that the incidence of bronchiectasis was higher in females (17.67%, 47/266 vs 33.05%, 79/239; χ^2^ = 15.914, P < 0.001), while Chronic Obstructive Pulmonary Disease (COPD) was found to be higher in males (9.77%, 26/266 vs 2.93%, 7/239; χ^2^ = 9.659, P = 0.002).
The comorbidities associated with the distribution of NTM species also vary. Patients with M. intracellulare were prone to malnutrition (102/202, 50.50%) and diabetes mellitus (30/202, 14.85%); on the contrary, patients with M. abscessus were more likely to be complicated with bronchiectasis (39/128, 30.47%) (Table 4).
Comparison analysis between NTM infections and TB
To further determine the risk factors for NTM disease, in addition to 505 patients with NTM infections, we also collected demographic characteristics and clinical comorbidities of 29,066 cases of TB, which were treated in our hospital in the same period. We noticed that there were statistically significant differences in age [59 (48.5–67) vs. 48 (28–63)], sex (1.11:1 vs. 1.78:1), and comorbidities (like bronchiectasis, pulmonary fungal infection, COPD, malnutrition, and immunological disease) between those infected with NTM and MTB (Table 5). The incidence of NTM was predominantly in the middle-aged and elderly, while TB is mainly in middle-aged males. Patients with NTM were worse in immunity and nutrition and were more likely to be complicated with lung diseases than patients with TB (Table 5). Hence, lung disease and immunocompromised status may play a vital part in the increased susceptibility to NTM infections.
DISCUSSION
In this study, the amount of NTM is increasing year by year, which is consistent with the current trend of annual NTM isolates reported worldwide (18). We evaluated the demographic characteristics, distribution of strains, and clinical relevance of all NTM inpatients treated at Beijing Chest Hospital, Capital Medical University, from January 2010 to December 2021. There were a variety of pathogens; 13 kinds of NTM species were detected in total from different types of specimens (mainly from pulmonary), 10 SGM, and 3 RGM. The SGM were more commonly isolated than RGM (68.39% vs 31.61%), among which M. intracellulare was the predominant species, accounting for 43.44% of total disease-causing NTM, followed by 27.52% M. abscessus. These data were similar to the reports that M. intracellulare was the most common NTM species in China (19, 20), whereas they were different from Southeast Asian countries such as Japan and South Korea (21–23).
Published case reports and series showed that the age range of those most affected by NTM was over 60 years old, a trend linked to an aging population (24). Furthermore, slender women were more susceptible to NTM infection (25, 26). In our study, we also found that NTM infection was associated with age, not gender. The incidence of NTM infection is high in patients aged 46–75 years, with a median age of 59 (48.5–67), and the prevalence of pulmonary NTM disease was similar in male and female patients. However, both male and female patients had slim figures with BMI close to the lower end of the normal range (19.53 (17.28–21.97), 19.13 (17.29–21.46) vs 19.82 (17.15–22.41)).
Studies have shown that pre-existing chronic pulmonary diseases are described as major predisposing factors for the development of pulmonary NTM infection; structural lung diseases predispose people to pulmonary NTM infection (7, 27). Previous history of PTB, bronchiectasis, and COPD is frequently associated with NTM, as well as diseases such as pneumoconiosis, silicosis, and cystic fibrosis (28, 29). Weak immune systems and nutritional deficiency are also included in the risk factor list for NTM disease (27). Among the NTM population in this study, 86.14% of the patients were complicated with different kinds of comorbidities. Malnutrition (217/505, 42.97%), liver disease (157/505, 31.09%), and bronchiectasis (126/505, 24.95%) were the main comorbidities of NTM infection, followed by previous TB (118/505, 23.37%), diabetes mellitus (63/505, 12.48%), hypertension (58/505, 11.49%), and pulmonary fungal infection. Unfortunately, we have rarely observed patients with cystic fibrosis, which may be related to race. In addition, we did find something special; the incidence of bronchiectasis was higher in females (17.67%, 47/266; 33.05%, 79/239; χ^2^ = 15.914, P < 0.001). In contrast, COPD was found higher in males (9.77%, 26/266; 2.93%, 7/239; χ^2^ = 9.659, P = 0.002). These distinct features were consistent with the findings observed in other studies (30, 31). Another interesting finding is that the comorbidities associated with the distribution of NTM species also vary. Patients with M. intracellulare were prone to malnutrition and diabetes mellitus; on the contrary, patients with M. abscessus were more likely to be complicated with bronchiectasis. Compared with tuberculosis, NTM disease and other basic diseases of the lung are much inextricably linked. NTM infection is more common in patients with bronchiectasis, pulmonary fungal infection, and COPD. A high prevalence of NTM is associated with a high burden of pulmonary basic disease such as bronchiectasis, likely explained by pulmonary damage, thus increasing the risk of acquiring NTM. However, it is not clear whether NTM is the cause or consequence of bronchiectasis. In the meantime, we also found that the nutritional status and immune ability of patients with NTM disease were lower. Some patients had Sjögren’s syndrome and rheumatoid arthritis. Our results suggest that patients suffering from malnutrition may have abnormal laboratory test results. We recorded 60.15% (246/409) of NTM disease patients had hypoproteinemia or anemia and higher ESR; the latter can also reflect that these patients had chronic inflammation.
This study has several limitations. Firstly, the study population was from a single tertiary hospital. Secondly, there may be an underestimation in the prevalence of NTM, due to all the enrolled cases being HIV-uninfected, while HIV infection was a risk factor for NTM-PD. Finally, our analysis was based exclusively on patients with culture-confirmed NTM. While this approach ensures diagnostic accuracy, it introduces a potential selection bias, as our cohort does not capture patients with clinically suspected disease whose cultures remained negative. Therefore, the comorbidity profile we describe should be interpreted as representative of the culture-positive NTM population, which may not reflect the entire spectrum of NTM infection.
Conclusion
Our work here underscores a fundamental point: NTM disease in our patients is intrinsically tied to specific underlying health conditions, setting it apart from tuberculosis. We found powerful links to bronchiectasis, COPD, and immunological diseases—associations so strong they should be considered defining features of the patient at risk. This isn't just an academic finding; it calls for a real shift in clinical practice. Instead of waiting for a classic presentation, clinicians should have a high index of suspicion for NTM in any patient with these comorbidities. For those with known bronchiectasis, in particular, proactive screening for NTM should be part of their routine care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ Jr, Andrejak C, Böttger EC, Brozek J, Griffith DE, Guglielmetti L, Huitt GA, Knight SL, Leitman P, Marras TK, Olivier KN, Santin M, Stout JE, Tortoli E, van Ingen J, Wagner D, Winthrop KL. 2020. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J 56:2000535. doi:10.1183/13993003.00535-202032636299 PMC 8375621 · doi ↗ · pubmed ↗
- 2Jeon D. 2019. Infection source and epidemiology of nontuberculous mycobacterial lung disease. Tuberc Respir Dis 82:94. doi:10.4046/trd.2018.0026 PMC 643593330302953 · doi ↗ · pubmed ↗
- 3Moriguchi S, Kita S, Yabuki Y, Inagaki R, Izumi H, Sasaki Y, Tagashira H, Horie K, Takeda J, Iwamoto T, Fukunaga K. 2018. Reduced Ca M kinase II and Ca M kinase IV activities underlie cognitive deficits in NCKX 2 heterozygous mice. Mol Neurobiol 55:3889–3900. doi:10.1007/s 12035-017-0596-128547530 · doi ↗ · pubmed ↗
- 4Stout JE, Koh W-J, Yew WW. 2016. Update on pulmonary disease due to non-tuberculous mycobacteria. Int J Infect Dis 45:123–134. doi:10.1016/j.ijid.2016.03.00626976549 · doi ↗ · pubmed ↗
- 5Hu C, Huang L, Cai M, Wang W, Shi X, Chen W. 2019. Characterization of non-tuberculous mycobacterial pulmonary disease in Nanjing district of China. BMC Infect Dis 19:764. doi:10.1186/s 12879-019-4412-631477038 PMC 6719376 · doi ↗ · pubmed ↗
- 6Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, Holland SM, Horsburgh R, Huitt G, Iademarco MF, Iseman M, Olivier K, Ruoss S, von Reyn CF, Wallace RJ, Winthrop K, ATS Mycobacterial Diseases Subcommittee, American Thoracic Society, Infectious Disease Society of America. 2007. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 175:367–416. doi:10.1164/rccm.200604-571ST 17277290 · doi ↗ · pubmed ↗
- 7Máiz L, Girón R, Olveira C, Vendrell M, Nieto R, Martínez-García MA. 2016. Prevalence and factors associated with nontuberculous mycobacteria in non-cystic fibrosis bronchiectasis: a multicenter observational study. BMC Infect Dis 16:437. doi:10.1186/s 12879-016-1774-x 27549788 PMC 4994165 · doi ↗ · pubmed ↗
- 8Nishiuchi Y, Iwamoto T, Maruyama F. 2017. Infection sources of a common non-tuberculous mycobacterial pathogen, Mycobacterium avium complex. Front Med (Lausanne) 4:27. doi:10.3389/fmed.2017.0002728326308 PMC 5339636 · doi ↗ · pubmed ↗