A systematic review and meta-analysis of pazopanib efficacy and adverse effects in sarcomas
Fernanda Picozzi, Alessandro Ottaiano, Antonella Lucia Marretta, Mariachiara Santorsola, Lucia Cannella, Antonio Pizzolorusso, Francesco Caraglia, Giuseppina Della Vittoria Scarpati, Alessandra Bracigliano, Ottavia Clemente, Ines Simeone, Michele Caraglia, Salvatore Tafuto

TL;DR
This study reviews pazopanib's effectiveness and side effects in treating sarcomas, finding it has a manageable toxicity profile and is not worse than other treatments.
Contribution
The study provides a systematic review and meta-analysis of pazopanib's efficacy and toxicity in sarcomas, highlighting histology-specific responses.
Findings
Pazopanib showed highest response rates in desmoid tumors and alveolar soft part sarcoma.
Common side effects included hypertension and liver abnormalities.
Pazopanib did not show significant survival advantage over non-placebo treatments.
Abstract
Pazopanib, a multi-targeted tyrosine kinase inhibitor, is employed in the treatment of various malignancies, including metastatic non-adipocytic soft tissue sarcoma. This systematic review and meta-analysis adhered to PRISMA guidelines to evaluate the efficacy and toxicity of pazopanib monotherapy in treating sarcomas. A comprehensive search of PubMed/MEDLINE and Scopus/ELSEVIER databases was conducted, covering the period from 2009 to 2025. The included studies were evaluated for quality using the MINORS, Newcastle-Ottawa Scale, and RoB2 tools. The spectrum of toxicities and responses in sarcoma types was described. A meta-analysis was performed to compare the efficacy of pazopanib with non-placebo treatments, using both fixed-effect and random-effect models to calculate pooled hazard ratios (HRs) for progression-free survival (PFS) and overall survival (OS). A total of 40 studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
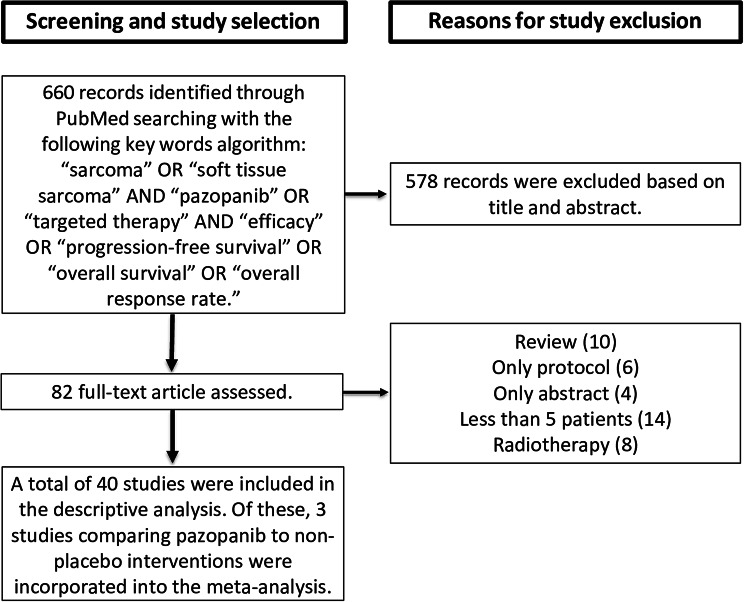 Figure 1
Figure 1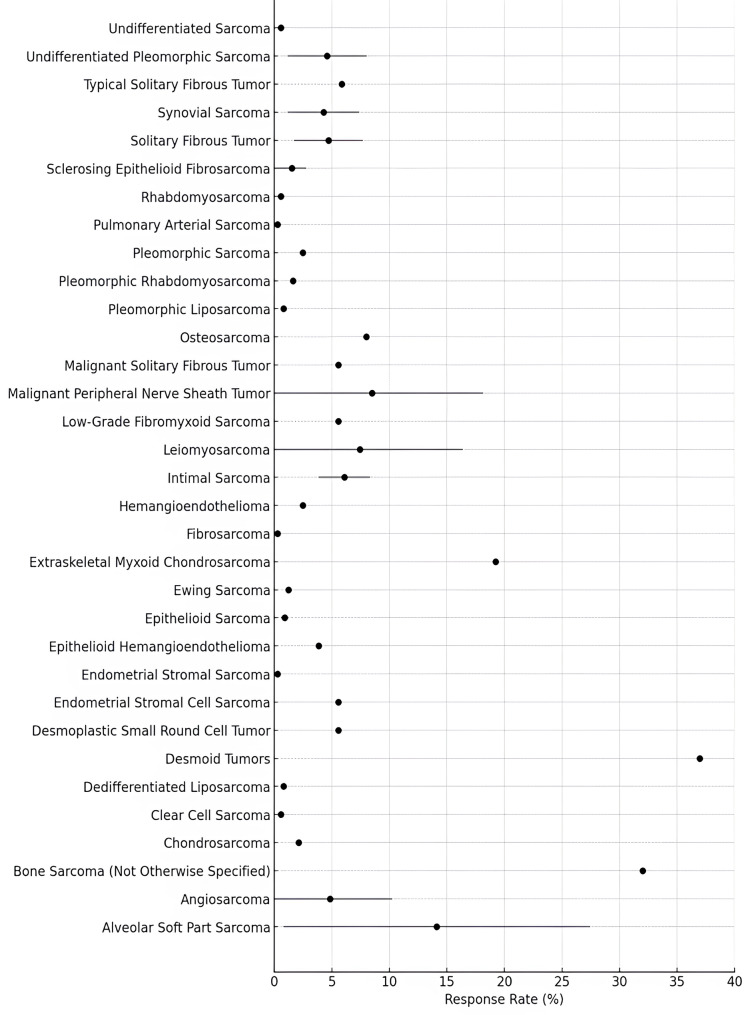 Figure 2
Figure 2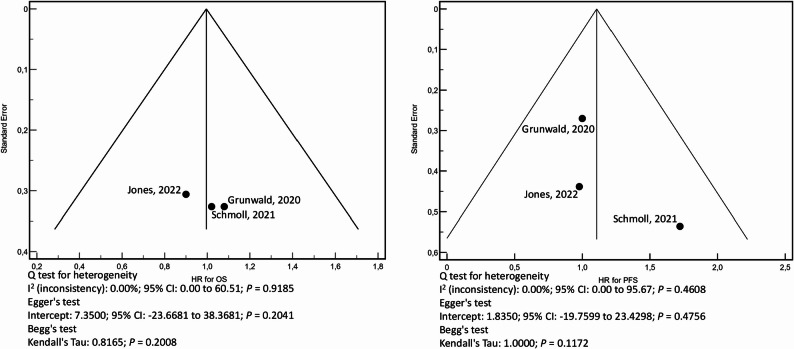 Figure 3
Figure 3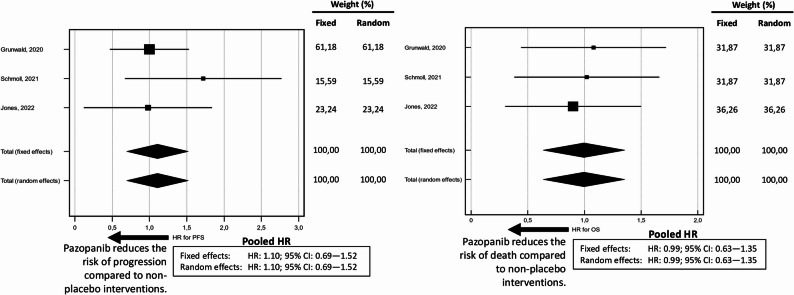 Figure 4
Figure 4- —http://dx.doi.org/10.13039/501100003852Regione Campania
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Soft tissue tumor case studies · Lung Cancer Treatments and Mutations
Introduction
Pazopanib is an oral multi-targeted tyrosine kinase inhibitor (TKI) with a well-established role in the treatment of various malignancies. As a sulfonamide compound, pazopanib inhibits several key receptor tyrosine kinases (RTKs), including vascular endothelial growth factor receptors (VEGFR-1, VEGFR-2, and VEGFR-3), platelet-derived growth factor receptors (PDGFR-α and PDGFR-β), and fibroblast growth factor receptor (FGFR) [1].
The primary mechanism of action of pazopanib involves the inhibition of angiogenesis, a hallmark of tumor progression and metastasis [2]. VEGF signaling is a major driver of angiogenesis in many cancers, including sarcomas. Pazopanib binds to the intracellular domain of VEGF receptors, blocking their autophosphorylation and thereby inhibiting downstream signaling pathways that promote endothelial cell proliferation and neovascularization [3]. Concurrent inhibition of PDGFR and FGFR enhances its anti-tumor efficacy by disrupting stromal support and impairing tumor cell proliferation [4, 5].
Sarcomas are a heterogeneous group of rare malignancies arising from mesenchymal tissues. Representing approximately 1% of all adult cancers, sarcomas encompass over 90 histological subtypes, contributing to their therapeutic complexity [6]. While surgery remains the cornerstone of treatment for localized disease, the management of metastatic or unresectable sarcomas remains challenging, primarily due to the limited efficacy of conventional cytotoxic chemotherapy. Standard first-line regimens for advanced sarcomas typically include monotherapies or combinations of agents such as anthracyclines, ifosfamide, cisplatin, etoposide, and vincristine. However, objective response rates per RECIST criteria are generally low, and the prognosis remains poor, with median overall survival ranging from 12 to 18 months in metastatic cases [7].
In recent years, pazopanib has emerged as an important therapeutic option for patients with metastatic non-adipocytic soft tissue sarcoma (STS) who have previously received chemotherapy. A pivotal randomized, double-blind, placebo-controlled phase III trial involving 369 patients demonstrated a significant improvement in progression-free survival (PFS) with pazopanib compared to placebo (median PFS: 4.6 months vs. 1.6 months; hazard ratio [HR] = 0.31, 95% confidence interval [CI]: 0.24–0.40, P < 0.0001), leading to its regulatory approval in this setting [8]. However, in addition to adipocytic sarcomas, several other histological subtypes were excluded from the trial, including embryonal rhabdomyosarcoma, chondrosarcoma, osteosarcoma, Ewing tumors, primitive neuroectodermal tumors, gastrointestinal stromal tumors (GISTs), dermatofibrosarcoma protuberans, inflammatory myofibroblastic sarcoma, malignant mesothelioma, and mixed Müllerian tumors of the uterus. These exclusions were based on the limited or absent evidence of pazopanib’s efficacy in these histologies at the time of trial design, as well as their distinct biological and molecular profiles compared to other soft tissue sarcomas.
The aim of this study is to provide a comprehensive evaluation of pazopanib monotherapy in patients with sarcomas, specifically assessing its therapeutic activity, as measured by clinical response outcomes, and its safety profile, as defined by the incidence and severity of treatment-related toxicities. Additionally, we evaluate the current literature comparing pazopanib with other active therapeutic alternatives, and assess whether these comparisons translate into meaningful survival benefits. Through this analysis, we aim to contribute to the growing body of evidence on the efficacy and safety of pazopanib, and to further define its role as a single-agent therapy in the treatment landscape for patients with advanced sarcomas.
Methods
This paper details a systematic review and meta-analysis investigating the toxicity and efficacy of pazopanib in treating sarcomas. The study adheres to the 2020 PRISMA guidelines [9] and was conducted under a meticulously crafted protocol registered with PROSPERO (Prospective Register of Systematic Reviews, managed by the National Institute for Health Research, UK) under CRD42024583953. The protocol outlines in detail the criteria for study selection and the methodologies implemented throughout the review process.
Search strategy and selection criteria
A comprehensive manual search was carried out in the PubMed/MEDLINE and Scopus/ELSEVIER databases. A manual search strategy was employed to ensure a thorough and context-specific inclusion of studies. To enhance the accuracy and breadth of the search, five researchers were divided into two independent teams (Team 1: F.P., A.L.M, M.S.; Team 2: A.O., S.T.). Team 1 initiated the search, and Team 2 replicated it to ensure consistency and reliability. This dual approach leveraged the varied expertise and perspectives of the researchers, enhancing the sensitivity of the search. Although labor-intensive, this manual strategy allowed for a deeper understanding of the scientific literature, ensuring the inclusion of studies that might be overlooked by automated searches. Each researcher independently reviewed the relevant databases, journals, and supplementary sources, including reference lists of selected articles, to enhance the final dataset. To maintain the integrity of the selection process, the team held regular consensus meetings to resolve any discrepancies that arose.
The search utilized the following keywords: “sarcoma” OR “soft tissue sarcoma” AND “pazopanib” OR “targeted therapy” AND “efficacy” OR “progression-free survival” OR “overall survival” OR “overall response rate.” The literature search spanned from January 2009 to June 2025, utilizing PubMed/MEDLINE and Scopus/ELSEVIER databases known for their comprehensive coverage of biomedical research. The chosen timeframe was carefully selected to include high-quality studies that reflect the most recent advancements in sarcoma treatment, while also capturing relevant historical data.
Specific inclusion criteria were applied to identify relevant studies. Only English-language articles were included, as English is the primary language of scientific communication in clinical oncology, and this criterion is commonly adopted in systematic reviews to ensure consistency, interpretability, and comparability of methodological and outcome data across studies. The review focused on studies involving individuals aged 18 and older with histologically confirmed sarcomas. Eligible studies had to meet the following criteria: (1) evaluate the effect of pazopanib as a single agent, (2) report Hazard Ratios (HRs) with 95% Confidence Intervals (CIs) or response rates (RRs) by RECIST (3) include a sample size of more than five patients, and (4) achieve a score of ≥ 4 on the Newcastle-Ottawa Scale for assessing the quality of non-randomized studies. Regarding response assessment, two studies evaluated response using both RECIST and CHOI criteria. However, only the RECIST-based response was included in our descriptive analyses. Studies that focused solely on prognostic factors affecting pazopanib efficacy were excluded. Studies primarily focused on pharmacokinetic or pharmacodynamic parameters were excluded, as the objective of this review was to evaluate clinical outcomes. Specifically, we did not include studies investigating intra-patient variability in drug plasma concentrations, exposure–response relationships based on therapeutic drug monitoring cohorts, dose–concentration correlations, or pharmacodynamic markers such as target inhibition or modulation of downstream signaling pathways. Data on HRs and RRs were extracted from all sections of the articles, including supplementary materials.
There were no restrictions on the study design or specific chemotherapy regimens used as comparator interventions in randomized trials. Preclinical studies that focused exclusively on in vitro or animal experiments were excluded from the analysis. Studies incorporating additional treatments (radiotherapy, biological drugs, surgery) were excluded to ensure a more accurate and focused analysis of pazopanib effects. A detailed flowchart illustrating the study selection process is provided in Fig. 1.
Fig. 1. Flowchart illustrating the selection process of studies
Data extraction
For each study, we extracted key details including the first author’s name, publication year, patient count, study design information, clinicopathological characteristics (such as age, gender, histotype, objective response by RECIST, line of therapy, toxicity types, and treatment adherence), follow-up data, and hazard ratios (HRs) for progression and/or mortality, along with their 95% confidence intervals (CIs). Any discrepancies or inconsistencies encountered during data extraction were discussed among the research team to reach a consensus.
Primary objectives
This review and meta-analysis aimed to achieve two main goals: first, to provide a comprehensive evaluation of the responses and toxicities associated with pazopanib in sarcomas, and second, to assess the relative benefits of pazopanib compared to non-placebo interventions.
Quality assessment
To thoroughly evaluate study quality and potential biases, two separate teams, Team 1 and Team 2, were assigned to assess the methodologies and outcomes of the selected studies. For non-randomized trials, the quality was assessed using the MINORS (Methodological Index for Non-Randomized Studies) [10] and the Newcastle–Ottawa Scale (NOS) criteria [11]. For randomized controlled trials, the Risk of Bias 2 (RoB2) tool [12] was employed. Each team independently rated the studies, and any differences in scoring were resolved through discussion until agreement was reached. The distinct characteristics of the MINORS, NOS, and RoB2 scales, and their respective applications, are elaborated in Supplementary File 1.
Statistical methods
A meta-analysis was undertaken to evaluate the comparative efficacy of pazopanib against non-placebo treatments. Both fixed-effect and random-effect models were employed, utilizing the DerSimonian and Laird method [13]. In summary, the fixed-effect model operates under the assumption that the true effect size remains consistent across all studies, with variations in observed effect sizes being attributed solely to random fluctuations. Conversely, the random-effect model acknowledges potential differences in the true effect size across studies, attributing observed variations to a combination of random error and genuine differences. Under this model, the true effect size is presumed to vary between studies, and the overall effect is calculated as a weighted average of the individual study effects. This approach often provides a more conservative estimate of the pooled hazard ratio (HR), particularly in the presence of heterogeneity across studies. The results are visually represented using forest plots, which illustrate the hazard ratios (HRs) along with their 95% confidence intervals (CIs) as error bars. The pooled HR estimates are prominently displayed at the end of the graphs.
For clarity and consistency in interpreting the results, it is essential to clarify that the HR compares the likelihood of disease progression or mortality between patients receiving pazopanib and those receiving non-placebo treatments. A HR of 1.0 indicates no difference in risk between the two groups, whereas a HR below 1.0 suggests that pazopanib is associated with a reduced risk of progression or death. Where necessary, HRs were recalculated using Altman’s method to ensure uniformity in the comparative analysis between pazopanib and non-placebo treatments [14].
Study heterogeneity was assessed using the I² statistic [15], which quantifies the percentage of variability across studies attributable to real differences rather than random error. The assessment and interpretation of the I² statistic are reported in Supplementary File 2. Given the high heterogeneity observed among the studies, as indicated by positive results for heterogeneity, no attempts were made to pool the odds ratios for ORR and DCR. In contrast, no such heterogeneity was recorded in studies reporting time-to-outcome.
Publication bias was evaluated using funnel plots [16]. This procedure involves several steps. Initially, effect sizes (HRs) and their corresponding standard errors (SEs) are extracted from the selected studies and plotted on a scatter plot, with effect sizes on the x-axis and precision (SEs) on the y-axis. In the absence of bias, the plot should resemble a symmetrical funnel, where smaller studies are more widely dispersed and larger studies are concentrated towards the top. Deviations from this symmetry may indicate the presence of publication bias, which requires careful consideration of the observed asymmetry’s direction and magnitude. Asymmetry may arise due to selective reporting or methodological inconsistencies. Conceptually, the funnel represents the expected distribution of studies in the absence of bias. Statistical tests, such as Egger’s and Begg’s tests, were applied to formally assess and quantify asymmetry, providing an objective measure of potential publication bias [16]. Detecting asymmetry helps determine whether the overall results might be disproportionately influenced by positive or significant findings. A symmetrical funnel plot suggests a lower probability of publication bias, thereby enhancing the internal validity of the study findings.
All statistical analyses were performed using MedCalc Statistical Software (MedCalc^®^ Statistical Software version 19.6, MedCalc Software Ltd., Ostend, Belgium) and Microsoft Excel^®^ for Windows, version 2302 (Microsoft Corporation, Redmond, WA, USA).
Results
Study characteristics
A total of 40 studies were included in the present analysis, encompassing both prospective and retrospective designs, with phases ranging from not reported to phase II and III trials [8, 17–55] (Table 1). The number of patients enrolled varied widely, from as few as 6 patients [26] to as many as 1964 patients [8]. The median follow-up period also exhibited significant variation, ranging from 7 months [39] to 63 months [46].
Table 1. Sample size, median follow-up, study design, and quality assessment of selected studies by NOS and MINORS scalesFirst authorYearNo. ofpatientsMedianfollow-up time (months)Study designPhase of the studyNOS scoreMINORS scoreSleijfer S200914222.5ProspectiveII712van de Graaf WTA201236914.9ProspectiveIIINANAYoo KH20154312.0RetrospectiveNR610Maruzzo M20151312.3ProspectiveNR69Nakamura T2016156NRRetrospectiveNR79Kollàr A20175215.9RetrospectiveNR66Jones RL20177NRRetrospectiveNR45Kim HJ20173534RetrospectiveNR68Stacchiotti S20183027RetrospectiveNR68Frezza AM201818NRRetrospectiveNR45Kim M2019633ProspectiveII49Sunar V20192810.7RetrospectiveNR510Stacchiotti S20192627ProspectiveII813Martin-Broto J20193627ProspectiveII813Toulmonde M20197223.4ProspectiveIINANASeto T2019123NRRetrospectiveNR77Frezza AM20191236.3RetrospectiveNR55Hirbe AC20205610.83ProspectiveII511Grunwald V202012011.8ProspectiveIINANAMartin-Broto J20203418ProspectiveII813Aggerholm-Pedersen N20201910RetrospectiveNR67Nishida Y20201210.6RetrospectiveII68Oh CR2020347NRRetrospectiveNR79Chow W20204741.0ProspectiveII712Halim NA2020157RetrospectiveNR67Liu J20203135.6RetrospectiveNR710Schmoll HJ20218639ProspectiveIINANAKataria B20213318.8RetrospectiveNR67Park C202124NRRetrospectiveNR56Alshamsan B20214512.4RetrospectiveNR79Frezza AM20211215.4RetrospectiveNR57Jones RL202211463ProspectiveIIINANAFrankel P20221214.8ProspectiveII55Thiebaud JA202229NRProspectiveII67Hong JY20231840.9ProspectiveNR68Giani C20243662.1RetrospectiveNR710Vincenzi B2024196451.36ProspectiveNR69Söylemez CM202481NRRetrospectiveNR68Burkhard-Meier A20251351.4RetrospectiveNR58Ecker N202599NRRetrospectiveNR67MINORS: Methodological Index for Non-Randomized Studies; NOS: Newcastle–Ottawa Scale; NR: Not Reported
Of the 40 studies, 17 were prospective, primarily phase II trials. These prospective studies generally demonstrated robust methodological quality, as indicated by relatively high scores on the NOS and MINORS scales (Table 1). In contrast, 23 studies were retrospective, showing a broader range of methodological quality. For instance, Nakamura T et al. [20] included 156 patients and achieved a NOS score of 7 and a MINORS score of 9, indicating good methodological rigor despite the retrospective design. Conversely, other retrospective studies, such as the one by Jones RL et al. [22] involving 7 patients, had lower NOS and MINORS scores of 4 and 5, respectively, reflecting a less rigorous study design. Overall, the studies analyzed exhibited a broad spectrum of quality and design, with prospective studies generally achieving higher methodological scores and longer follow-up periods compared to retrospective studies. The quality of the included randomized studies was evaluated using the RoB2 tool, and the results are summarized in Table 2. The studies presented varying levels of risk of bias across different domains, with some demonstrating consistently low risks, while others showed moderate to high concerns in specific areas. Among these, four studies reported a comparison between pazopanib and a comparator other than placebo [30, 33, 41, 46].
Table 2. Quality assessment of randomized studies through RoB2 toolFirst authorComparatorYearRandomization processDeviations from intended interventionMissing outcome dataMeasurement of the outcomeSelection of the reported resultOverall biasvan de Graaf WTAPlacebo2012low risklow risklow risklow risklow risklow riskToulmonde MMethotrexate-Vinblastine2019low risksome concerslow risklow risksome concernssome concernsGrunwald VDoxorubicin2020some concernslow risklow risklow risksome concernssome concernsSchmoll HJPazopanib-Gemcitabine2021some concernslow risksome concernslow risksome concernssome concernsJones RLPazopanib-Carotuximab2022some concernslow riskhigh risksome concernssome concernshigh risk
Clinico-pathological characteristics of enrolled patients
Table 3 provides a summary of the key demographic and clinical characteristics across the selected studies. The patient populations in the pazopanib trials were diverse, varying in age, gender, histology, and line of therapy. The median ages of patients ranged from 26 to 78.7 years, indicating a wide age spectrum. Gender distribution also varied significantly, with the number of male participants ranging from 0 (in studies focused on gynecological sarcomas) to 743, and female participants from 3 to 1221. Histologically, the studies predominantly concentrated on either specific types of sarcoma or a broader array of multiple sarcoma histologies. Only a few studies included osteosarcomas [31, 32]. The line of therapy varied among the studies, with most trials assessing pazopanib in a non-first-line setting, typically involving patients who had already undergone prior treatments.
Table 3. Clinico-pathologic characteristics of selected studiesFirst AuthorYearMedian age (years)GenderHistologyLine of therapyMaleFemaleSingle sub-type of STSMultiple STSMultiple sarcomas including osteosarcomasFirst-lineOther than firstAnySleijfer S200951.47171√√van de Graaf WTA201256.799147*√√Yoo KH2015542617√√Maruzzo M20155167√√Nakamura T201653.89759√√Kollàr A201762.43220√√Jones RL20175234√√Kim HJ201757035√√Stacchiotti S2018331911√√Frezza AM201831135√√Kim M201929.533√√Sunar V201953028√√Stacchiotti S201963215√√Martin-Broto J2019621521√√Toulmonde M2019351731*√√Seto T2019605865√√Frezza AM20225175√√Hirbe AC202078.72927√√Grunwald V2020714437*√√Martin-Broto J2020631717√√Aggerholm-Pedersen N202039145√√Nishida Y20204966√√Oh CR202051170177√√Chow W2020582918√√Halim NA202048.687√√Liu J2020261021√√Schmoll HJ2021592320*√√Kataria B2021471815√√Park C2021NRNR√√Alshamsan B2021282322√√Frezza AM20214648√√Jones RL202262.61835*√√Frankel P20223275√**√Thiebaud JA2022661217√√Hong JY202318810√√Giani C2024NRNRNR√√Vincenzi B202459.77431221√√Söylemez CM2024NR3051√√Burkhard-Meier A20254376√√Ecker N202549.84653√√*These data pertain solely to the pazopanib arm. **Osteosarcoma
Efficacy of pazopanib
As anticipated, the studies demonstrated variability in ORR by RECIST, disease control rate (DCR), and survival outcomes, including PFS and overall survival (OS) (Table 4). Two studies [29, 34] reported responses evaluated using both RECIST and CHOI criteria. The reported ORR varied widely across the studies, ranging from 0% to 37%. The table lists the histological types in which responses according to RECIST were detected. The highest response rates were reported in desmoid tumors with an ORR of 37% [30] and in alveolar soft part sarcoma (ASPS) with an ORR of 35.5% [40]. Several studies reported no response at all in chondrosarcomas and angiosarcomas [22, 46], in epithelioid sarcomas, epithelioid haemangioendothelioma [25, 45], haemangioendothelioma [54], and in undifferentiated STSs, synovial sarcomas, leiomyosarcomas, angiosarcoma, and desmoid tumor [39], where the ORR was 0%. DCR was inconsistently reported, ranging from 13.3% to 100%. The highest DCR by RECIST was observed in ASPS (100%) [26] and in typical solitary fibrous tumors (100%) [34]. Desmoid tumors also showed a high DCR of 96% [30], while the lowest DCR (13.3%) was observed in undifferentiated STSs and synovial sarcoma [39]. Data on PFS and OS were limited, with HR reported only in a few studies (Table 4). A Forest Plot illustrating the response rates across different histotypes is presented in Fig. 2.
Table 4. Detailed outcomes in the selected articlesFirst authorYearSample sizeResponse to treatmentProgression-free survivalOverall survival CR
no(%)
Histotype with CR
ORR (%)*
Responsive histotypes
DCR (%)
HR**
CI
p
HR**
CI
p Sleijfer S20091420-6.3LMS, SSNRNRNRNRNRNRNRvan de Graaf WTA20123690-6NR730.310.24–0.40< 0.00010.860.67–1.110.2514Yoo KH2015430-16.3SS, MFH, UPS, MPNST, LMS, angiosarcoma60.2NRNRNRNRNRNRMaruzzo M2015130-9Solitary fibrous tumours82NRNRNRNRNRNRNakamura T20161560-8.3UPS, SS, ASPS55.7NRNRNRNRNRNRKollàr A2017521(1.9)HE23.1Angiosarcoma, epithelioidHE, intimal sarcoma44.3NRNRNRNRNRNRJones RL201770-0None71.4NRNRNRNRNRNRKim HJ2017351(3)LMS29LMS60NRNRNRNRNRNRStacchiotti S2018301(3.3)ASPS27ASPS83NRNRNRNRNRNRFrezza AM2018180-0None50NRNRNRNRNRNRKim M201960-16.7ASPS100NRNRNRNRNRNRSunar V2019280-14.3LMS75NRNRNRNRNRNRStacchiotti S2019260-18Extraskeletal myxoid chondrosarcoma91NRNRNRNRNRNRMartin-Broto J2019360-6Malignant solitary fibrous tumour66NRNRNRNRNRNRToulmonde M2019720-37Desmoid tumours96NRNRNRNRNRNRSeto T20191231(0.8)LGFMS10.6Angiosarcoma, dedifferentiated liposarcoma, LMS, pleomorphic liposarcoma, pleomorphic rhabdomyosarcoma, LGFMS38.2NRNRNRNRNRNRFrezza AM2019128Intimal sarcoma42NRNRNRNRNRNRHirbe AC2020561(1.8)LMS8.9UPS, SS, LMS39.2NRNRNRNRNRNRGrunwald V20201201(1.2)NR12.3NR62.91.000.65–1.53NR1.080.68–1.720.735Martin-Broto J2020340-6Typical solitary fibrous tumours100NRNRNRNRNRNRAggerholm-Pedersen N2020190-32Bone sarcoma (not otherwise specified)69NRNRNRNRNRNRNishida Y2020120-25MPNST50NRNRNRNRNRNROh CR20203470-15.6LMS, UPS, angiosarcoma, SS, MPNST, solitary fibrous tumor, ASPS, rhabdomyosarcoma, epithelioid sarcoma, endometrial stromal sarcoma, pulmonary arterial sarcoma, clear cell sarcoma, sclerosing epithelioid fibrosarcoma, fibrosarcoma54.8NRNRNRNRNRNRChow W2020470-2Chondrosarcoma66NRNRNRNRNRNRHalim NA2020150-0None13.3NRNRNRNRNRNRLiu J2020311(3.2)ASPS35.5ASPS90.3NRNRNRNRNRNRSchmoll HJ2021860-5NR470.580.36–0.920.020.980.60–1.580.83Kataria B2021330-27NR70NRNRNRNRNRNRPark C2021240-16.7AngiosarcomaNRNRNRNRNRNRNRAlshamsan B2021450-20NR55.5NRNRNRNRNRNRFrezza AM2021120-0None25NRNRNRNRNRNRJones RL20221140-13NRNR0.980.52–1.840.950.790.41–1.510.47Frankel P2022120-8Osteosarcoma50NRNRNRNRNRNRThiebaud JA2022290-3Angiosarcoma48NRNRNRNRNRNRHong JY2023180-12.5LMS, SS62.5NRNRNRNRNRNRGiani C2024360-33LGFMS, SEF, Hybrid-LGFMS/SEF58.3NRNRNRNRNRNRVincenzi B202419640-NRLMS, UPS, SS,angiosarcoma, malignant solitary fibrous tumor, MPNST, fibrosarcoma, myxofibrosarcoma,epithelioid sarcoma, pleomorphic rhabdomyosarcoma, MFH, epithelioid HE, DSRCT, clear cell sarcoma, ASPS, other (not specified)NRNRNRNRNRNRNRSöylemez CM2024810-18.8SS, pleomorphic sarcoma, LMS, ASPS, MPNST, fibrosarcoma, angiosarcoma, chondrosarcoma, Ewing sarcoma, epitheloid sarcoma, HE46.3NRNRNRNRNRNRBurkhard-Meier A2025130-0HE85NRNRNRNRNRNREcker N2025990-14LMS, SS, myxofibrosarcoma, fibrosarcoma, liposarcoma, UPS, myofibroblastic sarcoma, pleiomorphic sarcoma, rhabdomyosarcoma, angiosarcoma, clear cell sarcoma, epithlioid sarcoma, epithelioid HE, follicular dendritic cell sarcoma, MPNST, spindle cell sarcoma, undifferentiated uterus sarcoma.40.45NRNRNRNRNRNRASPS: Alveolar Soft Part Sarcoma; CR: complete response; HE: hemangioendothelioma; LGFMS: Low-Grade FibroMyxoid Sarcoma; LMS: Leiomyosarcoma; MFH: Malignant Fibrous Histiocytoma; SS: Synovial Sarcoma; MPNST: Malignant Peripheral Nerve Sheath Tumor; SEF: Sclerosing Epithelioid Fibrosarcoma; UPS: Undifferentiated Pleomorphic Sarcoma. *(Complete and Partial Responses) According to RECIST v1.1 criteria: **HRs as reported in comparative trials were considered (studies reporting HRs derived solely from prognostic models, multivariate analyses, or subgroup analyses were excluded)
Fig. 2. Forest plot showing the mean response rate (RR) for each histotype across studies. Horizontal gray lines represent the standard deviation (SD), where available; for histotypes with only a single data point, only the point estimate is shown. In studies including multiple histotypes, histotype-specific denominators (i.e., the number of responders within a histotype divided by the number of patients with that histotype) were not consistently reported. Therefore, to ensure methodological consistency and enable comparisons across studies, all RRs were calculated using the total study sample size as the denominator. While this approach may underestimate the true histotype-specific RR, particularly for histotypes representing a small fraction of the study population, it offers a conservative and uniform method that facilitates reliable cross-study comparisons
Toxicity and compliance to pazopanib
A comprehensive analysis of toxicities associated with various treatments across multiple studies was performed, focusing on dose reductions, treatment interruptions, and the most common grade III-IV toxicities. The results are summarized in Table 5. The proportion of patients who required dose reductions due to toxicity varied significantly from 23% [17, 19] to 60% [46]. The incidence of treatment interruptions due to toxicity also exhibited considerable variability. Notably, Frezza et al. [49] reported a 100% treatment interruption rate, with other high rates observed in Jones et al. [46] at 94% and Nishida et al. [36] at 66.6%. However, these studies did not clearly distinguish the causes of treatment interruptions, such as disease progression, toxicity, patient choice, or other factors. In contrast, significantly lower interruption rates were reported by Burkhard-Meier et al. [54], Martin-Broto et al. [29], and Sleijfer et al. [17] at 0%, 3%, and 6%, respectively. The median duration of treatment also varied across studies. The longest median treatment duration was observed at 12 cycles in ASPS [24], and at 16.4 weeks in advanced non-adipocitic STS [8]. The most common grade III-IV toxicities observed across the studies demonstrated significant variability. Hypertension was the most frequently reported toxicity, followed by liver function test abnormalities (LFTA). Other commonly observed toxicities included diarrhea, neutropenia, and fatigue. Some studies [30, 38] lacked sufficient data on dose reductions or treatment interruptions, highlighting the heterogeneity in reporting across trials.5
Table 5. Toxicity and compliance associated with pazopanib in the analyzed studiesFirst authorYear% of patients who experienced dose-reduction for toxicity% of patients who experienced drug interruption for toxicityMedian duration of treatmentType of three most common grade III-IV toxicitiesSleijfer S2009236NRHepatotoxicity; Cardiac toxicityvan de Graaf WTA2012394916.4 weeksHypertension; Cardiac toxicity; Elevated bilirubinYoo KH201548.82.34.8 cyclesStomatitis; Anemia; DiarrheaMaruzzo M201523154.1 monthsLFTA; Hypertension; HyponatraemiaNakamura T2016NR28.228.7 weksNRKollàr A2017NRNRNRLFTA; Fatigue; NeutropeniaJones RL2017NRNRNRFatigue; LFTA; Elevated blood pressureKim HJ2017NR804 cyclesHypertension; Transaminases elevation; NeutropeniaStacchiotti S2018NR13.312 cyclesHand-foot syndrome; Diarrhea; AnorexiaFrezza AM2018NRNR2 cyclesNRKim M2019NRNR7.5 cyclesFatigue; Hypertension; AnorexiaSunar V2019NR7.15 monthsNRStacchiotti S201930915 cyclesNRMartin-Broto J20192835.5 cyclesNRToulmonde M2019NR8NRNRSeto T2019NRNR3 monthsMucositis; Hand-foot syndrome; Deep vein thrombosisFrezza AM2019NR100NRLFTA; Hypertension; NeutropeniaHirbe AC202019.69NRHypertension; LFTA; DiarrheaGrunwald V*202024.732.13.8 monthsHypertension; Diarrhea; FatigueMartin-Broto J202052848 cyclesDiarrheaAggerholm-Pedersen N20202610NRNRNishida Y20205066.6NRHypertension; Hand-foot syndrome; DiarrheaOh CR202032.6NRNRHypertension; Fatigue; ThrombocytopeniaChow W2020NR26NRNRHalim NA20203326.73 monthsHypertension; LFTA; HyponatremiaLiu J202035.5NRNRHypertension; LFTA; DiarrheaSchmoll HJ*2021NRNRNRLFTA; WBC decrease; Cardiac toxicityKataria B20211221NRDiarrhea; Nausea; VomitingPark C2021NRNRNRLFTA; Hypertension; InfectionAlshamsan B2021316NRNRFrezza AM2021NR91NRLFTAJones RL*20226094**NRHypertension; Pneumothorax; Liver disorderFrankel P2022NR17NRLFTA; Hypertension; NeutropeniaThiebaud JA202210142 cyclesHypertension; Diarrhea; NeutropeniaHong JY2023NRNRNRNRGiani C2024NRNR4 cyclesNRVincenzi B202425.29.63 cyclesNRSöylemez CM20246.11.5NRFatigue; Arrhythmia; PneumothoraxBurkhard-Meier A20252308.8 monthsFatigue; Hypothyroidism; Hair color changesEcker N202539.417.2NRNR (Grade 3 toxicities are grouped with Grade 2; Grade 4 not reported)*The data refer solely to the pazopanib arm. **In these studies, there is no clear distinction among the causes of treatment interruptions, such as disease progression, toxicity, patient choice, or other factors. LFTA: Liver Function Test Abnormalities
Comparative efficacy of pazopanib versus active non-placebo interventions
To determine whether pazopanib offers advantages over other active treatment options, three studies were selected for meta-analysis, assessing the efficacy of pazopanib against non-placebo interventions in various sarcoma types [33, 41, 46]. These studies included a total of 320 patients in the progression-free survival and overall survival analyses. No significant heterogeneity was observed, and the funnel plots indicated a symmetrical distribution among the selected studies (Fig. 3). The Forest Plots for PFS and OS are presented in Fig. 4. The pooled HR for PFS and OS were 1.10 (95% CI: 0.69–1.25) and 0.99 (95% CI: 0.63–1.35), respectively, consistent across both fixed and random-effects models. Notably, these estimates showed similar efficacy compared to alternative interventions considered active to date. (Table 2).
Fig. 3. The left funnel plot depicts the hazard ratios (HR) for Overall Survival (OS), and the right plot shows the hazard ratios (HR) for Progression-Free Survival (PFS). In each plot, individual studies are represented as points plotted against their standard error, with the HR values on the x-axis. Symmetry around the central line indicates the absence of publication bias. Below the plots, results from the Q test, Begg’s test, and Egger’s test are shown. No significant asymmetry is observed in either plot, and all tests for heterogeneity are non-significant, confirming the absence of publication bias
Fig. 4. Forest plots displaying the pooled hazard ratios (HRs) for Progression-Free Survival (PFS) on the left and Overall Survival (OS) on the right, analyzed using both fixed-effects and random-effects models. The weight of each study is indicated alongside the corresponding plot. Arrows indicate the direction of effect, showing a trend toward risk reduction in favor of pazopanib compared to non-placebo interventions
Discussion
The results of this systematic review and meta-analysis provide an overview of the efficacy and toxicity of pazopanib in treating sarcomas.
Pazopanib has shown variable efficacy across STS subtypes and treatment settings. Its clinical utility appears greatest in specific histologies such as desmoid tumors and ASPS, where high ORRs and DCRs were consistently observed, up to 37% and 35.5%, respectively. Although rare, complete responses were primarily reported in leiomyosarcoma and ASPS, further supporting the notion that pazopanib, despite its approval for all non-adipocytic STSs, offers greater benefit in selected subtypes. Importantly, responses were also reported in challenging histologies such as malignant peripheral nerve sheath tumors and extraskeletal myxoid chondrosarcoma (Table 4). In contrast, limited or no activity was observed in chondrosarcoma, epithelioid sarcoma, and undifferentiated sarcomas, where ORRs were consistently 0%. Across studies, pazopanib was predominantly evaluated in pre-treated patients, typically in the second-line setting or beyond. Key limitations include heterogeneity in study design, absence of histotype-specific denominators in most reports, inconsistent documentation of DCR and toxicity, and a lack of superiority over other active treatments in comparative trials. Importantly, these negative or modest outcomes should not be uniformly interpreted as evidence of intrinsic biological resistance, but may in part reflect methodological factors that underestimate therapeutic benefit. Collectively, these findings support the use of pazopanib as a relevant option in select STS subtypes, while highlighting its limited or uncertain role in others, emphasizing the need for more histology-driven, prospective investigations.
Assessing radiologic response and, consequently, activity of pazopanib in sarcomas is challenging. Only two studies in this analysis evaluated response using both RECIST and CHOI criteria, while the remaining studies employed RECIST alone. This reliance on RECIST, which primarily captures tumor size reduction, may systematically underestimate the activity of antiangiogenic agents such as pazopanib, as these therapies often induce changes in tumor density, necrosis, or vascularization rather than rapid dimensional shrinkage. In contrast, CHOI criteria account for these changes, offering potential advantages in detecting therapeutic response, particularly in sarcomas, where size changes may not be the sole indicator of treatment efficacy and failure [56, 57]. Thus, some cases of apparent “non-response” may reflect limitations of response assessment rather than true lack of biological activity.
In terms of toxicity, pazopanib was associated with a range of adverse effects, with hypertension being the most frequent, followed by liver function abnormalities, diarrhea, and fatigue. These toxicities, while highlighting the need for careful management and monitoring during treatment to minimize adverse effects, are generally manageable. This is consistent with the existing evidence in scientific literature [58–60].
Placebo-controlled designs are generally considered ethically acceptable when no effective standard therapies are available. However, the expanding landscape of alternative therapeutic options necessitates careful reconsideration of this approach. It is therefore increasingly important to determine whether pazopanib, approved for use in non-adipocytic soft tissue sarcomas from the second-line setting, provides efficacy advantages not only over placebo but also in comparison with other active treatment strategies. In this context, the pooled hazard ratios for progression-free survival and overall survival did not demonstrate a significant advantage of non-placebo interventions over pazopanib. It is noteworthy that pazopanib was not inferior to more aggressive chemotherapy regimens, such as methotrexate-vinblastine in desmoid tumors [30] and doxorubicin in diverse sarcomas [33]. The response rates observed with pazopanib are notably significant, particularly when considering its use beyond the first-line of treatment. This significance is underscored when comparing pazopanib to the outcomes of large randomized studies focused on first-line therapies. In these studies, doxorubicin monotherapy typically yields response rates of around 15%. When combined with ifosfamide, response rates increase to approximately 30%. However, the combination of anthracyclines and ifosfamide is also associated with considerable severe toxicities, including myelosuppression, dose-dependent cardiotoxicity, and mucositis [61, 62]. Notably, the absence of superiority should be interpreted in light of late-line treatment settings, where disease biology and prior resistance mechanisms may confound efficacy estimates and bias results toward underestimation of benefit.
The heterogeneous response to pazopanib across histological subtypes of STS represents a critical challenge highlighted by this study. While the drug shows notable clinical efficacy in specific subtypes such as leiomyosarcoma and alveolar soft part sarcoma, many others (including undifferentiated pleomorphic sarcoma and liposarcoma) typically demonstrate only modest benefit. This variability likely reflects the profound biological and molecular heterogeneity that characterizes STSs [63–65]. Each sarcoma subtype harbors distinct oncogenic drivers, patterns of vascularization, and stromal microenvironments that can influence sensitivity to pazopanib. For example, alveolar soft part sarcoma is marked by a high degree of vascularization and a characteristic ASPSCR1-TFE3 fusion, potentially rendering it particularly susceptible to VEGF-targeted agents [66]. In contrast, liposarcomas (especially the well-differentiated and dedifferentiated forms) are generally less vascularized and may not depend heavily on angiogenic pathways, possibly accounting for their reduced responsiveness to pazopanib [67]. Another important limitation contributing to the observed variability in clinical outcomes is the design of many trials, which often do not include stratification based on molecular subgroups. The frequent lack of molecular stratification in clinical trials further complicates interpretation, as biologically distinct entities are often analyzed together, potentially obscuring subtype-specific efficacy signals. A key example is the frequent omission of the distinction between translocation-associated and non-translocation STSs, despite their well-documented differences in molecular architecture and drug sensitivity; this lack of molecular stratification may mask subtype-specific efficacy signals [68].
Taken together, these considerations highlight that the observed heterogeneity in clinical outcomes likely arises from an interplay between true biological resistance and methodological constraints inherent to trial design, response assessment, and patient selection. These considerations highlight the need for innovative and pragmatic trial designs to more accurately assess comparative efficacy in rare and heterogeneous sarcoma populations. Future randomized studies may benefit from basket trial approaches, histology-agnostic but biomarker-driven designs, or the incorporation of well-defined real-world comparators, which could enhance feasibility while preserving clinical relevance. Such strategies may allow more precise identification of patient subsets most likely to benefit from pazopanib and better contextualize its role relative to emerging therapeutic options. To overcome these challenges, future research should first and foremost prioritize the refinement of patient selection through the identification and validation of novel biomarkers predictive of response to pazopanib. Although the evidence is still preliminary, several promising avenues include the use of systemic inflammatory indices (e.g., neutrophil-to-lymphocyte ratio [NLR], platelet-to-lymphocyte ratio [PLR]) [69, 70], the presence of PDGFRA mutations [71], and co-amplifications of PDGFRA, VEGFR2, and KIT [72]. These markers could help establish a molecular rationale for more individualized treatment approaches, ultimately enhancing therapeutic precision and optimizing outcomes in patients most likely to benefit from pazopanib.
Recently, cabozantinib has emerged as a compelling alternative to pazopanib for the treatment of soft tissue and bone sarcomas [73]. Like pazopanib, it is a multi-kinase inhibitor, but it has a broader target profile that includes MET and AXL, which are implicated in tumor invasiveness and resistance mechanisms. This expanded activity spectrum may offer particular advantages in sarcoma subtypes driven by MET signaling, such as osteosarcoma and Ewing sarcoma, which are often refractory to VEGFR inhibitors [74]. In the CABONE phase 2 trial, cabozantinib demonstrated encouraging clinical activity in these settings, with median progression-free survival ranging from 4 to 6 months and disease control rates approaching 60% [75]. Both pazopanib and cabozantinib are orally administered once daily, yet their safety profiles differ. In addition to class-related toxicities such as fatigue, hypertension, and QT prolongation, cabozantinib more frequently induces adverse effects like palmar–plantar erythrodysesthesia and mucositis.
Importantly, both agents have also been evaluated in combination with immune checkpoint inhibitors (ICIs) in STS [76]. This therapeutic strategy is particularly intriguing given their ability to modulate the tumor microenvironment and potentially enhance antitumor immunity. Pazopanib has been shown to attenuate immunosuppressive angiogenic signaling, thereby promoting T-cell infiltration and function [77]. Similarly, cabozantinib has demonstrated immunomodulatory effects, including the reduction of myeloid-derived suppressor cells and regulatory T cells [78]. These properties provide a compelling rationale for combining these agents with PD-1 or CTLA-4 blockade. In a retrospective study, a subset of patients received pazopanib plus nivolumab, with evidence of partial response, especially in histotypes typically less responsive to pazopanib (dedifferentiate chondrosarcoma and epithelioid sarcoma) [79]. In a phase 2 study, the combination of pazopanib with the PD-L1 immune checkpoint inhibitor durvalumab demonstrated unexpectedly meaningful clinical activity in STS subtypes that typically show limited responsiveness to pazopanib monotherapy (desmoplastic small round cell tumour, undifferentiated pleomorphic sarcoma, and malignant peripheral nerve sheath tumour). The overall response rate of 30.4% surpassed the predefined efficacy threshold, and a median PFS of 7.7 months was achieved. Crucially, high intratumoral infiltration by CD20 + B cells, along with increased vessel density, emerged as independent predictors of prolonged PFS and superior clinical outcomes [80]. These findings suggest that the tumor immune microenvironment may play a critical role in mediating response to this therapeutic combination. In line with this synergistic rationale, results from a randomized phase II trial demonstrated that the combination of cabozantinib with dual immune checkpoint inhibition (nivolumab and ipilimumab) significantly improved disease control and PFS in patients with metastatic STS, particularly in leiomyosarcoma. Notably, responses were also observed in angiosarcoma, epithelioid sarcoma, and myxofibrosarcoma [81]. Together, these studies support the emerging paradigm that integrating antiangiogenic agents with immunotherapy may enhance clinical benefit across a broader spectrum of STS subtypes than previously recognized, and underscore the need for biomarker-driven strategies to guide therapeutic decision-making.
Our study has several limitations. The first stems from the methodological heterogeneity of the included studies, which varied widely in design (encompassing both prospective and retrospective approaches) and in sample size, quality scores, and follow-up duration. However, this heterogeneity is multifaceted. For instance, the diversity in patient populations, reflected by a wide age range (26 to 78.7 years) and varying gender distributions, underscores the inherently heterogeneous nature of sarcomas. Furthermore, the inclusion of different histological types, ranging from STSs to osteosarcomas, complicates the evaluation of pazopanib’s efficacy across such a diverse spectrum of tumors. In this context, predefined subgroup analyses by histologic subtype were neither planned nor feasible, given the marked granularity of sarcoma histotypes and the limited number of patients within individual subgroups, which would not have allowed statistically robust or clinically meaningful comparisons. Additional complexity arises from variability in the line of therapy at which pazopanib was administered. Most studies evaluated pazopanib in non-first-line settings (Table 3), a scenario that mirrors real-world clinical practice. However, this approach may underestimate the true efficacy of pazopanib in non-randomized settings, as the drug is often offered to patients with more advanced disease or following prior treatment failures. As a result, the potential therapeutic benefit may be confounded by the disease’s progression stage at the time of treatment initiation.
Second, although the hazard ratios for PFS and OS suggest that pazopanib may be a viable alternative to more intensive therapeutic strategies, the limited availability of time-to-outcome data (combined with substantial heterogeneities) limits the strength of any conclusions regarding its long-term efficacy. Therefore, even in the absence of significant statistical heterogeneity, the paucity of data warrants caution in interpreting the pooled HRs.
A third limitation involves methodological variability in toxicity assessment. Notably, discrepancies in dose reduction and treatment interruption rates likely reflect not only true differences in pazopanib tolerability across histological subtypes but also variability in treatment protocols and adverse event reporting practices. High rates of treatment discontinuation reported in some studies [46, 49] were influenced by factors beyond toxicity, including disease progression or patient preference. Future studies should clearly differentiate the reasons for treatment interruption to better assess the role of toxicity in treatment adherence.
Our results underscore that pazopanib is not uniformly effective across STS subtypes, despite its broad regulatory approval. Its most meaningful benefit appears confined to select histologies where both ORRs and DCRs are consistently high. This suggests that pazopanib should not be considered a default option for all non-adipocytic sarcomas, but rather integrated into histology-driven treatment algorithms. Clinically, this means reserving pazopanib for subtypes where angiogenesis plays a central role or where other systemic options are limited. Furthermore, our findings emphasize that pazopanib’s efficacy in pretreated populations compares favorably to other non-placebo interventions, despite its oral administration and generally manageable toxicity. This is particularly relevant in frail patients or those for whom cytotoxic chemotherapy is contraindicated. Thus, pazopanib serves not only as a bridging therapy but also as a viable alternative in specific second- or third-line settings. However, the variability in radiologic response and toxicity reporting across studies underscores the need for standardization in evaluating targeted therapies. The limited use of CHOI criteria, for example, may have led to underestimation of benefit in certain subtypes. Clinicians should be aware that traditional RECIST assessments might not fully reflect biological activity, particularly in vascular sarcomas. Finally, the integration of pazopanib with immunotherapy, and its potential predictive markers such as CD20 + B cell infiltration, suggests a future paradigm shift toward combination strategies. This approach holds promise for expanding pazopanib’s utility beyond traditionally responsive subtypes and warrants further clinical exploration.
Conclusions
Pazopanib remains an important therapeutic option for previously treated, non-adipocytic soft tissue sarcomas, offering consistent disease stabilization across several histologies despite modest objective response rates. Its efficacy appears particularly notable in selected subtypes such as alveolar soft part sarcoma, desmoid tumors, and solitary fibrous tumors. Toxicity is frequent and often necessitates dose modifications, underscoring the need for careful clinical monitoring and optimized management strategies. Further research is essential to identify specific patient subgroups that may derive greater benefit from pazopanib and to explore potential biomarkers that could predict treatment response. This continued investigation will be crucial for refining therapeutic allocation, improving risk–benefit balance, and ultimately enhancing outcomes for patients with advanced sarcomas.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sunar V, Korkmaz V, Akin S, Can Guven D, Arik Z, Ates O, Yilmaz M, Mutlu Meydanli M, Oksuzoglu B. Efficacy of pazopanib in patients with metastatic uterine sarcoma: a multi-institutional study. J BUON. 2019;24(6):2327–32.31983102 · pubmed ↗
- 2Stacchiotti S, Ferrari S, Redondo A, Hindi N, Palmerini E, Vaz Salgado MA, Frezza AM, Casali PG, Gutierrez A, Lopez-Pousa A, Grignani G, Italiano A, Le Cesne A, Dumont S, Blay JY, Penel N, Bernabeu D, de Alava E, Karanian M, Morosi C, Brich S, Dagrada GP, Vallacchi V, Castelli C, Brenca M, Racanelli D, Maestro R, Collini P, Cruz J, Martin-Broto J. Pazopanib for treatment of advanced extraskeletal myxoid chondrosarcoma: a multicentre, single-arm, phase 2 trial. Lancet Oncol. 2019;20(9):1252–1262. · doi ↗ · pubmed ↗