Bladder flap creation during cesarean delivery. A systematic review and meta-analysis of randomized controlled trials
Nour A El-Goly, Ahmed Mohamed Maged, Sally El-Attar, Nada Kamal

TL;DR
This study compares the outcomes of creating a bladder flap during cesarean delivery versus omitting it, finding that omitting it may reduce operative time and postoperative pain.
Contribution
The study provides a systematic review and meta-analysis of randomized trials to evaluate the risks and benefits of bladder flap creation during cesarean delivery.
Findings
Omission of bladder flap creation significantly shortens operative time and incision-to-delivery time.
Omission is associated with reduced microscopic hematuria and postoperative pain.
No significant difference in bladder injury or postoperative complications was found.
Abstract
The aim of the study is to compare the risks and benefits of bladder flap creation and omission during cesarean delivery. The databases search from inception to August 2025 included PubMed, Scopus, Embase, Web Of Science, Cochrane library, and clinicaltrials.gov registration using the keywords cesarean delivery AND bladder flap and their MesH terms yielded 13 studies with 3663 participants. All studies were evaluated through risk of bias assessment, and the quality of evidence was assessed through GRADE analysis. Microscopic hematuria was evaluated in 6 studies with 2738 participants and revealed an Odds Ratio (OR) of 3.23 with 1.10, 9.42 95% Confidence Interval (CI), P value = 0.04, I2 = 94%. Intraoperative blood loss was evaluated in 3 studies with 609 participants and revealed a mean difference (MD) of 46.75 with -123.50, 217.00 95% Confidence Interval (CI), P value =0.59, I2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
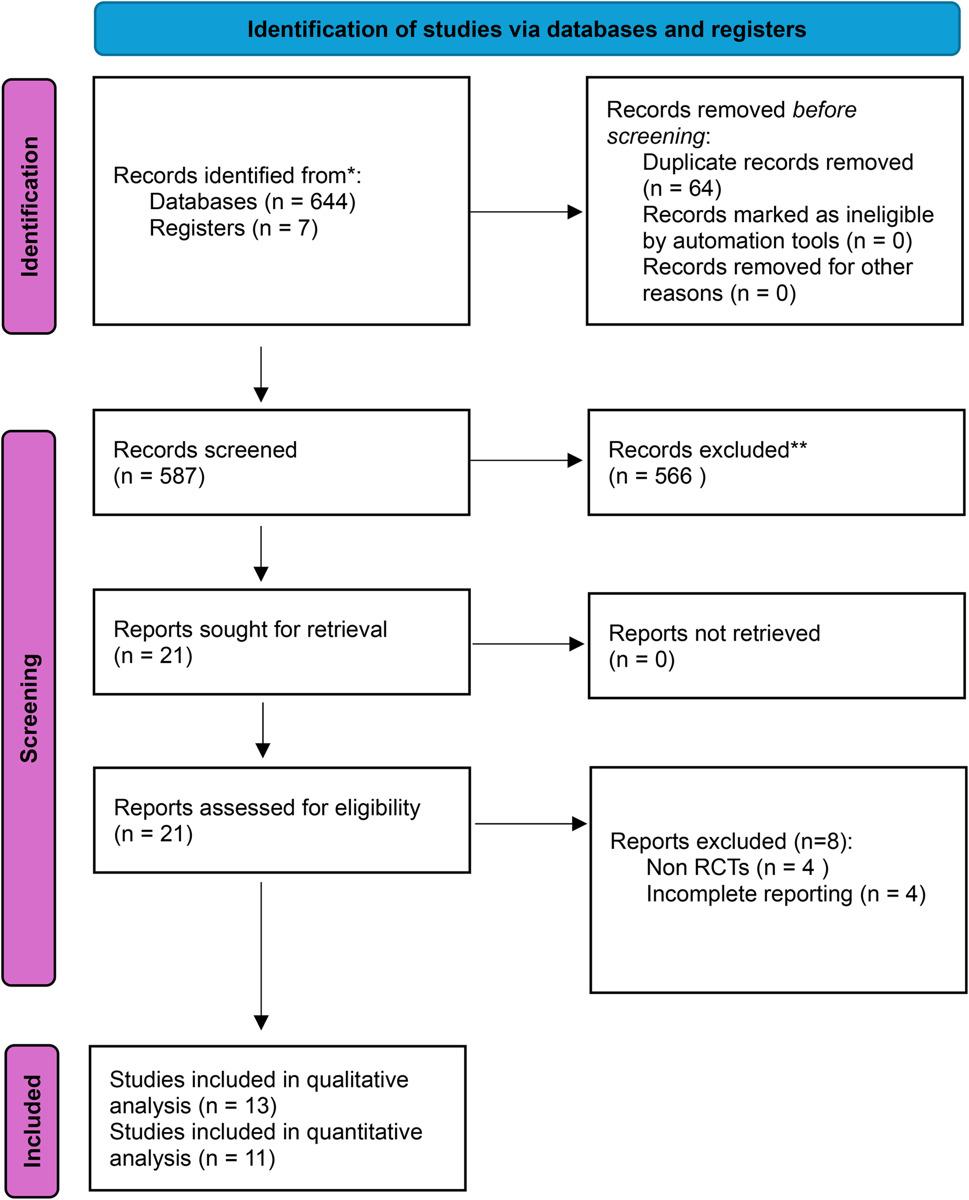 Figure 1
Figure 1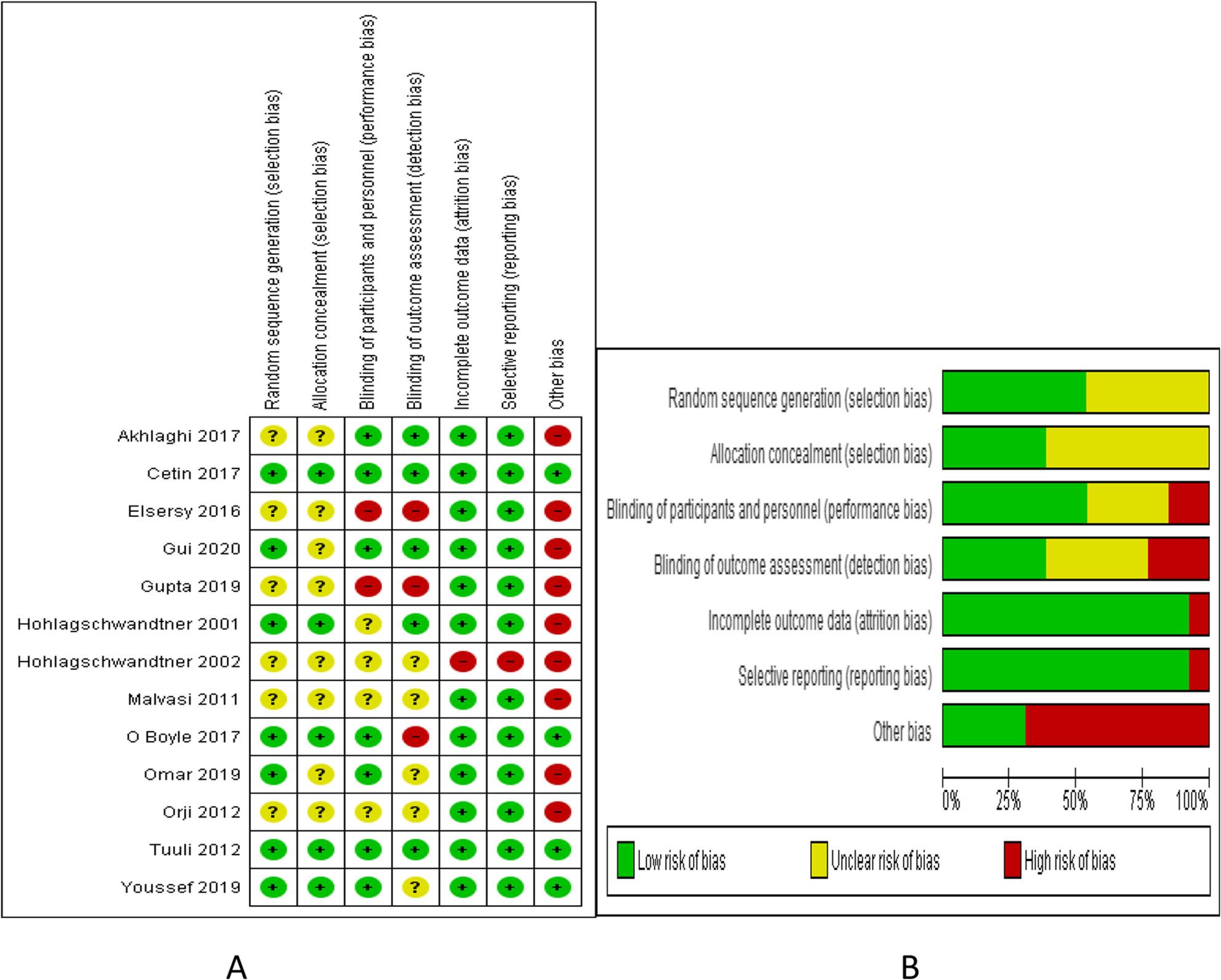 Figure 2
Figure 2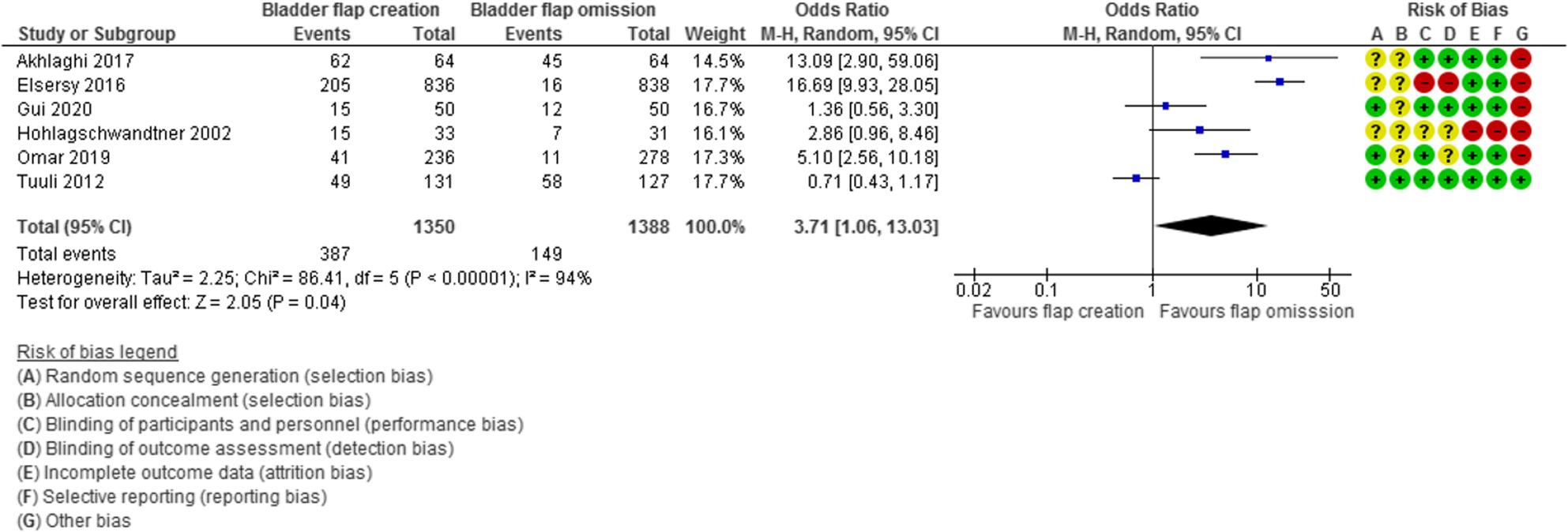 Figure 3
Figure 3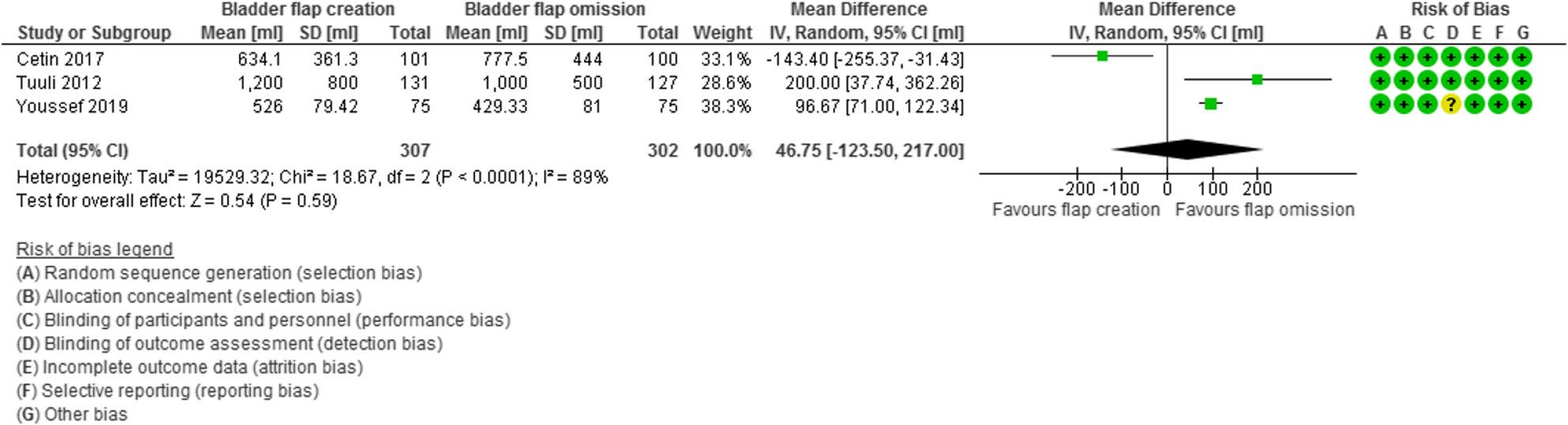 Figure 4
Figure 4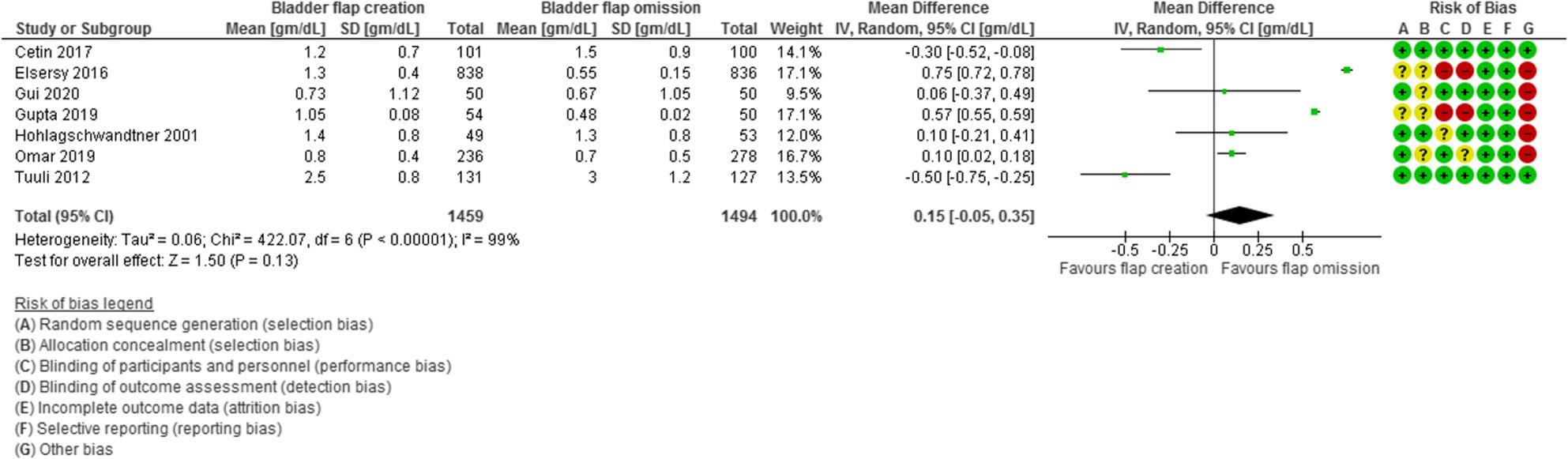 Figure 5
Figure 5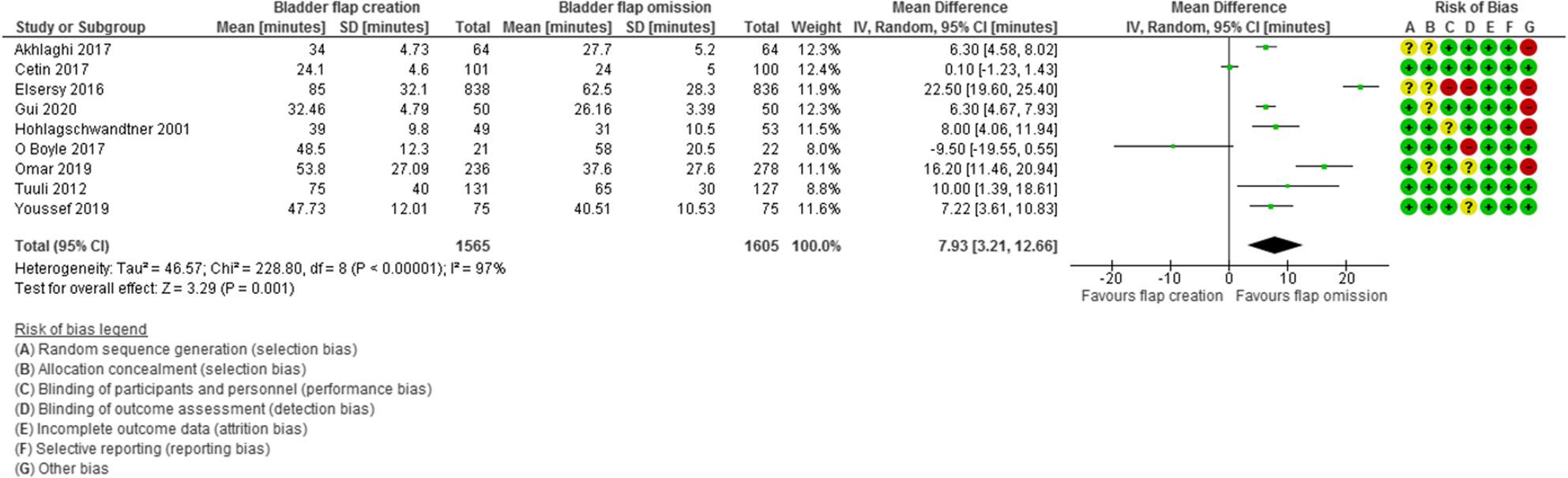 Figure 6
Figure 6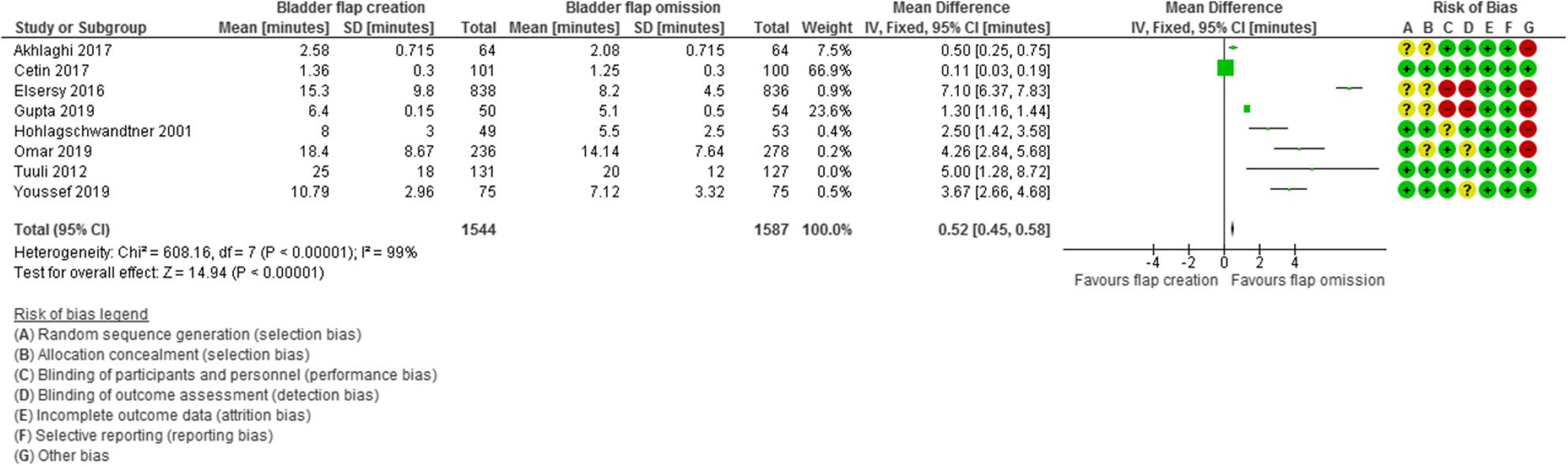 Figure 7
Figure 7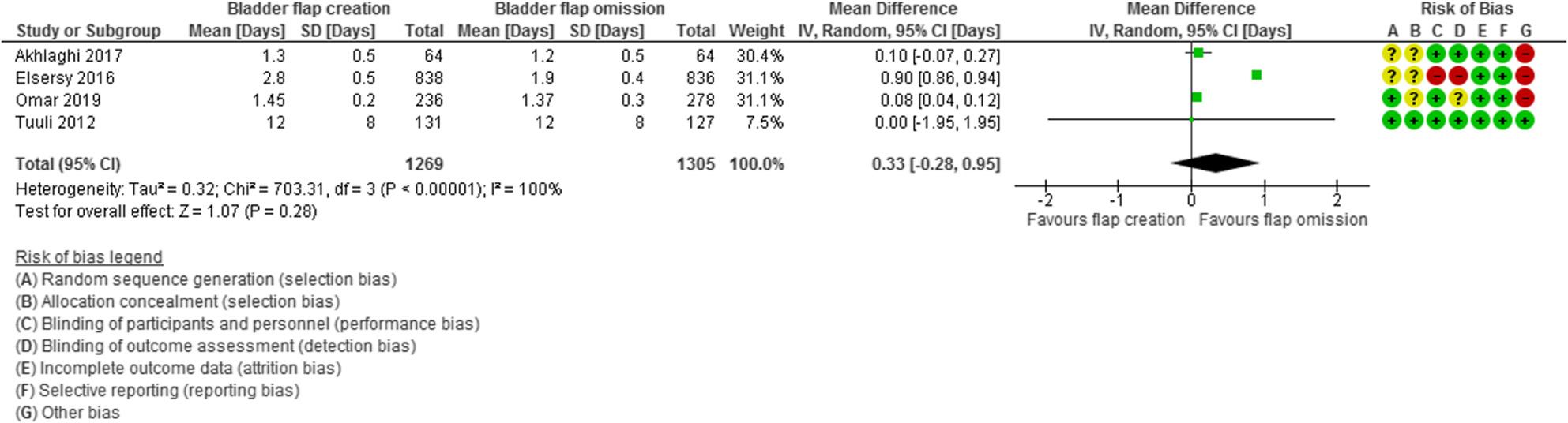 Figure 8
Figure 8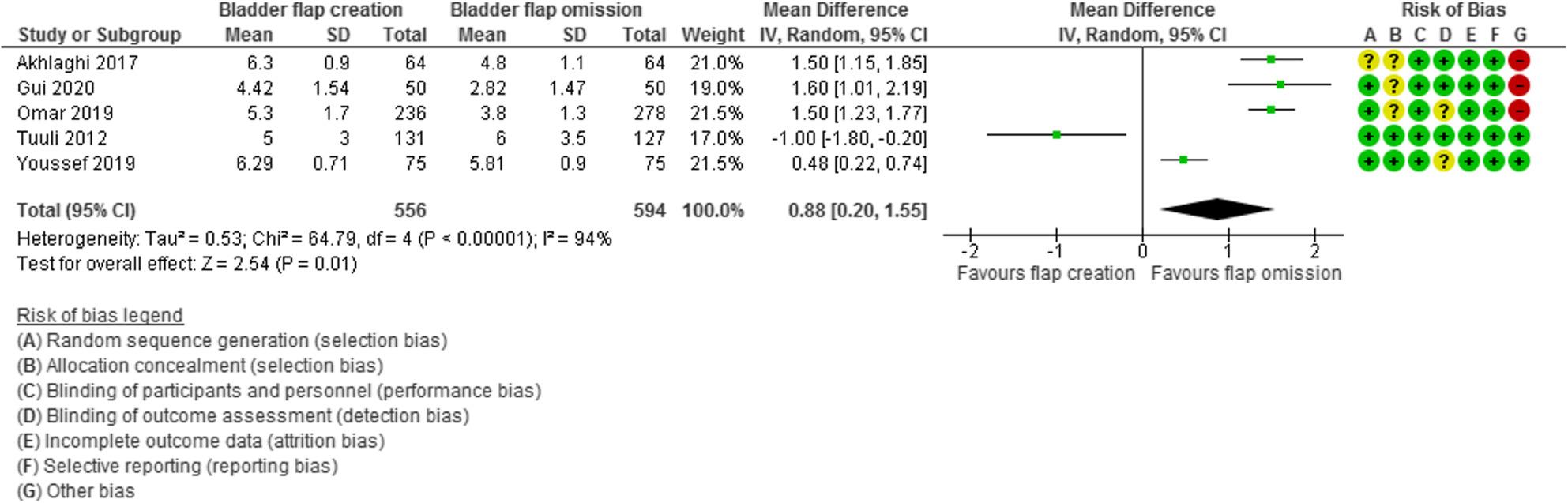 Figure 9
Figure 9- —Cairo University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and Perinatal Health Interventions · Ureteral procedures and complications · Pelvic floor disorders treatments
Introduction
Worldwide, the most commonly conducted surgery is Cesarean delivery (CD). Generally, the rate of CD is about 21% with large variation among different areas with less than 5% in Somalia and more than 50% in Egypt and Brazil. Although CD is associated with lower risk of maternal pelvic floor and fetal birth injuries, it carries a twofold increase in maternal and neonatal morbidity compared with vaginal delivery [1].
During the last years the technique of standard CD has undergone several suggestions to optimize the outcome and minimize costs and complications of the procedure. These suggestions include the need for urinary catheter insertion [2], uterine exteriorization versus insitu repair [3], closure of uterine incision in a single or double layers [4], technique of uterine incision closure [5], suturing or omitting peritoneal closure [6], suturing the subcutaneous tissue versus leaving a subcutaneous drain [1], and different techniques of skin closure [7].
Bladder flap creation defined as the dissection of the urinary bladder from the lower uterine segment was a standard step during CD. This aimed to protect the bladder from any inadvertent injury during the coming steps in the procedure [8].
In 1994, Pelosi and Ortega suggested omission of bladder flap creation with other surgical modifications to achieve simplicity, lower costs, and enhance recovery after CD [9].
After that several trials were conducted to compare the advantages and disadvantages of omission of bladder flap creation with conflicting results. The performance of routine formation of bladder flap varies among obstetricians and institutions. There is a lack of consensus in the existing literature about bladder flap creation, especially regarding long-term sequalae such as adhesion formation. A comprehensive and updated systematic review is therefore warranted to synthesize the current available evidence about the risks and benefits of omission of bladder creation during CD and its effects on maternal and surgery outcomes and establish a clear clinical guidance.
Objective
Comparing bladder flap creation and omission during cesarean delivery.
Methods
The PRISMA guidelines protocol were followed to prepare the protocol for this review. The protocol was registered at Prospero (CRD42022306980) on 25/2/2022.
Eligibility criteria, information sources, search strategy
The search included PubMed, Scopus, Embase, Web Of Science, Cochrane library, and clinicaltrials.gov registration till August 2025 and was conducted by two authors independently. The search keywords included cesarean delivery AND bladder flap and their MesH terms. Details about search strategy are shown in Supplementary table S1.
Study selection
Selection of the included studies was done following PICOS format designed for research question by 2 authors independently. Population were pregnant women who underwent CD whether primary or repeated one. Intervention was the creation of bladder flap before uterine incision. Comparator was omission of bladder flap creation and direct incision of the lower uterine segment. Outcomes included were the presence of microscopic hematuria, intraoperative blood loss, hemoglobin and hematocrit changes after the operation, total operative time, incision to delivery time, duration of hospital stay, postoperative pain score, and development of complications including bladder injury, urinary tract infection, and urine retention. Only randomized controlled studies with no language limitations were included in our review. Cohort, case control, case reports, case series, editorial opinions, letters to editor, review articles, and studies with incomplete data were excluded from our review.
We used a data extraction sheet that was prepared and approved by all authors. The sheet included names of authors, year of publication, study settings, participants characteristics, sample size, intervention details, and outcomes reported.
The studies included in our review were subjected to risk of bias assessment following the Cochrane Handbook recommendations for Systematic Reviews. Items for evaluation were random sequence generation, allocation concealment, blinding of participants and assessors of outcomes, incomplete data, selective data reporting and other biases [10].
The quality of evidence was evaluated using GRADE analysis which includes assessing the studies number, their risk of bias, inconsistencies reported among different studies, indirectness of data, number of participants, limits of confidence intervals and publication bias [11].
Statistical analysis
Dichotomous variables overall estimate was calculated using Odds Ratio (OR) and 95% confidence interval (CI) while and the mean differences and its corresponding 95% CI was used to calculate the effect estimates for continuous variables. OR greater than 1 indicates that the exposure or intervention is associated with higher odds of the outcome occurring compared with the reference or control group, suggesting a positive association between exposure and outcome. The magnitude of the OR reflects the strength of this association rather than causality.
The random and fixed effect models were used in case of high and insignificant heterogeneity, respectively. The level of significance for P value and I2 test for heterogeneity was set at 0.05 and 40%, respectively. Statistical analysis was done using the Review Manager (RevMan) version 5.4.1 (The Nordic Cochrane Centre, Cochrane Collaboration, 2020, Copenhagen, Denmark) [11].
Results
Study selection, study characteristics
Prisma flow chart of the study is described in Fig. 1.
Fig. 1. Prisma flow chart
Thirteen RCTs were included in our qualitative analysis [12–24] but Malvasi and colleagues’ study [19] was not included in quantitative analysis as it was focused on different outcome mainly postoperative adhesion formation and Orji et al. study [22] was excluded from the quantitative analysis as the exact numbers of randomized women could not be reached even after authors contacting.
The included studies were conducted on 3734 randomized participants (only 3663 were analyzed), 1704 of them had bladder flap creation while the other 1749 had bladder flap omission (in 201 women in Orji study, the number for each intervention was not clear). All the studies were conducted in a single center except Akhlaghi 2017 and Malvasi 2011 that were conducted in 2 and 3 centers, respectively. All studies were published in English except Hohlagschwandtner which was published in German. Three studies were conducted in Egypt, 2 in Austria, 2 in Turkey, 2 in USA, and one study was conducted in each of the following countries India, Iran, Italy, and Nigeria. All the studies were not registered except Cetin, O Boyle (retrospective registration), Tuuli, and Youssef. The CD was primary in 8 studies and a mix of primary and repeated CD in 5 studies.
The characteristics of the included studies are described in Table 1, and the risk of bias summary and graph is shown in Fig.2.
Table 1. Characteristics of the included studiesStudysettingsDesignSizeParticipantsInterventionOutcomeAkhlaghi 2017Two centers IranNot registered128Inclusion criteria:CD primaryGA ≥ 36 weeksExclusion criteria:Previous abdominal surgeryCD with full cervical dilatation or station zero or lower.Bladder flap formation (n = 64): created through the cutting surface of the visceral peritoneum to isolate the bladder from the lower uterine segment.Avoiding bladder flap formation (n = 64): to open the bladder flap, a layer of the peritoneum above the upper edge of the bladder and in the anterior part of the lower uterine segment was taken with forceps in the middle line and transected with the scalpel or scissors. The scissors were placed between the bladder – uterine serous and the lower segment myometrium, and pressed out from the center line, and then while the blades were alternately partially opened, it was withdrawn to isolate a strip up to 2 cm wide from the serous, then the incision was made.Time to fetal extractionTime of CDBladder injuryBlood lossHematocrite changesPostoperative painHematuriaPostoperative complicationsDuration of hospitalizationCetin 2017Single center TurkeyNCT0297787208 randomized201 analyzedInclusion criteria:PrimiparaGA > 37 weeksLow risk pregnancyExclusion criteria:Urinary tract infectionMultiple pregnancyEFW > 4000 gmPrevious abdominal surgeryAssociated comorbiditiesCervical dilatation > 4 cmBladder flap group (n = 101):, a bladder flap was created using a scalpel to make a small transverse midline incision in the vesicouterine peritoneal fold, then both index fingers were used to stretch it laterally and caudally to separate the bladder from the low uterine segment.Non-Bladder flap group (n = 100) a transverse incision was made 1 cm above the vesicouterine peritoneal fold, and a bladder flap was not created.Primary outcome Operative timeSecondary outcomes: Urinary symptoms Bladder injury Urine retention Postoperative residual urine volume.Elsersy 2016EgyptNot registered1674Inclusion criteria:Elective primary and repeat CDGA ≥ 32 weeks.Exclusion criteria:Planned vertical uterine incisionPrevious abdominal surgeriesSedation and inability to obtain consentGroup 1 (n = 838): No Bladder Dissection Group, Uterine incision made 1 cm above the vesicouterine reflection without incision and dissection of the bladder peritoneum.Group 2 Bladder Dissection Group (n = 836): Standard CD with incision and dissection of a bladder flap prior to uterine incision.Primary outcome:Total operating timeSecondary outcomes:Times of skin to delivery and to facial closureBlood loss,Hematuria, dysuria, urinary retentionFebrile morbidityHospital stay and readmissionWound infection, Neonatal outcomesGul 2020Single center TurkeyNot registered100Inclusion criteria:Age 20–40 yearsGA 37–42nd weeksPrimipara undergoing elective CDExclusion criteria:Chronic disease (diabetes, hypertension) Previous urinary tract infectionPrevious laparotomyEmergency cesarean section (abruptio placenta, fetal distress, etc.)Flap group (n = 50): A small transverse midline incision was made with a scalpel at the vesicouterine peritoneum, and the bladder peritoneum was bluntly separated from the uterus using both index fingers.Control group (n = 50): A bladder flap was not created; a transverse incision was made 1 cm above the peritoneal vesicouterine layer.Primary outcome:Changes in urinary symptoms UDI-6 scoresSecondary outcomes:Residual urineHemoglobin changesUrinary symptoms and infectionGupta 2019Single center IndiaNot registered104Inclusion criteria:Primipara or multipara with singleton pregnancy with GA≥34weeksMultiparous previous 1 CS with singleton pregnancy with GA≥34weeks.Exclusion criteria:Anomalous babyPrevious 2 or 3 CSStudy group (n = 54): a low uterine transverse incision was given about 1 to 2 cm above the vesicouterine peritoneal fold without dissection and formation of a bladder flap.Control group (n = 50): caesarean delivery was performed in the same way together with the formation of a bladder flap before the uterine incision.Total operating timeIncision-delivery timePre- and postoperative haemoglobin Urinary tract infectionBowel functionWound healingHospitalization daysReadmissions.Hohlagschwandtner 2001Single center AustriaNot registered102Inclusion criteria:White women undergoing CD and give their informed consent.Exclusion criteria:fetal malformationsPrevious uterine surgeryStudy group (n = 53): A low-transverse uterine incision was performed about 1 cm above the vesicouterine peritoneal fold, without dissection and formation of a bladder flap.Control group (n = 49): cesarean delivery was performed in the same way together with formation of a bladder flap before the uterine incisionTotal operating timeIncision-delivery timePre- and postoperative hemoglobin Pre- and postoperative urine test for bloodFebrile morbidity Postoperative need of analgesicsBowel function Wound healing Hospitalization daysReadmissions.Hohlagschwandtner 2002 GermanSingle center AustriaNot registered64Inclusion criteria:White women undergoing CD and give their informed consent.Exclusion criteria:fetal malformationsPrevious uterine surgeryStudy group (n = 31): A low-transverse uterine incision was performed about 1 cm above the vesicouterine peritoneal fold, without dissection and formation of a bladder flap.Control group (n = 33): cesarean delivery was performed in the same way together with formation of a bladder flap before the uterine incisionPrimary outcome:Hematoma formationSecondary outcomes:Total operating timeIncision-delivery timeHemoglobin dropMicrohematuriaFebrile morbidityReoperationMalvasi 20113 centers ItalyNot registered115Inclusion criteria:Primary CSGA > 38 weeksExclusion criteria:Previous gynaecological surgeryEmergency CDPROM for > 36 hInfections, anticoagulant therapy during pregnancy or deliveryPre-eclampsia, HELLP syndrome, placentae previae, other placental pathologiesEFW > 4500 gramGroup 1(n = 58): anatomical forceps were used to grasp the visceral peritoneum around the vesico-uterine peritoneal bladder flap. A scalpel was used to make a small transverse midline incision in the VP, and both index fingers were used to stretch it laterally in both directions for approximately 4 cm and caudally for 3 cm in order to separate the bladder from the LUS.Group 2 (n = 57): a transverse incision was made 1 cm above the vesico-uterine peritoneal fold. The direct transverse incision of the VP and, subsequently, the myometrium was performed without dissection of the bladder flap.Primary outcome:Severity of adhesions.Secondary outcomes:Intra-operative blood lossOperative time Bladder injuries, Postoperative urinary dysfunction Postoperative pelvic painO’Boyle 2017Single center USARetrospective registration NCT0296791370 randomized 43 analyzedInclusion criteria:Primary elective CD for uncomplicated pregnancy signed an informed consent.Exclusion criteria:Age < 18 yearsGA < 37 weeksPrevious pelvic surgery including cesarean delivery, any surgery involving the bladder, endometriosis, uterine leiomyomata, chronic pelvic pain, or a history of nephrolithiasis during the current pregnancy.CD after failed trial of operative vaginal delivery (forceps or vacuum extraction).omission of the bladder flap (n = 22) and bladder flap (n = 21)The primary outcome was urinary symptom scores using UDI-6 at the 6–8 week postpartumSecondary outcomes:Pelvic floor symptomscores changesSymptom bother responses.Omar 2019Single center EgyptNot registered550 randomized514 analyzedInclusion criteria:Primary or repeat elective CDGA ≥ 32 weeksExclusion criteria:Emergent CDPlanned vertical uterine incisionPrevious laparotomies besides CD.Bladder flap formation (n = 236): during CS created through taking a layer of the peritoneum above the upper edge of the bladder and in the anterior part of the lower uterine segment with forceps in the middle line and transected with the scalpel or scissors. Then the scissor placed between the bladder—uterine serous and the lower segment myometrium, and pressed out from the center line, and then while the blades were alternately partially opened, it was withdrawn to isolate a strip up to 2 cm wide from the serous, then the incision was madeNo bladder flap group (n = 278): a low-transverse uterine incision was made approximately 1 cm above the vesico-uterine peritoneal fold without dissection and formation of a bladder flap.Times of incision, delivery and total CD. Intra- and post-operative complications. Blood lossHematuriaPain scoreNeed for analgesicsHemoglobin changesHospital stayInfectionOrji 2012Single center NigeriaNot registered210Primary CDNo detailsintraoperative bladder injury, compare the duration of surgery, compare the occurrence of haematuria in the immediate postoperative period and assess post operative need for analgesicsTuuli 2012Single center USAProspective registeration NCT00918996259 randomized258 analyzedInclusion criteria:Primary or repeat CDGA ≥ 32 weeksExclusion criteria:Emergent CDPlanned vertical uterine incisionPrevious laparotomies besides CD.Bladder flap formation (n = 131): bladder flap was createdNo bladder flap group (n = 127): a low-transverse uterine incision was made approximately 1 cm above the vesico-uterine peritoneal fold without dissection and formation of a bladder flap.Times of incision, delivery and total CD. Intra- and post-operative complications.Youssef 2019Single center EgyptProspective registeration NCT03016273150Inclusion criteria:Primary or repeat CDGA ≥ 32 weeksAge 18–45 yearsExclusion criteria:Planned vertical uterine incision.Previous laparotomies.Patient refusing to participateBladder flap (n = 75): Dissection of the vesicouterine peritoneal fold to allow bladder retraction.Non bladder flap (n = 75): uterine incision made 1 cm above the vesico-uterine reflection without incision and dissection of the bladder peritoneumTimes of operation, incision, delivery, and skin closure.Intraoperative complications.Postoperative Morbidity and mortality Postoperative pain scoreNeed for blood transfusion, Bladder injury Microhematuria.
Fig. 2. Risk of bias A summary B graph
Synthesis of results
Microscopic hematuria was evaluated in 6 studies with 2738 participants (1350 subjected to bladder flap creation and 1388 subjected to bladder flap omission) and revealed an Odds Ratio (OR) of 3.23 with 1.10, 9.42 95% Confidence Interval (CI), P value = 0.04, I2 = 94% (Fig. 3).
Fig. 3. Microscopic hematuria
Intraoperative blood loss was evaluated in 3 studies with 609 participants (307 subjected to bladder flap creation and 302 subjected to bladder flap omission) and revealed a mean difference (MD) of 46.75 with − 123.50, 217.00 95% Confidence Interval (CI), P value = 0.59, I2 = 89% (Fig. 4).
Fig. 4. Intraoperative blood loss
Hemoglobin drop was evaluated in 7 studies with 2953 participants (1459 subjected to bladder flap creation and 1494 subjected to bladder flap omission) and revealed a MD of 0.15 with − 0.05, 0.35 95% Confidence Interval (CI), P value = 0.13, I2 = 99% (Fig. 5).
Fig. 5. Hemoglobin drop
Total operative time was evaluated in 9 studies with 3170 participants (1565 subjected to bladder flap creation and 1605 subjected to bladder flap omission) and revealed a MD of 7.93 min with 3.21, 12.66 95% Confidence Interval (CI), P value = 0.001, I2 = 97% (Fig. 6).
Fig. 6. Total operative time
Incision to delivery time was evaluated in 8 studies with 3131 participants (1544 subjected to bladder flap creation and 1587 subjected to bladder flap omission) and revealed a MD of 0.52 min with 0.45, 0.58 95% Confidence Interval (CI), P value < 0.001, I2 = 99% (Fig. 7).
Fig. 7. Incision to delivery time
Duration of hospitalization was evaluated in 4 studies with 2574 participants (1269 subjected to bladder flap creation and 1305 subjected to bladder flap omission) and revealed a MD of 0.33 days with − 0.28, 0.95 95% Confidence Interval (CI), P value = 0.28, I2 = 100% (Fig. 8).
Fig. 8. Duration of hospitalization
Pain VAS score was evaluated in 5 studies with 1150 participants (556 subjected to bladder flap creation and 594 subjected to bladder flap omission) and revealed a MD of 0.88 with 0.20, 1.55 95% Confidence Interval (CI), P value = 0.01, I2 = 94% (Fig. 9).
Fig. 9. Pain score
The risk of bladder injury was evaluated in 5 studies with 1188 participants (576 subjected to bladder flap creation and 612 subjected to bladder flap omission) and revealed an OR of 2.11 with 0.48, 9.20 95% CI, P value = 0.32, I2 = 0%.
Urinary tract infection was evaluated in 3 studies with 876 participants (417 subjected to bladder flap creation and 459 subjected to bladder flap omission) and revealed an OR of 2.20 with 0.53, 9.13 95% CI, P value = 0.28, I2 = 52%.
Time to first defecation was evaluated in 3 studies with 356 participants (174 subjected to bladder flap creation and 182 subjected to bladder flap omission) and revealed a MD of 0.46 days with 0.02, 0.91 95% Confidence Interval (CI), P value = 0.04, I2 = 99%.
Urine retention was evaluated in 2 studies with 316 participants (159 subjected to bladder flap creation and 157 subjected to bladder flap omission) and revealed an OR of 1.25 with 0.18, 8.43 95% CI, P value = 0.82, I2 = 24%.
Postoperative complications were evaluated in 4 studies with 1101 participants (532 subjected to bladder flap creation and 569 subjected to bladder flap omission) and revealed an OR of 1.44 with 0.55, 3.75 95% CI, P value = 0.46, I2 = 0%.
GRADE quality of evidence is shown in Table 2 and subgroup analysis are described in Table 3.
Table 2GRADE quality of evidenceOutcomeNo studiesRisk of biasInconsistencyIndirectnessImprecisionPublication biasQualitySample sizeWide CIMicroscopic hematuria6NNN2738NNAHighIntraoperative blood loss3NSN609SNALowHemoglobin changes7NSN2953SNALowOperative time9NNN3170NNAHighIncision to delivery time8NNN3131NNAHighDuration of hospitalization4NNN2574NNAModeratePain score5NSN1150SNALowBladder injury5NNN1188SNAModerateUrinary tract infection3NNN876SNALowTime to 1st defecation3NNN356NNAModerateUrine retention2NNN316SNALowPostoperative complications4NNN1101SNALowN not serious, NA Not applicable, S serious
Table 3. Subgroup analysis of outcomesOutcomeSubgroupStudiesParticipantsEffect EstimateP valueI2Microscopic hematuriaPrimary CD56122.28 [0.80, 6.45]0.1283%Repeated CD24522.85 [0.32, 25.68]0.3589%Primary and repeated CD1167416.69 [9.93, 28.05]< 0.001NATotal627383.23 [1.10, 9.42]0.0494%Blood lossPrimary CD2329-36.96 [-273.60, 199.69]0.7676%Repeated CD1230250.00 [47.70, 452.30]0.02NAPrimary and repeated CD115096.67 [71.00, 122.34]< 0.001NATotal360946.75 [-123.50, 217]0.5989%Hemoglobin dropPrimary CD5723-0.04 [-0.18, 0.10]0.5445%Repeated CD2452-0.36 [-1.19, 0.48]0.494%Primary and repeated CD217780.66 [0.48, 0.84]< 0.00199%Total729530.15[-0.05,0.35]0.1399%Operative timePrimary CD77665.67 [2.11, 9.22]0.00292%Repeated CD258017.29 [3.79, 30.79]0.0185%Primary and repeated CD2182414.90 [-0.07, 29.87]0.0598%Total931707.93 [3.21,12.66]0.00197%Incision to delivery timePrimary CD57510.18 [0.10, 0.26]< 0.00195%Repeated CD24525.81 [4.48, 7.15]< 0.0010%Primary and repeated CD319281.54 [1.41, 1.68]< 0.00199%Total831310.52 [0.45,0.58]< 0.00199%Duration of hospitalizationPrimary CD34480.19 [0.12, 0.25]< 0.0010%Repeated CD24520.30 [0.22, 0.38]< 0.0010%Primary and repeated CD116740.90 [0.86, 0.94]< 0.001NATotal425740.33 [-0.28,0.95]0.28100%Pain scorePrimary CD45480.96 [0.27, 1.65]0.00685%Repeated CD2452-0.04 [-1.74, 1.67]0.9789%Primary and repeated CD11500.48 [0.22, 0.74]< 0.001NATotal511500.88 [0.20,1.55]0.0194%Blabber injuryPrimary CD57361.99 [0.29, 13.77]0.4821%Repeated CD24523.83 [0.15, 94.65]0.41NAPrimary and repeated CD00NANANATotal511882.11 [0.48,9.2]0.320%UTIPrimary CD23201.44 [0.21, 9.93]0.7128%Repeated CD24521.55 [0.63, 3.83]0.340%Primary and repeated CD110411.63 [1.42, 95.56]0.02NATotal38762.20 [0.53,9.13]0.2852%CD Cesarean delivery, CI Confidence Interval
Orji and colleagues [22] in their RCT compared the omission of bladder flap against its creation during CD in 210 women. They reported a significant reduction in blood loss (1.9% vs. 11.4%) [p = 0.026], duration of operation (43 ± 4.1 min vs. 47 ± 4.7 min) [p = 0.001], incision to delivery time (4.6 ± 0.9 min vs. 6.3 ± 1.2 min) [p = 0.001], postoperative pain score, needed doses for analgesics [p = 0.001], postoperative microscopic hematuria (20% vs. 71.4%) in women with omission of bladder flap compared to those with its creation, respectively. They found no significant differences between both groups regarding post-operative febrile morbidity and wound infection with no reporting of any bladder injury.
Malvasi and colleagues evaluated the value of bladder flap creation on the cesarean scar integrity. Their randomized 115 women undergoing primary CD to either bladder flap creation (58 women) or omission of bladder flap (57 women) and reevaluated them during their second CD. During the repeated CD they took 4 specimens from the scar and examined it by light and electron microscopy. They found higher rates of adhesions in bladder flap formation group compared to omission group (28 (48.3%) (20 mild and 8 severe) vs. 14 (24.1%) (8 mild and 6 severe), respectively). They also found higher rates of submesothelial fibrosis (39.6% vs. 12.2%, p < 0.01) and mesothelial stroma neovascularization (46.5%vs 21%, p < 0.01), and inflammatory cells (29.7 ± 1.3 vs. 18.3 ± 1.9, P < 0.01) in bladder flap creation versus omission, respectively. They concluded that creation of bladder flap is associated with inflammatory, regenerative, and fibrotic processes that can be reduced if bladder flap creation was omitted.
Exclusion of studies at high risk of bias yielded comparable effect estimates, supporting the robustness of the primary analysis (Table 4).
Table 4. Sensitivity analysis of outcomes after exclusion of high risk studiesOutcomeStudiesParticipantsEffect EstimateP valueI2Miscroscopic hematuria410000.1490%Intraoperative blood loss [ml]360946.75 [-123.50, 217.00]0.5989%Hemoglobin drop [gm/dL]51175-0.11 [-0.38, 0.15]0.4086%Hematocrite changes3271-0.95 [-2.58, 0.69]0.2674%Operative time [minutes]814966.12 [2.68, 9.57]< 0.00192%Incision to delivery time [minutes]613530.20 [0.12, 0.28]< 0.00195%Duration of hospitalization [Days]39000.08 [0.04, 0.12]< 0.0010%Pain score511500.88 [0.20, 1.55]0.0194%Complications411011.44 [0.55, 3.75]0.460%Bladder injury410735.27 [0.59, 46.93]0.140%Urine retention12015.05 [0.24, 106.53]0.30NAUrinary tract infection27721.55 [0.66, 3.63]0.325%Time of first defecation22520.48 [-0.50, 1.46]0.3396%
Discussion
This systematic review and meta-analysis provide a comprehensive and quantitatively robust synthesis of the available evidence comparing bladder flap creation versus omission during cesarean delivery (CD). The findings consistently suggest that routine bladder flap creation confers no meaningful perioperative benefit and may, in fact, be associated with increased operative morbidity, longer operative metrics, and heightened postoperative discomfort.
This meta-analysis found a highly significant shortening of the operative time (high evidence) and incision to delivery time (high evidence) and a significant reduction in microscopic hematuria (low evidence), postoperative pain score (low evidence) and time to 1st defecation (moderate evidence) and a non-significant differences in intraoperative blood loss (low evidence), postoperative hemoglobin changes (low evidence), duration of hospitalization (moderate evidence), risk of bladder injury (moderate evidence), urinary tract infection (low evidence), postoperative urine retention (low evidence) and postoperative complications (low evidence) in women who underwent omission of bladder flap creation compared to those who had creation of bladder flap.
The most clinically salient finding is the significantly increased odds of postoperative microscopic hematuria associated with bladder flap creation. Across six studies encompassing more than 2,700 participants, bladder flap creation was associated with more than a threefold increase in microscopic hematuria compared with omission. Although the confidence interval was wide and heterogeneity was substantial, the directionality of effect was consistent across studies. This observation plausibly reflects increased bladder manipulation and devascularization during flap dissection, leading to mucosal microtrauma or transient ischemia. Importantly, microscopic hematuria, while often self-limited, may represent a surrogate marker of subclinical bladder injury and tissue stress, particularly relevant in high-volume obstetric practice.
In contrast, no significant differences were observed between the two techniques with respect to intraoperative blood loss or hemoglobin drop. These null findings, despite large pooled sample sizes, suggest that bladder flap creation does not meaningfully contribute to hemostatic control during CD. However, the very high statistical heterogeneity (I² > 85% for both outcomes) indicates considerable variability in measurement methods, surgical technique, patient populations, and perioperative protocols. Consequently, these estimates should be interpreted with caution, and the absence of statistical significance should not be conflated with definitive equivalence.
Operative efficiency outcomes strongly favored omission of the bladder flap. Total operative time was significantly prolonged by nearly eight minutes when a bladder flap was created, with a similarly consistent and clinically relevant increase in incision-to-delivery time. Even modest delays in incision-to-delivery interval may carry implications for neonatal outcomes in compromised fetuses and are particularly pertinent in emergency CD settings. The finding of prolonged operative metrics aligns closely with the randomized controlled trial by Orji et al., which demonstrated significant reductions in operative time and incision-to-delivery interval when bladder flap creation was omitted. These data collectively challenge the historical rationale for bladder flap creation as a protective or efficiency-enhancing maneuver.
Postoperative pain outcomes further reinforce the lack of benefit of bladder flap creation. Women undergoing flap creation reported significantly higher pain scores, an effect that is both statistically and clinically relevant. Increased pain likely reflects additional tissue dissection, inflammation, and nerve irritation at the vesicouterine interface. This finding is concordant with Orji et al., who also reported increased analgesic requirements in the bladder flap group. Given current emphasis on enhanced recovery after cesarean delivery, minimizing avoidable sources of postoperative pain is a critical consideration.
Notably, bladder flap creation did not significantly reduce the risk of bladder injury, urinary tract infection, urinary retention, or overall postoperative complications. The absence of a protective effect against bladder injury is particularly important, as avoidance of bladder injury is often cited as the primary justification for bladder flap creation. The pooled estimate showed no statistically significant difference, with low heterogeneity, suggesting that omission of the bladder flap does not compromise surgical safety in this regard. This finding aligns with contemporary surgical principles emphasizing sharp, well-visualized dissection rather than routine prophylactic maneuvers lacking empirical support.
Gastrointestinal recovery, as measured by time to first defecation, was modestly but significantly delayed in the bladder flap creation group. Although the absolute difference was small, it is directionally consistent with increased surgical manipulation and inflammatory response. Duration of hospitalization did not differ significantly between groups; however, this outcome exhibited extreme heterogeneity, likely reflecting institutional policies and non-clinical determinants of discharge rather than true differences in recovery.
Beyond short-term outcomes, the histopathological evidence provided by Malvasi et al. offers compelling mechanistic insight into the potential long-term consequences of bladder flap creation. Their demonstration of increased adhesions, submesothelial fibrosis, neovascularization, and inflammatory cell infiltration in women undergoing bladder flap creation provides biological plausibility for the observed clinical findings. These chronic inflammatory and fibrotic changes may predispose to more difficult repeat cesarean deliveries, increased adhesion-related morbidity, and longer-term pelvic complications. The convergence of histological, clinical, and operative data strengthens the argument against routine bladder flap creation.
There is no available evidence about the use in emergency CD as most of the included studies omitted inclusion of these women, few studies included both elective and emergency CD but the effect on this particular group was not specified. The exclusion of emergency CD in most studies is related to difficulties in randomization properly in the emergency situation.
According to these findings, creation of bladder flap is probably not a necessary step during routine CD. This step can cause unnecessary prolongation of the incision to delivery and total operative time. This prolongation carries a high risk for adverse maternal and neonatal outcomes especially in cases of emergency CD conducted for fetal or maternal distress.
Strengths and limitations
This is the first comprehensive systematic review to compare the safety and efficacy of bladder flap creation and omission. All the currently available RCTs were included after extensive search efforts. All included studies were subjected to complete data extraction including the risk of bias and all possible outcomes. All outcomes were evaluated for quality of evidence using GRADE analysis. The distribution of studies among different countries including developing and developed countries is another strength of this review.
Several plausible factors may explain this marked heterogeneity. First, substantial clinical heterogeneity exists among the included studies. Variations in patient characteristics—such as parity, number of prior cesarean deliveries, indication for cesarean delivery (elective versus emergency), labor status, degree of bladder descent, and presence of adhesions—are likely to influence operative difficulty, bladder manipulation, and postoperative recovery, thereby affecting outcomes such as operative time, blood loss, pain scores, and urinary symptoms. Importantly, few studies are stratified or adjusted for these key baseline variables.
Second, technical heterogeneity in surgical practice is a major contributor. Bladder flap creation is not a standardized maneuver; its extent, plane of dissection, use of sharp versus blunt techniques, and degree of bladder mobilization varied considerably and were often poorly described. Similarly, comparator intervention may have ranged from minimal bladder handling to partial mobilization in anticipation of uterine incision. Differences in surgeon experience, training background, and institutional cesarean protocols further amplify this variability.
Third, methodological heterogeneity likely played a significant role. Included studies risk of bias, sample size, and outcome ascertainment. Several outcomes were measured using non-uniform definitions and assessment tools; for example, microscopic hematuria was variably defined and inconsistently timed postoperatively, pain was assessed using different VAS scales and at different postoperative intervals, and blood loss was estimated using subjective versus quantitative methods. These inconsistencies inherently inflate heterogeneity and reduce comparability across studies.
Fourth, perioperative care pathways differed widely among studies, including anesthesia type, use of prophylactic antibiotics, bladder catheterization duration, analgesic protocols, and criteria for hospital discharge. Such factors are known to influence pain scores, gastrointestinal recovery, urinary outcomes, and length of stay, yet were rarely controlled for or reported in sufficient detail.
Taken together, the very high heterogeneity observed underscores the need for caution in over-interpreting pooled estimates and highlights the importance of individual high-quality randomized trials with standardized surgical definitions, uniform outcome measures, and transparent reporting. Nonetheless, the consistent direction of effect across multiple clinically relevant outcomes, combined with mechanistic histopathological evidence, suggests that the observed disadvantages associated with bladder flap creation are unlikely to be spurious and warrant serious consideration in contemporary cesarean surgical practice.
Only one study included long term follow up and evaluated adhesion formation mainly. Further subgroup analysis according to technique of CD or type of CD (whether elective or emergency) could not achieved due to limited study numbers. Neonatal outcomes (Apgar score, umbilical cord pH, NICU admission) were not evaluated, despite their known association with incision-to-delivery time. Surgeon experience level was not reported in all studies. Most of the studies were not prospectively registered. Analysis of outcomes may be underpowered to detect rare events.
Comparison with existing reviews
One metaanalysis assessed the value of bladder flap creation during CD [8]. O’Neill study included 4 RCTs (3 published and 1 unpublished) with 581 participants. They reported that omission of bladder flap creation was associated with shorter incision to delivery interval (WMD 1.27 min; p = 0.0001) and associated with no significant differences in the total operative time (WMD 3.5 min), intraoperative blood loss (WMD 42 ml), duration of hospital stay (WMD 0.07 days) or risk of bladder injury (pooled OR 0.96) when compared to women subjected to bladder flap creation. However, this review had limited number of studies with small number of participants. The limited number of studies limited the ability to conduct subgroup analysis. It also lacks assessment of quality of evidence for all outcomes.
Conclusion
This review suggested that omission of bladder flap creation during CD is associated with significant shortening of the operative time (high evidence) and incision to delivery time (high evidence) and a significant reduction in microscopic hematuria (low evidence), postoperative pain score (low evidence) and time to 1st defecation (moderate evidence) compared to women subjected to bladder flap creation. This omission could be associated with similar intraoperative blood loss, duration of hospitalization, risk of bladder injury, urinary tract infection, postoperative urine retention and postoperative complications to those who had bladder flap creation during their CD. Although the evidence of most outcomes is not high enough to strongly recommend omission of bladder flap creation, we suggest this omission in those women when time is very crucial in the procedure outcomes as those with maternal and or fetal distress. There is lack of high-quality multicenter studies considering the different techniques and indications of CD with adequate long term follow up duration addressing the value of creation or omission of bladder flap. A large RCTs focusing specifically on high-risk groups (e.g., women with prior bladder surgery, dense adhesions, emergency CDs for fetal distress) and studies with long-term follow-up for adhesion-related morbidity conduction is recommended. .
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bujold E, Romero R. Uterine closure after Cesarean delivery: surgical principles, biological rationale, and clinical implications. Am J Obstet Gynecol. 2025;Article in press. 10.1016/j.ajog.2025.10.007. ISSN 0002-9378.10.1016/j.ajog.2025.10.00741485855 · doi ↗ · pubmed ↗
- 2Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration. 2011. http://handbook-5-1.cochrane.org. Accessed June 2025.
- 3Elsersy MA. Dec. Usefulness of bladder dissection in cesarean section: a randomized controlled trial. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2016;5(12):4317–20. 10.18203/2320-1770.ijrcog 20164335.
- 4Gül KD, Şolt A. Effects of creation of bladder flap during cesarean section on long-term residual urine volume and postoperative urinary retention. J Surg Med. 2020;4(12):1190–4. Available from. https://jsurgmed.com/article/view/832595. Accessed 20 Oct 2025.
- 5Hohlagschwandtner M, Ruecklinger E, Husslein P, Joura EA. Is the formation of a bladder flap at cesarean necessary? A randomized trial. Obstet Gynecol. 2001;98(6):1089–92. 10.1016/s 0029-7844(01)01570-8. PMID: 11755558.10.1016/s 0029-7844(01)01570-811755558 · doi ↗ · pubmed ↗
- 6Malvasi A, Tinelli A, Guido M, Cavallotti C, Dell’Edera D, Zizza A, et al. Effect of avoiding bladder flap formation in caesarean section on repeat caesarean delivery. Eur J Obstet Gynecol Reprod Biol. 2011;159(2):300–4. 10.1016/j.ejogrb.2011.09.001. Epub 2011 Oct 11. PMID: 21992961.10.1016/j.ejogrb.2011.09.00121992961 · doi ↗ · pubmed ↗
- 7Tuuli MG, Odibo AO, Fogertey P, Roehl K, Stamilio D, Macones GA. Utility of the bladder flap at cesarean delivery: a randomized controlled trial. Obstet Gynecol. 2012;119(4):815–21. 10.1097/AOG.0b 013e 31824 c 0e 12. PMID: 22395144.10.1097/AOG.0b 013e 31824 c 0e 1222395144 · doi ↗ · pubmed ↗