Intracoronary Vasoactive Therapy for No-Reflow During Primary PCI: A Network Meta-Analysis of Randomized Trials
Federico Oliveri, Lorenzo Tua, Luca Raone, Francesco Maria Sparasci, Marco Ferlini, Alessandro Mandurino-Mirizzi, Leonardo De Luca, Fatih Arslan, Brian O. Bingen, Jose’ M. Montero-Cabezas

TL;DR
This study compares medications used during heart procedures to improve blood flow and finds that epinephrine and verapamil are most effective.
Contribution
A network meta-analysis comparing intracoronary medications for treating the no-reflow phenomenon during heart procedures.
Findings
Epinephrine and verapamil significantly improved TIMI flow grade 3 compared to control.
Epinephrine, verapamil, and adenosine improved ST-segment resolution.
No therapies reduced major adverse cardiovascular events or mortality.
Abstract
The no-reflow phenomenon frequently complicates primary percutaneous coronary intervention and is associated with adverse outcomes. Evidence supporting a specific pharmacological treatment is limited. The aim of this study was to compare commonly used intracoronary medications for the treatment of the no-reflow phenomenon. We performed a systematic review and frequentist network meta-analysis of randomized controlled trials comparing intracoronary adenosine, epinephrine, nitroprusside, and verapamil administered during primary percutaneous coronary intervention for the treatment of the no-reflow phenomenon (PROSPERO CRD420251102877). The primary efficacy endpoint was restoration of TIMI flow grade 3 flow at the end of the procedure. Secondary endpoints included ST-segment resolution, major adverse cardiovascular events, and all-cause mortality. Thirteen studies, for a total of 1,674…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
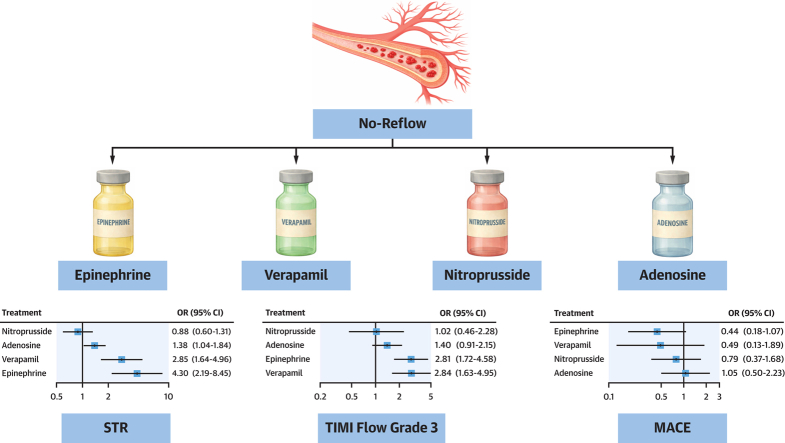 Figure 1
Figure 1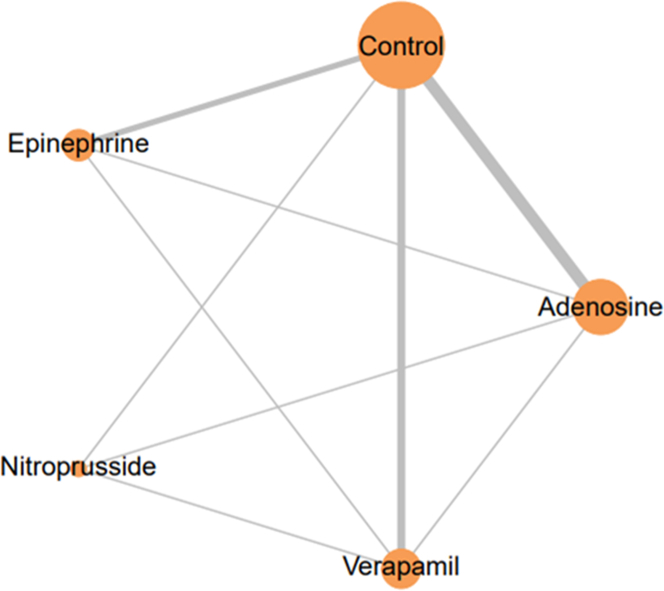 Figure 2
Figure 2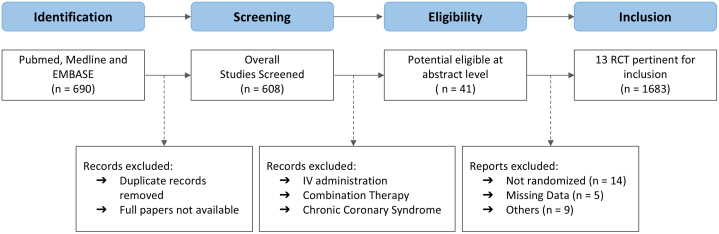 Figure 3
Figure 3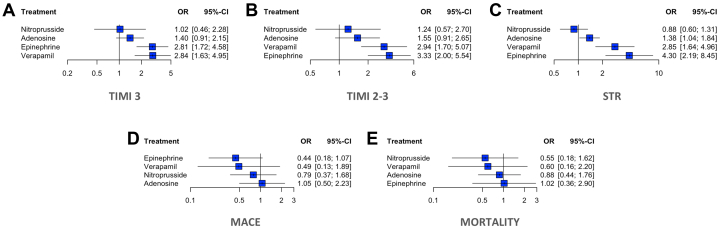 Figure 4
Figure 4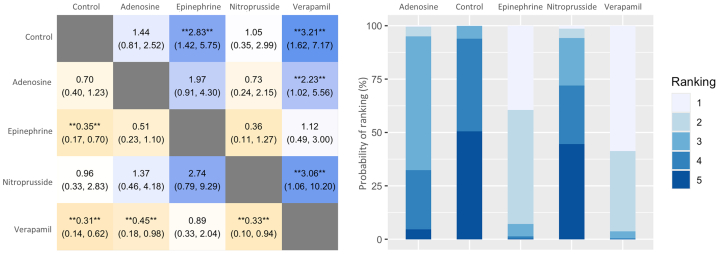 Figure 5
Figure 5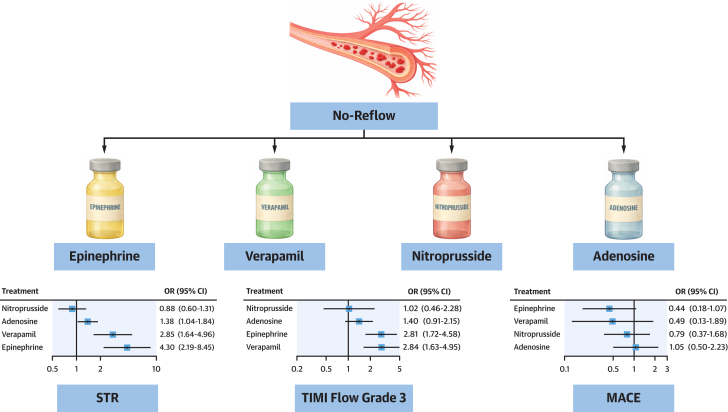 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Acute Myocardial Infarction Research · Cerebrovascular and Carotid Artery Diseases
Although primary percutaneous coronary intervention (PCI) represents the cornerstone of reperfusion therapy in ST-segment elevation myocardial infarction, successful restoration of epicardial coronary patency does not invariably translate into effective tissue-level perfusion.1 The no-reflow phenomenon, defined as persistent myocardial hypoperfusion in the absence of residual epicardial mechanical obstruction, occurs in a substantial proportion of patients and is associated with larger infarct size, worse left ventricular remodeling and increased mortality.2, 3, 4, 5, 6 Its incidence varies widely depending on the diagnostic modality employed, ranging from 5 to 25%.7, 8, 9 The underlying mechanisms of coronary no-reflow are multifactorial and involve a dynamic interplay between mechanical obstruction by microthrombi or plaque debris, endothelial dysfunction, ischemia-reperfusion injury, vasoconstriction, and inflammatory microvascular damage.2^,^3 Recognition of its prognostic relevance has led to the development of multiple pharmacologic strategies aimed at promoting microvascular reperfusion in the acute setting.10 Although several procedural (eg, direct stenting, thrombectomy, or distal embolic protection for graft) and pharmacologic strategies (eg intracoronary vasodilators, glycoprotein (GP) IIb/IIIa inhibitors, and intracoronary thrombolytics) have been proposed to manage the no-reflow phenomenon, none has consistently demonstrated superiority over the others.11^,^12 Recent evidence has shown that intracoronary administration of agents such as adenosine, verapamil, epinephrine, and nitroprusside may play a significant role in restoring coronary flow. However, the lack of standardized dosing protocols and the frequent use of drug combinations, even among different operators within the same center, underscore the variability in current practice and the need for more robust evidence. To address this gap, we conducted a network meta-analysis (NMA) of randomized controlled trials (RCTs) evaluating the efficacy of adenosine, verapamil, epinephrine, or nitroprusside used in the treatment of the no-reflow phenomenon during primary PCI.
Methods
This systematic review and NMA was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.13 The full study protocol was registered in the PROSPERO (CRD420251102877).
Search strategy and data extractions
Four independent reviewers (F.O., L.T., L.R., and F.S.) performed the initial screening of titles and abstracts to identify potentially eligible studies, each one for 1 of the drugs included in our paper (adenosine, epinephrine, verapamil, and nitroprusside). Primary keywords were “adenosine” "epinephrine", “nitroprusside”, “verapamil”,” no-reflow”, “(adenosine OR epinephrine OR nitroprusside OR verapamil) AND no-reflow”. They systematically searched the Pubmed, Scopus, Cochrane, and EMBASE databases starting on February 21, 2025, and finishing on May 30, 2025. In case of disagreement, shared decisions were with other coauthors (M.F. and A.M.M.). Data were therefore extracted independently using a standardized recording tool to document the study setting and design, year of publication, number of study participants, country of origin, participant clinical characteristics, and study outcomes. The Kappa statistic was used to assess the inter-rater reliability of the reviewers.14
Inclusion criteria
The screening focused on studies enrolling patients with acute coronary syndromes undergoing primary PCI. Eligible interventions included intraprocedural intracoronary administration of adenosine, epinephrine, nitroprusside, verapamil, or placebo. Only RCTs were considered for inclusion. Studies were excluded if they involved combination therapies using 2 or more of the aforementioned agents, included patients with stable coronary artery disease, or used intravenous administration of the study drug. Intracoronary medications could be administered at different procedural stages, either before or after balloon inflation or stenting, but never as a preventive strategy before guidewire advancement. We adopted an inclusive definition of “no-reflow,” encompassing both the classical form and persistent no-flow (TIMI flow grade 0) observed after guidewire passage but before balloon inflation or stenting.15 This broader definition was selected to reflect the clinical continuum of impaired myocardial perfusion during PCI, as both phenomena are associated with adverse outcomes and are frequently reported under the umbrella term “no-reflow” in the literature. The use of thrombectomy or GP IIb/IIIa inhibitors was recorded for each study as potential confounders.
Endpoint
The primary efficacy endpoint was the restoration of TIMI flow grade 3 at the end of the procedure. Secondary efficacy endpoints included the achievement of TIMI flow grade 2 to 3 and ST-segment resolution (STR) on electrocardiogram (>70% reduction from baseline). Exploratory clinical outcomes were major adverse cardiovascular events (MACE) and all-cause mortality.
Quality assessment
Two authors (F.O. and L.T.) assessed the risk of bias of all considered RCTs according to the Cochrane Collaboration's tool and Cochrane RoB-2.16 In case of discrepancy, a consensus with a third author (A.M.M.) was made the final evaluation. We explored the potential for publication bias by visual inspection of funnel plots.
Data analysis and synthesis
We conducted a NMA using both frequentist and Bayesian frameworks to evaluate treatments for no-flow in primary PCI. A random-effects model was applied to account for between-study variability. Treatment effects were expressed as ORs for binary outcomes along with their corresponding 95% CIs (frequentist) or 95% credible intervals (CrIs) (Bayesian). Network plots were generated for each outcome to illustrate the geometry of the evidence and the connectivity between interventions. Pooled-effect estimates were summarized using forest plots, whereas treatment rankings were presented using surface under the cumulative ranking curve values and ranking probability plots. Between-study heterogeneity was quantified using the I^2^ statistic and between-study variance (τ^2^). Small study effects and potential publication bias were explored using funnel plots. Bayesian network meta-analyses were conducted using random-effects models. Weakly informative priors were used to minimize prior influence on treatment effect estimates. Treatment effects were assigned normal priors centered at zero with large variance, reflecting no assumed effect a priori, whereas between-study heterogeneity was modeled using a half-normal prior. Posterior distributions were estimated using Markov chain Monte Carlo methods, and model convergence was assessed using the standard diagnostic criteria. Statistical incoherence was assessed globally using the design-by-treatment interaction model and locally through node-splitting analyses. Transitivity was assessed by evaluating the comparability of study populations, clinical context, outcome definitions, and control interventions across trials, as well as the distribution of key procedural characteristics. A contribution matrix was generated for the primary outcome to quantify the relative contribution of each direct comparison to the final network estimates. Prespecified sensitivity analyses were performed to evaluate the robustness of the findings, including leave-one-out analysis and the exclusion of studies at a higher risk of bias for our primary outcome. A meta-regression analysis was conducted to explore the influence of potential effect modifiers, including age, sex, GP IIb/IIIa inhibitor use, and mechanical thrombectomy on the final TIMI flow grade 3. Frequentist analyses were conducted using the netmeta, whereas Bayesian analyses and visualizations were performed using BUGSnet. Additional outputs, such as surface under the cumulative ranking curve rankings and network geometry plots, were also created using MetaInsight (version 6.0.1).
Ethical considerations
Institutional review board or ethics committee approval was not required for this study because it was based exclusively on data from previously published RCTs and did not involve the collection or analysis of individual patient-level data.
Results
A total of 680 records were identified in the preliminary search. A total of 13 studies were used for data extraction and synthesis for our NMA.17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29 Overall, 1,683 patients were included in our study. A total of 516 were treated with intracoronary adenosine, 196 with epinephrine, 189 with nitroprusside, 139 with verapamil, and 554 with control. Network Plot is shown in Figure 1, whereas the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram in Figure 2. Studies and baseline characteristics are detailed in Table 1, Table 2, Table 3, respectively.Figure 1Network Plots of Treatment ComparisonsEach node represents an individual treatment, and lines between nodes indicate direct comparisons available in the included studies. The size of the nodes and the thickness of the lines correspond to the number of studies and comparisons, respectively.Figure 2Network Plots of Treatment ComparisonsIV = intravenous; RCT = randomized controlled trial.Table 1. Studies CharacteristicsFirst AuthorJournalCountryIndicationTreatmentControlSampleTimingFollow-upDesmet et al17European Heart JournalBelgiumSTEMIAdenosine (4 mg)0.9% NaClA: 56C: 54Before PCI12 monthsGarcia-Dorado et al18International Journal of CardiologySpainSTEMIAdenosine (4.5 mg)0.9% NaClA: 100C: 97Before PCI6 monthsNaghshtabrizi et al19Coronary Artery DiseaseIranSTEMIAdenosine (40 ug + 40 ug)0.9% NaClA 52C: 52First dose: after crossingSecond dose: after stenting30 daysNiccoli et al2^,^3^,^21^,^30JACC Cardiovascular InterventionItalySTEMIAdenosine (120 ug + 2 mg)Nitroprusside (60 ug + 100 ug)0.9% NaClA: 80N: 80C: 80Before PCI30 daysPetronio et al20American Heart JournalItalypPCIAdenosinestandard care^a^A: 30C: 30Before PCI6 monthsNazir et al29European Heart JournalUnitedKingdomSTEMIAdenosine (1 mg + 1 or 2 mg)Nitroprusside: (250 ug + 250 ug)standard care^b^A: 82N: 79C: 86First dose: before PCISecond dose: after stenting6 monthsRyabov et al22American Journal of CardiologyRussiaSTEMIEpinephrine 100 mcgstandard care^c^E: 45C: 45After failure of previous treatmentsbefore hospital dischargeAbdelaziz et al28Coronary Artery DiseaseUnitedKingdompPCINitroprusside (60 ug + 120 ug)Verapamil (250 ug + 500 ug)NothingN: 30V: 30After lesion crossing30 daysFaruk Akturk et al26Minerva Cardioangiol.TurkeypPCIAdenosine 240 ugVerapamil 1.5 mg0.9% NaClA: 16V: 15C: 15After PCI6 monthsHuang et al27American Heart JournalChinapPCIVerapamil 200 ug bolus repeatable (max 2 gr)NTG 200 ug bolus repeatable (max 1 gr)V: 34C: 34After PCI30 daysTaniyama et al25JACCJapanpPCIVerapamil 0.5 mgNothingV: 20C: 20After PCI24-25 daysQiao et al31Chinese Journal of Interventional CardiologyChinapPCIVerapamil 200ug0.9% NaClV: 47C: 44After PCI3 monthsYassin et al23Cardiology & Vascular ResearchEgyptpPCIEpinephrine 100 ugVerapamil 200 ugNothingE: 40V: 40C: 40After lesion crossing30 daysKhan et al24Circulation Cardiovasc Interv.PakistanACSAdenosine 60- 1,000 μgEpinephrine 100-600 mcgNothingA: 100E: 101After PCI30 daysA = adenosine; ACS = acute coronary syndrome; C = control; E = epinephrine; N = nitroprusside; NTG = nitroglycerin; PCI = percutaneous coronary intervention; pPCI = primary percutaneous coronary intervention; STEMI = ST-elevation myocardial infarction; V = verapamil.^a^Stenting only; ^b^Standard PPCI alone; ^c^At least 1 among nitroglycerin, adenosine, papaverine, glycoprotein IIB/IIIA inhibitors, and thrombectomy.Table 2. Baseline CharacteristicsFirst AuthorAge (years)Female (%)Thrombectomy (%)GP IIb-IIIa (Inhibitors)TIMI 0-1 (Baseline)MACE DefinitionDesmet et al17A: 61 ± 12C: 61 ± 11A: 21%C: 15%A: NAC: NAA: 91%C: 93%A: 80%C: 63%All-cause mortality and functional status (NYHA functional class)Garcia-Dorado et al18A: 60 ± 12C: 59 ± 14A: 15%C: 12%A: 73%C: 77%A: 63%C: 65%A: 100%C: 100%All-cause mortalityNaghshtabrizi et al19A: NAC: NAA: NAC: NAA: NAC: NAA: 0%C: 0%A: 100%C: 100%All-cause mortalityNiccoli et al2^,^3^,^21^,^30A: 63 ± 11N: 63 ± 10C: 64 ± 13A: 23%N: 26%C: 26%A: 100%N: 100%C: 100%A: 100%N: 100%C: 100%A: 100%N: 100%C: 100%Cardiac mortality, MI, HF, and TLRPetronio et al20A: 56 ± 14C: 61 ± 13A: 17%C: 13%A: NAC: NAA: NAC: NAA: 100%C: 100%All-cause mortality and HFNazir et al29A: 58 ± 13N: 61 ± 13C: 60 ± 11A: 21%N: 16%C: 14%A: 99%N: 95%C: 93%A: NAN: NAC: NAA: 99%N: 91%C: 97%All-cause mortality, MI, HF, and TLRRyabov et al22E: 65 ± 10C: 63 ± 12E: 33%C: 22%E: 33%C: 51%E: 33%C: 51%E: 26%C: 16%Cardiovascular mortality, MI, and HFAbdelaziz et al28N: 53 ± 9V: 53 ± 8N: 33%V: 33%N: 0%V: 0%N: 0%V: 0%N: 100%C: 100%Cardiovascular mortality, MI, HF, and TVRFaruk Akturk et al26A: 56 ± 10V: 59 ± 14C: 58 ± 13A: 25%V: 13%C: 13%A: 0%V: 0%C: 0%A: 100%V: 100%C: 100%A: 94%V: 93%C: 100%NoneHuang et al27V: 65 ± 13C: 66 ± 12V: 24%C: 24%V: 32%C: 38%V: 88%C: 100%V: 82%C: 88%All-cause mortality, MI, and TVRTaniyama et al25V: 61 ± 11C: 67 ± 14V: 25%C: 20%V: NAC: NAV: NAC: NAV: 100%C: 100%NoneQiao et al31V: 61 ± 12C: 64 ± 11V: NAC: NAV: NAC: NAV: NAC: NAV: NAC: NACardiac mortality, MI, HF, and recurrent anginaYassin et al23E: 53 ± 10V: 56 ± 9C: 56 ± 10E: 20%V: 20%C: 23%E: 83%V: 95%C: 80%E: NAV: NAC: NAE: 93%V: 95%C: 93%All-cause mortality, MI, HF, TVR, and TLRKhan et al24A: 57 ± 11E: 57 ± 12A: 24%E: 31%A: NAE: NAA: 20%E: 24%A: 63%E: 59%MI, TVR, cerebrovascular accident, and HFGP = glycoprotein; HF = heart failure; MACE = major adverse cardiovascular effect; MI = myocardial infarction; NA = not available; TLR = target lesion revascularization; TVR = target vessel revascularization; other abbreviations as in Table 1.Table 3. Procedural and Clinical OutcomesFirst AuthorFinal TIMI Flow Grade ≥IIFinal TIMI Flow Grade IIIFinal cTFC (frames)Final MBG 2-3STRMACEOverall MortalityPost-LV-EF (%)VT/VF3° AVBHypotensionDesmet et al17A: 96%C: 96%A: 80%C: 87%A: 34.1 ± 25.2C: 30.5 ± 19.6A: 63%C: 59%A: 45%C: 41%A: 4%C: 4%A: 4%C: 4%A: 47.6 ± 9.5C: 51.3 ± 8.7A: 4%C: 6%A: 18%C: 7%A: NAC: NAGarcia-Dorado et al18A: 99%C: 99%A: 94%C: 88%A: NAC: NAA: 82%C: 82%A: 66%C: 57%A: NAC: NAA: 3%C: 1%A: 49.5 ± 10.4C: 49.4 ± 10.2A: 2%C: 1%A: 2%C: 0%A: NAC: NANaghshtabrizi et al19A: 96%C: 88%A: 85%C: 63%A: NAC: NAA: NAC: NAA: 17%C: 17%A: NAC: NAA: 4%C: 8%A: 40.1 ± 11.9C: 42.9 ± 7.7A: 10%C: 21%A: NAC: NAA: NAC: NANiccoli et al2^,^3^,^21^,^30A: 91%N: 90%C: 90%A: 91%N: 90%C: 90%A: NAN: NAC: NAA: NAN: NAC: NAA: 71%N: 54%C: 51%A: 10%N: 7%C: 20%A: 3%N: 3%C: 4%A: NAN: NAC: NAA: 3%N: 3%C: 3%A: 13%N: 1%C: 3%A: 6%N: 15%C: 9%Petronio et al20A: 93%C: 87%A: 93%C: 87%A: 16 ± 12C: 23 ± 11A: NAC: NAA: 43%C: 53%A: 7%C: 3%A: 7%C: 3%A: 47 ± 10C: 48 ± 6A:13%C: 13%A: NAC: NAA: NAC: NANazir et al29A:NAN: NAC: NAA: NAN: NAC: NAA: NAN: NAC: NAA: NAN: NAC: NAA: 68%N: 61%C: 65%A: 13%N: 5%C: 2%A: 1%N: 1%C: 0%A: 43.2 + 7.9N: 43.9 + 6.5C: 45.7 + 8.0A: 6%N: 4%C: 6%A: 11%N: 4%C: 12%A: 6%N: 4%C: 7%Ryabov et al22E: 56%C: 29%E: 56%C: 29%E: NAC: NAE: NAC: NAE: 78%C: 36%E: 11%C: 22%E: 7%C: 9%E: 51.0 ± 8.6C: 47.0 ± 8.8E: 9%C: 7%E: 0%C: 2%E: NAC: NAAbdelaziz et al28N: 73%V: 90%N: 73%V: 90%N: 26.9 ± 4.5V: 20.1 ± 3.6N: 60%V: 87%N: 17%V: 40%N: 7%V: 3%N: NAV: NAN: 40.5 ± 4.7V: 42.6 ± 4.9N: NAV: NAN: NAV: NAN: 20%V: 3%Faruk Akturk et al26A: 69%V: 80%C: 40%A: 6%V: 27%C: 0%A: 71 ± 46V: 52 ± 48C: 71 ± 37A: NAV: NAC: NAA: 6%N: 7%C: 3%A: NAN: NAC: NAA: 3%N: 2%C: 2%A: 41 ± 9.7N: 42.1 ± 9.9C: 39.9 ± 9.4A: NAN: NAC: NAA: NAN: NAC: NAA: NAN: NAC: NAHuang et al27V: 85%C: 53%V: 85%C: 53%V: 28.4 ± 10.2C: 42.4 ± 17.9V: NAC: NAV: 56%C: 29%V: 9%C: 12%V: 3%C: 9%V: 57 ± 8.9C: 58.1 ± 8.7V: NAC: NAV: 15%C: 0%V: NAC: NATaniyama et al25V: 85%C: 75%V: 85%C: 75%V: NAC: NAV: NAC: NAV: NAC: NAV: NAC: NAV: NAC: NAV: 48 ± 11C: 47 ± 9V: NAC: NAV: NAC: NAV: NAC: NAQiao et al31V: 100%C: 91%V: NAC: NAV: 27.1 ± 14.2C: 39.0 ± 23.8V: 91%C: 75%V: NAC: NAV: 15%C: 18%V: NAC: NAV: 63.4 ± 8.2C: 63.5 ± 10.3V: NAC: NAV: NAC: NAV: NAC: NAYassin et al23E: 65%V: 63%C: 53%E: 65%V: 63%C: 53%E: NAV: NAC: NAE: 85%V: 88%C: 33%E: 83%V: 80%C: 65%E: 1%V: 0%C: 0%E: NAV: NAC: NAE: 46.9 ± 9.3V: 43.9 ± 7.1C: 46.4 ± 7.8E: 5%V: 0%C: 0%E: NAV: NAC: NAE: NAV: NAC: NAKhan et al24A: 78%E: 90%A: 78%E: 90%A: 24 ± 8.4E: 26.6 ± 9.2A: 56%E: 46%A: NAE: NAA: 6%E: 4%A: 6%E: 4%A: NAE: NAA: 0%E: 3%A: NAE: NAA: NAE: NAAVR = atrio-ventricular block; cTFC = Corrected Thrombolysis In Myocardial Infarction Frame Count; LV-EF = left ventricle ejection fraction; MBG = Myocardial blush grade; STR = ST-segment resolution; VF = ventricular fibrillation; VT = ventricular tachycardia; other abbreviations as in Tables 1 and 2.
TIMI flow grade 3
Both epinephrine (OR: 2.81; 95% CI: 1.72-4.58) and verapamil (OR: 2.84; 95% CI: 1.63-4.95) were associated with significantly higher odds of achieving final TIMI flow grade 3 compared with control. In contrast, neither adenosine (OR: 1.40; 95% CI: 0.91-2.15) nor nitroprusside (OR: 1.02; 95% CI: 0.46-2.28) showed a statistically significant difference vs control (Figure 3). Estimated between-study heterogeneity was negligible (τ^2^ = 0; I^2^ = 0%). Findings were consistent in the Bayesian analysis (Supplemental Figure 1). League-plot and ranking-plot analyses indicated that verapamil had the highest probability of achieving final TIMI flow grade 3 (Figure 4).Figure 3Forest Plots of Primary and Secondary Outcomes Compared to Control(A) TIMI flow grade 3; (B) TIMI flow grade 2 to 3; (C) ST-segment resolution (STR); (D) major adverse cardiovascular events (MACE); and (E) overall mortality. Each plot shows the effect estimates and 95% CIs for each treatment compared to control. Heterogeneity: TIMI flow grade 3 (τ^2^ = 0; I^2^ = 0%); TIMI flow grade 2 to 3 (τ^2^ = 0; I^2^ = 0%), STR (τ^2^ = 0; I^2^ = 0%), MACE (τ^2^ = 0; I^2^ = 0%), and mortality (τ^2^ = 0.15; I^2^ = 21.4%).Figure 4League Plots and Ranking Plots for Each OutcomeThe league plots (left) display head-to-head comparisons between treatments. The ranking plots (right) summarize the overall probability of each treatment being the most effective in achieving final TIMI flow grade 3.
TIMI flow grade 2 to 3
In the frequentist analysis, all intracoronary agents were associated with numerically higher odds of achieving TIMI 2 to 3 flow restoration compared with control; however, only epinephrine (OR: 3.33; 95% CI: 2.00-5.54) and verapamil (OR: 2.94; 95% CI: 1.70-5.07) reached statistical significance (Figure 3). Estimated between-study heterogeneity was negligible (τ^2^ = 0; I^2^ = 0%). Findings were consistent in the Bayesian analysis (Supplemental Figure 2).
ST-segment resolution
In the frequentist analysis, STR was significantly improved with epinephrine (OR: 4.30; 95% CI: 2.19-8.45), verapamil (OR: 2.85; 95% CI: 1.64-4.96), and adenosine (OR: 1.38; 95% CI: 1.04-1.84) compared with control. Estimated between-study heterogeneity was negligible (τ^2^ = 0; I^2^ = 0%) (Figure 3). However, in the Bayesian analysis, only epinephrine (OR: 4.43; 95% CrI: 2.14-9.78) and verapamil (OR 2.92; 95% CrI: 1.59-5.37) remained significantly associated with STR (Supplemental Figure 3).
Adverse events
In the frequentist NMA evaluating the effect of intracoronary drugs on MACE, epinephrine was associated with the greatest numerical reduction in risk compared to control (OR: 0.43; 95% CI: 0.17-1.07), followed by verapamil (OR: 0.55; 95% CI: 0.14-2.14) and nitroprusside (OR: 0.80; 95% CI: 0.37-1.70), although none of these comparisons reached statistical significance (Figure 3). Between-study heterogeneity was low with τ^2^ = 0.15 and I^2^ = 21.4%. Results were consistent in the Bayesian analysis (Supplemental Figure 4).
Mortality
None of the evaluated agents demonstrated a statistically significant reduction in mortality compared with control. In the frequentist model, there was a nonsignificant trend toward lower mortality with adenosine, nitroprusside (OR: 0.55; 95% CI: 0.18-1.62), and verapamil (OR: 0.60; 95% CI: 0.16-2.20). Estimated between-study heterogeneity was negligible (τ^2^ = 0; I^2^ = 0%) (Figure 3). The Bayesian model showed a similar neutral effect (Supplemental Figure 5).
Quality assessment
Risk of publication bias and the quality assessment are presented in Supplemental Figures 12 and 13. Most trials were judged as having low risk or some concerns across key domains, with only a few studies presenting a high risk in specific areas such as missing outcome data or deviations from intended interventions (Supplemental Figure 13). Sensitivity analyses excluding higher-risk studies did not materially change the results for the primary endpoint, supporting the robustness of the main findings (Supplemental Figures 27 to 31).
Sensitivity analysis
In the leave-one-out analysis, both epinephrine and verapamil remained associated with higher rates of final TIMI flow grade 3 (Supplemental Materials). When the study by Desmet et al.17 was excluded, adenosine was also associated with a significantly higher rate of TIMI flow grade 3 (OR: 1.69; 95% CI: 1.05-2.71). Following quality assessment, 4 studies were excluded from the sensitivity analysis.18^,^19^,^22^,^25 Results remained consistent with the primary analysis (Supplemental Figures 27 to 31), with adenosine again showing a significant association with improved final TIMI flow grade 3 (OR: 1.53; 95% CI: 1.12-2.10).
Meta-regression
Meta-regression analyses did not reveal any significant confounding effects from baseline age or sex distribution, nor from the intraprocedural use of GP IIb/IIIa inhibitors or mechanical thrombectomy (Supplemental Figures 32 to 35).
Discussion
The results of this NMA of randomized trials can be summarized as follows: 1) among the 4 tested drugs, epinephrine and verapamil significantly improved TIMI flow grade >2; 2) significant STR was consistently achieved with epinephrine and verapamil, and with adenosine only in the frequentist analysis; and 3) all 4 agents showed only nonsignificant trends toward reducing MACE and all-cause mortality (Central Illustration).Central IllustrationIntracoronary Vasoactive Drugs the Treatment of No-ReflowIn primary PCI complicated by no-reflow, verapamil and epinephrine were the most effective agents for restoring coronary flow, with verapamil showing the most consistent benefit across TIMI 3 flow and STR. MACE = major adverse cardiovascular events; STR = ST-segment resolution.
Previously published meta-analyses on the subject presented heterogeneous inclusion criteria, as well as sparse treatment options and timing. Laborante et al32 only included studies comparing intracoronary or intravenous adenosine vs placebo (increasing heterogeneity), whereas Niu et al33 assessed the effect of 7 intracoronary agents (adenosine, anisodamine, diltiazem, nicorandil, nitroprusside, urapidil, and verapamil), most of which are not used in daily practice, and did not include epinephrine.
Methodologically, our meta-analysis specifically focused on 4 routinely-used drugs for the treatment of the no-flow phenomenon (adenosine, epinephrine, nitroprusside, and verapamil), with intracoronary administration through a microcatheter or an over-the-wire balloon. We excluded studies combining the 4 pharmacological strategies together and only allowed combination with nonvasoactive agents such as GP IIb/IIIa inhibitors. Furthermore, we only included randomized controlled studies. Such strict criteria for study selection enabled a more reliable analysis of each single drug separately. Thus, all the included studies could be comparable, as it can be appreciated by the low heterogeneity and by the “leave-one” analysis that assessed the influence of each study on the overall extracted results.
Classically, the management of no-reflow depends on intracoronary vasodilation. Overall, in our NMA only epinephrine and verapamil showed a statistically significant improvement in flow restoration (both defined as TIMI flow grade 3 and TIMI flow grade >2) as well as in STR. Although these 2 agents share a common final effect of vasodilatation (epinephrine through beta 2 receptors, verapamil through calcium channel blockage), epinephrine also features beta 1 receptor-mediated inotropic and chronotropic stimulation, which can increase the coronary flow. Previous studies showed that intracoronary epinephrine administration for the management of no-flow during primary PCI yielded significantly better coronary flow patterns compared to those treated with conventional agents such as nitrates, adenosine, thrombectomy, and Gp IIb/IIIa inhibitors.34 As far as the 2 remaining agents, both are regarded as effective for reducing the incidence of no-reflow; however, adenosine can increase the risk of atrioventricular block and has a relatively short half-life, which requires repeated administrations.35 Moreover, both adenosine and nitroprusside increase the risk dose-related hypotension.36 The findings of this NMA are somewhat in contrast with the current practice, where adenosine is the most widely used drug as a first line treatment; epinephrine is commonly a second line drug after failure of flow restoration with adenosine, and, on the other hand, verapamil is rarely used.
Although angiographic (ie, TIMI flow grade) or instrumental (ie, STR) benefits were found in our NMA for some agents (epinephrine and verapamil), no significant benefit was found regarding clinical outcomes. This could have several explanations: first, TIMI flow grade and STR bear the limitations of all surrogate endpoints, which do not fully capture the complexity of clinical and late-manifesting outcomes.37 Second, the no-reflow phenomenon is a transient phenomenon, which can be acutely and angiographically solved by the vasoactive agent, without, nevertheless, yielding a long-term resolution of the underlying myocardial damage. Third, the studies assessed the clinical outcomes with relatively short follow-up periods (maximum of 6 months) and this could miss significant differences in the long-term. Fourth, the majority of the included studies presented relatively low sample sizes (on average between 100 and 200 patients) and could therefore be underpowered for detecting clinical outcomes such as MACE or death. Fifth, the exact mechanism behind the no-flow/no-reflow phenomenon is still debated and multifactorial, with possible concomitant implications of microvascular obstruction by debris, endothelial dysfunction as well as reperfusion injury30: it is possible that each tested drug targets some, but not all, of these mechanisms. And finally, the effects of the tested agents could be confounded by underlying and pre-existing cardioprotective therapies that vary from patient to patient (such as antiplatelet therapy, beta-blockers, and statins).
Study limitations
The findings of this NMA should be interpreted considering some limitations. First, we acknowledge that the broad definition of no-reflow used in the included studies, even if reflecting the terminology adopted in the original study, may introduce conceptual heterogeneity and potential classification bias. Then, the included studies all compared the 4 tested drugs in a different fashion, such as one-to-one comparison of a drug with another, or with a placebo, or a comparison of 3 different strategies; moreover, no direct comparison between epinephrine and nitroprusside was present. However, as already mentioned, the absence of studies where the different strategies were combined provide a clear separation of the pharmacological effects from which our findings can be inferred. Then, some procedural differences were present, such as the timing and dosage of the drugs among studies and the usage, at operator discretion, of balloon inflation before intracoronary infusion, potentially affecting our results. This aspect mainly reflects the absence of a shared consensus on the best approach to the reflow phenomenon, procedurally and pharmacologically; in this context, our NMA could guide future studies to clear such gaps in evidence. As already mentioned in the discussion section, the relatively small sample sizes and short follow-up also represent limitations that underpower each single study for the analysis of clinical outcomes. Nevertheless, due to the relatively low number of studies, the meta-regression analysis may lack sufficient statistical power and therefore results are exploratory and should not be considered definitive. Moreover, due to the small number of studies contributing to each comparison, funnel plots offer only limited interpretability and may not reliably detect publication bias; therefore, these assessments should be viewed as exploratory.
Conclusions
In primary PCI complicated by no-reflow, verapamil and epinephrine were associated with significantly higher odds of achieving final TIMI flow grade 3 compared with controls, with verapamil showing the most consistent benefit across TIMI flow grade 3 and STR. Adenosine and nitroprusside showed no clear association compared with controls. Further studies are needed to clarify optimal agent selection, dosing, and timing of administration.
Funding support and author disclosures
The Department of Cardiology of the Leiden University Medical Center received unrestricted research grants from 10.13039/100011949Abbott Vascular, 10.13039/100004326Bayer, 10.13039/501100005035Biotronik, 10.13039/100008497Boston Scientific, 10.13039/100006520Edwards Lifesciences, 10.13039/100006775GE Healthcare, and 10.13039/100004374Medtronic. Dr Montero-Cabezas received a research grant from Shockwave Medical and speaker fees from 10.13039/100020297Abiomed, 10.13039/100008497Boston Scientific, and 10.13039/100020501Penumbra Inc. Dr De Luca received speaker fees from 10.13039/100002429Amgen, 10.13039/501100015704Aspen, 10.13039/100004325AstraZeneca, 10.13039/100004326Bayer, 10.13039/100001003Boehringer Ingelheim, Chiesi, Daiichi Sankyo, Eli Lilly, Menarini, Novonordisk, Pfizer/Bristol-Myers Squibb, Sanofi, and Servier. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Byrne R.A.Rossello X.Coughlan J.J.2023 ESC guidelines for the management of acute coronary syndromes Eur Heart J 44382023372038263762265410.1093/eurheartj/ehad 191 · doi ↗ · pubmed ↗
- 2Niccoli G.Burzotta F.Galiuto L.Crea F.Myocardial no-reflow in humans J Am Coll Cardiol 54420092812921960802510.1016/j.jacc.2009.03.054 · doi ↗ · pubmed ↗
- 3Niccoli G.Scalone G.Lerman A.Crea F.Coronary microvascular obstruction in acute myocardial infarction Eur Heart J 37132016102410332636428910.1093/eurheartj/ehv 484 · doi ↗ · pubmed ↗
- 4Montone R.A.Vetrugno V.Santacroce G.Recurrence of angina after ST-segment elevation myocardial infarction: the role of coronary microvascular obstruction Eur Heart J Acute Cardiovasc Care 10620216246323161738710.1177/2048872619880661 · doi ↗ · pubmed ↗
- 5Sattur S.Sarwar B.Sacchi T.J.Brener S.J.Correlation between markers of reperfusion and mortality in ST-elevation myocardial infarction: a systematic review J Invasive Cardiol 2611201458759525364000 · pubmed ↗
- 6Hamirani Y.S.Wong A.Kramer C.M.Salerno M.Effect of microvascular obstruction and intramyocardial hemorrhage by CMR on LV remodeling and outcomes after myocardial infarction: a systematic review and meta-analysis JACC Cardiovasc Imaging 7920149409522521280010.1016/j.jcmg.2014.06.012PMC 4301583 · doi ↗ · pubmed ↗
- 7Mehta R.H.Harjai K.J.Cox D.Clinical and angiographic correlates and outcomes of suboptimal coronary flow inpatients with acute myocardial infarction undergoing primary percutaneous coronary intervention J Am Coll Cardiol 42102003173917461464268110.1016/j.jacc.2003.07.012 · doi ↗ · pubmed ↗
- 8Morishima I.Sone T.Okumura K.Angiographic no-reflow phenomenon as a predictor of adverse long-term outcome in patients treated with percutaneous transluminal coronary angioplasty for first acute myocardial infarction J Am Coll Cardiol 3642000120212091102847110.1016/s 0735-1097(00)00865-2 · doi ↗ · pubmed ↗