Augmented and virtual reality in dental and oral and maxillofacial surgery education: a systematic review with a taxonomy of training technologies
Mathias Maes, Jasper Deferme Van Gerven, Robin Willaert, Reinhilde Jacobs

TL;DR
This paper reviews how augmented and virtual reality can improve dental and surgical training by offering safe, repeatable practice and better learning outcomes.
Contribution
The study introduces a taxonomy of AR/VR training tools and evaluates their effectiveness in dental and maxillofacial surgery education.
Findings
AR/VR tools showed equal or better outcomes than traditional training in preparation accuracy and diagnostic precision.
Most studies reported low risk of bias, indicating reliable evidence for AR/VR effectiveness.
User confidence improved with AR/VR training, though some studies found no significant advantage over conventional methods.
Abstract
The use of augmented reality (AR) and virtual reality (VR) in surgical training has increased significantly. Trainees in skill-intensive specialties such as dentistry and oral and maxillofacial surgery (OMFS) highly depend on treating real life cases under supervision. This old apprentice model is challenged by reduced learning opportunities and patient safety questions. AR and VR training can create alternative learning opportunities and intricate skill acquisition by simulating scenarios, providing real-time feedback and repetitive practice without patient risk. This systematic review aims to evaluate the effectiveness and usability of AR/VR tools in surgical skills training and provides a clear overview of the available systems. In accordance with the PRISMA-SR guidelines, different databases were searched for studies published between April 2015 and 2025. Different AR and VR tools…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
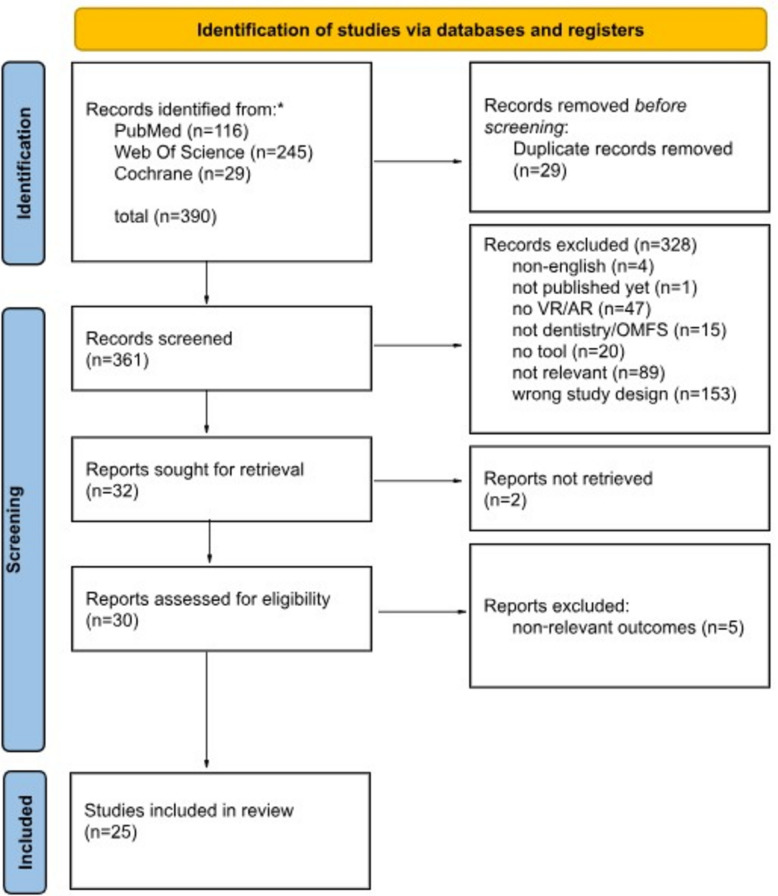 Figure 1
Figure 1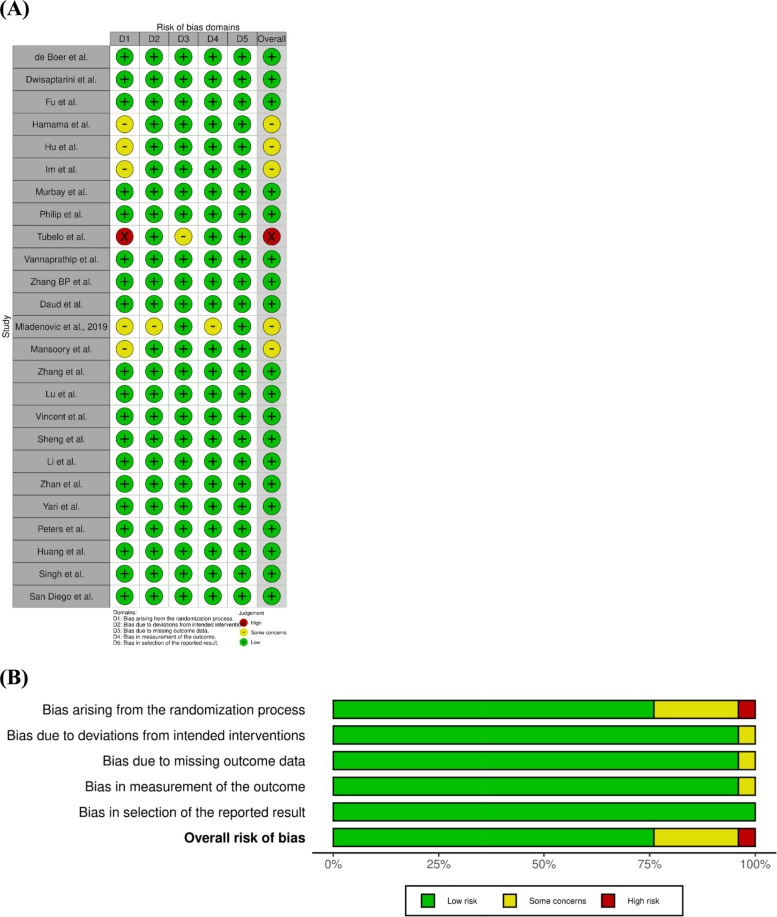 Figure 2
Figure 2 Figure 3
Figure 3- —Karolinska Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Dental Research and COVID-19 · Augmented Reality Applications
Introduction
Virtual reality (VR) and augmented reality (AR) are increasingly used in surgical education. They provide immersive environments for knowledge acquisition and skill development. VR places the learner in a fully computer-generated environment, typically via a head-mounted display. AR overlays digital information onto the real world, often via smart glasses, smartphones, or tablets. Haptic interfaces (e.g., gloves or controllers) can be used in both VR and AR to deliver tactile feedback through vibration, force, or resistance and to improve interaction with virtual objects.
Dentistry and oral and maxillofacial surgery (OMFS) training require complex knowledge and fine motor skills within limited timeframes, which is challenging for novice learners [1]. Training traditionally relies on supervised practice with real patients. This model is increasingly constrained by workload, time pressure, and patient-safety considerations, which reduce hands-on learning opportunities [2–4]. VR and AR tools are currently being used to effectively replicate operating room scenarios, provide real-time feedback, and allow repetitive practice without patient risk [5]. Applications already span preoperative planning, implantology training, and restorative dentistry [6–8].
Within OMFS, AR has been reported since 1995 and is now applied across several domains. Orthognathic surgery and dental implantology remain prominent areas, with growing use in head and neck oncologic resection and reconstruction. AR-based teaching tools also support visualization of complex anatomy [9]. In head and neck oncology, AR navigation can overlay tumor margins and critical structures intraoperatively [10]. In implantology, dynamic navigation has been associated with improved placement accuracy compared with freehand techniques, supporting novice performance [11]. Mixed-reality systems in orthognathic contexts have been linked to improved planning accuracy, reduced intraoperative time, and enhanced trainee knowledge and technical skills [12].
Extended reality (XR) technologies have been associated with improved procedural accuracy and efficiency in surgical education [13–15]. Beyond performance metrics, VR-based learning has been linked to higher motivation, enjoyment, confidence, and post-intervention knowledge gains [16–19]. High-fidelity XR platforms may enable simulation of rare procedures, support robotic-assisted training, and facilitate remote mentorship [20, 21]. Cost-effectiveness has been suggested, with lower per-trainee costs than cadaveric or animal-laboratory sessions, although initial investment can be substantial [22–24].
Despite increasing implementation, evidence on whether AR and VR training improves objective technical performance compared with conventional methods in dental and OMFS education remains fragmented [25, 26].
This systematic review aimed to determine whether AR- and VR-based training improves objective educational performance compared with conventional teaching methods in dental and OMFS education. Given the heterogeneity of training tasks and assessment methods, the primary outcome was defined as the main performance-based educational endpoint prespecified by each randomized controlled trial, typically reflecting objectively assessed technical skill, procedural accuracy, error rates, or task-specific competence, as summarized in Table 2. Secondary aims were to evaluate effects on learner-related outcomes, including knowledge acquisition and retention, self-efficacy, confidence, cognitive load, and user satisfaction, and to examine differences in educational effectiveness across AR/VR tool categories.
Methods
Protocol and registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [27] and was registered on the Open Science Framework (OSF). To enhance transparency, the study protocol was prospectively uploaded to OSF (10.17605/OSF.IO/CXKSA).
Eligibility criteria
- Population (P): Undergraduate dental students, postgraduate residents and fellows in dentistry and OMFS.
- Intervention (I): AR or VR-based training tools.
- Comparator (C): Traditional training (didactic, cadaver labs, non-AR/VR simulators).
- Outcomes (O):
- Primary outcomes were objective, performance-based measures of surgical skill (e.g., accuracy, error rates, procedural quality or time).
- Secondary outcomes included knowledge retention and learner-reported measures such as confidence or satisfaction.
Study design
Randomized controlled trials, including parallel-group, cluster-randomized, and crossover designs, published in English between January 2015 and April 2025 were included. We restricted inclusion to RCTs to maximize internal validity when comparing AR/VR training with conventional methods.
Exclusion criteria
Non-randomized study designs, including quasi-randomized trials or controlled trials without true random allocation, were excluded; pre–post studies without a parallel control group were excluded by design; non-educational applications of AR/VR; studies not involving dental or OMFS learners; interventions without an AR/VR/XR component; studies in which no objective, performance-based primary outcome was assessed; studies evaluating only secondary outcomes such as learner confidence, perceptions, or satisfaction without an objectively measurable clinical skill outcome; secondary literature (reviews, editorials); conference abstracts or records without full text; non-human studies; and publications outside the predefined language and date limits.
Databases and search criteria
A systematic search was conducted in PubMed, the Cochrane Library, and Web of Science on 15 June 2025. The search combined controlled vocabulary terms (MeSH, where applicable) and free-text keywords related to immersive technologies, education, and the clinical domain. Boolean operators were consistently applied, using OR to combine synonyms within the same concept and AND to link different conceptual domains. The key terms were combined as follows: (‘virtual reality’ OR ‘augmented reality’ OR ‘mixed reality’ OR ‘extended reality’ OR ‘VR’ OR ‘AR’ OR ‘XR’) AND (‘dental education’ OR ‘dentistry’ OR ‘education’ OR ‘training’ OR ‘simulation’) AND (‘oral surgery’ OR ‘oral and maxillofacial surgery’). Search strategies were tailored to the indexing system of each database. The complete search strategies for each database are presented in Table 1.Table 1. Overview of the search strategies per databaseDatabaseSearch Terms UsedRecords IdentifiedCochrane Library(“Virtual Reality” OR “Augmented Reality”) AND (“Education” OR "Training") AND (“Surgery, Oral” OR “Dentistry” OR "OMFS" OR "Maxillofacial")29PubMed("Virtual Reality"[MeSH] OR "Augmented Reality"[MeSH] OR "Simulation Training"[Mesh] OR “VR” OR “AR” OR "virtual reality" OR "augmented reality" OR “Simulation” OR “Simulator”) AND (("Education, Dental"[MeSH] OR "Surgery, Oral/education"[MeSH] OR "dental education" OR "oral surgery education" OR "maxillofacial surgery education") OR ((“Education”[MeSH] OR “education” OR “training”) AND (“Dentistry”[MeSH] OR “Surgery, Oral”[MeSH] OR “dentistry” OR “OMFS” OR “maxillofacial” OR “oral surgery”)))116Web of ScienceTS = (("Virtual Reality" OR "Augmented Reality") AND ("Education" OR "Training") AND ("Oral Surgery" OR "Dentistry" OR "Maxillofacial" OR "OMFS"))245
Searches were limited to English-language publications published between January 2015 and June 2025, with results restricted to randomized controlled trials using database filters. Grey literature sources, including conference proceedings, theses, and preprints, were not searched. Reference lists of all included full-text articles were manually screened; however, no additional randomized controlled trials meeting the predefined eligibility criteria were identified.
Data collection process
Study selection and screening procedures are summarized in the PRISMA flow diagram (Fig. 1). Two reviewers independently screened titles and abstracts for eligibility. Inter-reviewer agreement was high (Cohen’s κ = 0.86). Discrepancies were resolved through discussion until consensus was reached.Fig. 1PRISMA flowchart
Data extraction and taxonomy
Data extraction was performed independently by two reviewers using a standardized extraction form. The extraction form was pilot tested on a subset of included studies and refined accordingly prior to full data extraction. Discrepancies were resolved through discussion until consensus was reached.
For each included study, core study characteristics and outcomes were extracted (Table 2). In addition, details of the AR/VR training technologies were systematically classified to establish a taxonomy of educational interventions evaluated in the included trials. Extracted variables included device type (e.g., head-mounted displays, haptic simulators, software-based platforms), commercial availability, hardware and software components, fidelity characteristics (visual, haptic, and/or auditory), and the targeted training scenario. This taxonomy is presented in Tables 3, 4 and 5.Table 2. Characteristics of the included studies according to tool performanceStudy (Author, Year)Simulator (Type)DesignPopulationPrimary OutcomeSecondary OutcomePrimary resultDaud A et al., 2023 [28]VRHS (haptic VR)2-arm crossover23 Year-3 dental studentsQuality of Class I cavity preparations (VRHS haptic simulator vs phantom-head training)Learner satisfaction and perceived realismNo statistically significant differencede Boer IR et al., 2017 [29]Simodont (haptic VR)Crossover RCT101 dental studentsCavity preparation performance and learner satisfaction (Simodont haptic VR simulator with force-feedback vs no force-feedback)Student satisfaction and perceived usefulnessFavours AR/VRDwisaptarini AP et al., 2018 Visuo-tactile VR task2-arm RCT32 Year-6 dental studentsMinimally invasive caries removal accuracy (visuo-tactile VR simulation vs conventional model)Not reportedNo statistically significant differenceFu J et al., 2024 [30]UniDental (haptic VR)3-arm RCT108 dental studentsResidual calculus amount and overall scaling performance score (ultrasonic scaling training, haptic VR)Student perceptions of realism, usability, and learning effectivenessFavours AR/VRHamama H et al., 2024 [31]Haptic VR cariology simulator2-arm crossover RCT76 dental studentsCaries removal knowledge and lesion detection accuracy (haptic VR cariology training)Self-confidence, perceived learning benefitNo statistically significant differenceHu J et al., 2025 [32]REP-VS (interactive VR)2-arm RCT123 Year-4 dental studentsRegenerative endodontics theory exam and practical procedure scores (interactive VR pulp regeneration simulation)Learning motivation, satisfactionFavours AR/VRHuang S et al., 2023ChatGPT-assisted VR2-arm RCT187 dental studentsClinical procedure performance score (ChatGPT-assisted immersive VR)Motivation, self-efficacy, cognitive loadFavours AR/VRIm JE et al., 20243D VR (Oculus Quest 2)2-arm RCT79 dental hygiene studentsUser-experience rating (immersion/usability for 3D intraoral radiography VR vs 360° video)Usability, satisfactionFavours AR/VRLi Y et al., 2025 [33]VR simulators (Unidental & Simodont)Hybrid RCT≈30 Year-4 dental studentsVeneer preparation quality (Unidental/Simodont VR vs phantom-head training)Perceived realism, educational value, satisfactionNo statistically significant differenceLu J et al., 2023Virtual simulation platform (pulpotomy)2-arm RCT199 Year-4 dental studentsPulpotomy theoretical exam and operative skill score (virtual simulation experimental platform)Not reportedFavours AR/VRMansoory MS et al., 2022 [34]3D VR (Gear VR)2-arm RCT50 dental studentsNeutral-zone design knowledge test score and learner satisfaction (Gear VR mixed reality)Learner perceptions and confidenceFavours AR/VR Mladenovic et al., 2019 [35]Mobile augmented reality (AR) simulator (smartphone app)Randomized controlled trial41 Year-4 and 5 dental studentsInferior alveolar nerve block knowledge/skill (post-training questionnaire)Procedure time and anesthesia success rateFavours AR/VRMurbay S et al., 2020 [36]Simodont (haptic VR)2-arm RCT32 Year-2 dental studentsClass I/II cavity preparation accuracy (Simodont haptic VR vs phantom-head training)Not reportedFavours AR/VRPeters P et al., 2024HMD-based immersive VR3-arm RCT101 novice studentsSurgical suturing OSATS score and self-assessed competence (HMD VR simulation vs e-learning)Cognitive load, confidenceNo statistically significant differencePhilip N et al., 2023 [37]SIMtoCARE Dente (haptic VR)2-arm RCT14 Year-4 dental studentsPulpotomy access outline and chamber deroofing quality (SIMtoCARE Dente haptic VR vs conventional)Student perceptions, satisfaction, confidenceNo statistically significant differenceSan Diego JP et al., 2022 [38]Haptic VR (visuo-tactile)Cluster RCT64 Year-1 dental studentsCavity preparation quality and instrument handling (Simodont haptic VR vs phantom-head)Not reportedNo statistically significant differenceSheng J et al., 2022 [39]UniDental (haptic VR)2-arm RCT38 Year-3 dental studentsInlay tooth preparation accuracy (virtual VR simulation vs jaw model training)Student attitudes toward learning modalityFavours hybrid armSingh V et al., 2024 [40]Immersive VR simulation2-arm RCT60 Year-3 dental studentsOverall clinical skill performance score (immersive VR training vs conventional)Student confidenceFavours AR/VRTubelo RA et al., 2016 [41]Virtual learning objectCluster RCT46 dental studentsZinc phosphate cement (ZPC) theoretical knowledge and manipulation skill score (virtual learning object vs traditional)Not reportedFavours AR/VRVannaprathip N et al., 2020 [42]SDMentor (haptic VR)2-arm RCT36 Year-5 dental studentsAccuracy of endodontic access decision-making (SDMentor VR intelligent tutor vs control)Cognitive workload, situational awarenessFavours AR/VRVincent M et al., 2020 [43]Virteasy (haptic VR)2-arm RCT88 Year-1 dental studentsClass I cavity preparation accuracy (Virteasy haptic VR vs phantom training)Not reportedNo statistically significant differenceYari A et al., 2023AR book2-arm RCT40 dental studentsInferior alveolar nerve block skill score and learner concentration (AR book vs traditional text)Learner satisfactionFavours AR/VRZhan Y et al., 2022Dynamic navigation (AR)Pilot RCT6 senior dental studentsImplant placement accuracy (augmented-reality dynamic navigation vs freehand)Self-confidenceFavours AR/VRZhang BP et al., 2020 [44]UniDental (haptic VR)Multi arm RCT80 OMFS studentsImplant placement accuracy and operative performance (haptic VR simulation vs hybrid training)Theoretical knowledge testFavours hybrid armZhang J et al., 2021 [45]Virtual simulation platform (periodontology)4-arm RCT60 dental studentsPeriodontal instrument debridement skill and knowledge score (periodontology VR simulation vs jaw model)Student feedback and perceived learning valueFavours hybrid armAbbreviations: Augmented Reality (AR); Virtual Reality (VR); Randomized Controlled Trial (RCT); Oral and Maxillofacial Surgery (OMFS)Table 3. Taxonomy of Haptic simulator devicesToolArticleAR/VRSpecializationObjectiveRegion of InterestAvailibilitySetupVisual QualityHaptic FeedbackTracking AccuracyAnatomical RealismEase of UsePerformance AnalysisScenario DiversityNO NAMEDwisaptarini et al., 2018 [46]VROMFSTraining and performing visual surgical planning in OMFSVR operates on a 2.8-GHz Pentium 4 PC, with 256 MB RAM; 2 Omni haptic devices13-inch computer monitorNot reportedHigh – Based on 3D micro-CTs of 10 extracted permanent molars with deep carious lesionsNot reportedParticipants were assessed by experts and scoredNot reportedUniDental VS SystemFu et al., 2024 [30]VROMFSImprove teaching ultrasonic scaling techniqueMain tower with tools and functional interface3D mixed reality display system, through the observation window or by wearing headsetsNot reportedHigh – Based on 3D scan with smartphone and intraoral scan to make custom or patient specific training casesModerate – Introductory guidance neededCompared to traditional group and quail egg; significantly higherCustom training cases and patient specific casesUnidental V1.0Li et al., 2025 [33]VRDentistryDental veneer tooth preparationNot reported2D displayHigh – Soft tissue force feedbackModerate – Lacks gingival dynamics, salivary flow, tongue mobility, etcNot directly stated – Mentions technical issues and need for recalibrationEvaluated using a 100-point rubric; includes marginal integrity, depth, contour, smoothnessAllows practice on different tooth positions and complex casesSimodont Dental TrainerLi et al., 2025; de Boer et al., 2017; Hamama et al., 2024; Murbay et al., 2020 [29, 31, 33, 36]VRDentistryDental veneer tooth preparation; Effect of force feedback (FFB) on performance and satisfaction; Detect and treat caries; Operative dentistry proceduresHaptic handpiece, 3D display, virtual drill, simulated tooth blockIncludes 3D vision and adjustable zoomModerate – Precise tracking of drill position and pressure, better force feedback for tooth preparation; lacks soft tissue feedbackHigh – Provides realistic visualization and tactile experience; includes tissue-specific hardness and visual cues; lacks gingival dynamics, salivary flow, tongue mobility, etcHigh – Students preferred working with FFB; some fatigue noted; occasional technical issues and need for recalibrationDetailed analysis using a 100-point rubric; Collected metrics on student performance; Self-assessment, detailed digital analysis of cavity prep (depth, width, centering, smoothness)Allows practice on different tooth positions and complex cases, different difficulty levels availableSIMtoCARE DentePhilip et al., 2023; Daud et al., 2023 [28, 37]VRDentistryPulpotomy procedures; Cavity preparation and caries removalPhysical handpiece (stylus) and dental mirror with virtual display on monitorNot reportedNot reportedHigh – Visual realism rated high by 72% of students; based on scanned extracted teeth, with caries texture simulation; tactile sensations moderate (difficult to distinguish enamel/dentine)Moderate – Students noted differences in grip, weight, and manoeuverability vs. real tools; lack of finger rests and lag when navigating imagesTracks procedural steps, quality scores, time taken and instructor prompts; time spent, percentage of structure removed, deviation from taskMultiple exercises and procedures with difficult complexity; focused on Class I cavity preparation and caries removalhapTELSan Diego et al., 2022 [38]VRDentistryDental cavity preparation and caries removal3D glasses, haptic device with handpiece and mirrorNot reportedModerate – Tracks handpiece angulation and movement)Moderate – 3D virtual teeth with layered structureLow – Perceived as harder to use than phantom headScoring rubric, tutor observation, statistical analysisDifferent tasks with varying difficulty and tooth positionsUniDental-MU01Sheng et al., 2022 [39]VRDentistryProsthodonticsComputer based systemNot reportedNot reportedHigh – Includes extracted teeth and scanned models for evaluationNot reportedIncludes theoretical and practical scores, scanned tooth forms, and Likert-scale feedbackFocused on inlay preparation on premolarsSDMentorVannaprathip et al., 2025 [42]VRDentistrySurgical decision making in dentistry (root canal treatment)HTC Vive Pro Eye headset, Geo-Magic Touch haptic devices2880 × 1600 resolution, stereoscopic 3DHigh – Uses collision detection and symbolic action recognitionHigh – Based on micro-CT scans of real teethNot directly stated – Requires VR headset and haptic devicesLogs actions, evaluates decisions, tracks learning progressSupports multiple intraoperative stages; customizable scenariosVirteasyVincent et al., 2020 [43]VRDentistry (restorative)Cavity preparationWindows 7 PC, touchscreen, 3D stereoscopic glasses, Geomagic Touch X haptic device, foot pedal3D stereoscopic display (Estar America ESG6100 glasses)High – Simulator records % inside/outside target, drilling time, etcHigh – Includes realistic tooth models and cavity shapes (e.g., Black’s Class II)Not directly stated – Students received demonstrations and briefingsObjective metrics (e.g., % inside/outside, time), subjective scoring by instructorsFocused on Class II cavity with mesial and prophylactic extensionsImages of tooth, bone, soft tissue, academic, commercial, yes and no (freepik.com and Lucide.dev, November 2025)TeethBoneSoft tissueAcademicCommercialYesNoAbbreviations: Augmented Reality (AR); Virtual Reality (VR); Oral and Maxillofacial Surgery (OMFS); Force Feedback (FFB); Cone Beam Computed Tomography (CBCT)Table 4. Taxonomy of Head-mounted devicesToolArticleAR/VRSpecializationObjectiveRegion of InterestAvailibilitySetupVisual QualityHaptic FeedbackTracking AccuracyAnatomical RealismEase of UsePerformance AnalysisScenario Diversity3DOVR-DR Im et al., 2025 [47]VRDental RadiographyDental radiography proceduresOculus Quest 2 with controllerNot reportedNot reportedHigh – Realistic visual modellingHigh – Commercially available deviceErrors indicated with visual cuesIncludes different teeth & different procedural stepsNO NAME Mansoory et al., 2022 [34]VRDentistryProsthodontics – neutral zone and teeth arrangementGear VR headset (Samsung), smartphone, Unity-based app, 3D cube navigationUses 3D cube with multi-angle videoNot reportedModerate – Based on multi-angle video capture of real proceduresMixed – Some confusion and incompatibility with glasses notedPre-/posttests and practical skill checklistsFocused on neutral zone and teeth arrangementNO NAME Peters et al., 2023 [48]VRDentistry & MedicineSurgical suturingOculus Quest 2Not reportedNot reportedLow – Low-fidelity model usedMixed – Generally positive; some discomfort notedOptical flow, number of suturesNot reportedImages of tooth, bone, soft tissue, academic, commercial, yes and no (freepik.com and Lucide.dev, November 2025)Teeth Bone Soft tissueAcademic Commercial Yes NoAbbreviations: Augmented Reality (AR); Virtual Reality (VR); Oral and Maxillofacial Surgery (OMFS); Force Feedback (FFB); Cone Beam Computed Tomography (CBCT)Table 5. Taxonomy of softwareToolArticleAR/VRSpecializationObjectiveRegion of InterestAvailibilitySetupVisual QualityHaptic FeedbackTracking AccuracyAnatomical RealismEase of UsePerformance AnalysisScenario DiversityREPs-VS platform Hu et al. 2025 [32]VRDentistryTeach regenerative endodontic proceduresWeb-based platform, PC/mobileNot reportedNot reportedModerate – Good visual and operational realism but lacks tactile precisionHigh – Software is accessible from multiple devices; no physical device or weight concernsStudy hours, progress, and masteryVirtual patient with complex scenarios and gamification elementsZhonghui Huang et al. 2025 [49]VRDentistryOperative dentistry proceduresNot reportedDesktop-based VR (not headset)Not reportedNot reportedNot reportedNot reportedAutomated scoring, eye-tracking, questionnairesNot reportedNO NAME Lu et al., 2022 [50]VRDentistry (pediatric)PulpotomyComputer-based; no headset or physical device mentionedNot reportedNot reportedModerate – Simulates clinical environment and procedures; lacks full anatomical diversityHigh – accessible anytime, repeatable, interactiveIncludes learning tracking, scoring, and retrospective analysisFocused on specific clinical scenarios (pulpotomy)Dental Simulator Mladenovic et al., 2019 [35]ARDentistryImprove Inferior Alveolar Nerve Block (IANB) learningMobile device + AR mode + VR goggles + plastic jaw modelNot reportedNot reportedModerate – AR overlays on plastic jaw model; improved visualization of reference pointsHigh – positive student feedbackQuestionnaire + time measurement + success rateSingle scenario: Inferior Alveolar Nerve BlockNO NAMESinghet al., 2024VRDentistryClinical skills and confidenceDesktop-based VRNot reportedNot reportedNot reportedNot reportedStandardized checklist, real-time feedback, confidence questionnaireMultiple clinical scenarios availableVirtual Learning Object (VLO) Tubelo et al., 2016 [41]VRDentistryDental materials (Zinc Phosphate Cement) manipulationLaptop or desktop computerNot reportedNot reportedLow – Focus on material manipulation, not anatomyHigh – Survey showed high acceptance (84.6% rated “very frequently”)Automatic scoring in simulation; pre/post theoretical tests + lab tests (film thickness, setting time)Single scenario: Zinc Phosphate Cement manipulationZappar Yari et al., 2024 [51]ARDentistryLocal anaesthesiaSmartphone or tablet (no headset)Not reportedNot reportedHigh – Based on Sobotta Atlas, 3D models of head anatomyModerate – Smartphone-based, no mention of weight/ergonomicsWritten exam, practical score, injection timeNot reportedDynamic navigation system Zhan et al., 2021 [52]VRDentistryDental implant placement (dynamic navigation vs. traditional freehand)Computer monitor, stereoscopic camera, handpiece with tagsReal-time video feedback; no specific resolution, refresh rate, or field of view statedHigh – Real-time tracking of drill and jaw position; deviation measured in 3DModerate – Simulated model with radiographic markers; not full soft tissue simulationHigh – Students rated ease of use highly (mean score 9.1); no mention of weight or ergonomics3D deviation at implant platform/apex and axis; statistical analysis of improvementSingle implant site (maxillary left first molar); no mention of varied casesUniDental-MS01 Zhang et al., 2020 [44]VROMFSPreclinical implant trainingComputer based systemNot reportedNot reportedModerate – Simulates implant site and procedureModerate – Students found it engaging but not superior alineTheoretical scores, implant accuracyMandibular molar implant onlyUniDental Zhang et al., 2021 [45]VRDentistryPeriodontology—supragingival scaling and periodontal examinationVR system (UniDental), possibly with headset and controllersNot reportedNot reportedModerate – Includes periodontal structures and proceduresModerate – Students reported high satisfactionTheoretical exams, operation scores, plaque index, satisfaction surveyIncludes periodontal probing, supragingival scaling, oral hygiene instructionImages of tooth, bone, soft tissue, academic, commercial, yes and no (freepik.com and Lucide.dev, November 2025)Teeth Bone Soft tissueAcademic Commercial Yes NoAbbreviations: Augmented Reality (AR); Virtual Reality (VR); Oral and Maxillofacial Surgery (OMFS); Force Feedback (FFB); Cone Beam Computed Tomography (CBCT)
Risk of bias detection
Two reviewers independently assessed the risk of bias and methodological quality. For RCTs, the Cochrane RoB 2 tool [53] was used. Disagreements were resolved by consensus. The results were summarized in tables and considered in the interpretation of the evidence.
Results
Study selection
The systematic search initially identified 390 records, from which 29 duplicates were removed, yielding 361 unique records for screening. After title and abstract screening, 30 full-text articles were assessed for eligibility, of which 25 randomized controlled trials met all inclusion criteria and were included in this review. The study selection process is detailed in the PRISMA flow diagram (Fig. 1). The included studies are summarized in Table 2. Most trials were conducted in undergraduate dental education, whereas a smaller subset focused on OMFS training (22 studies in general dentistry vs. 3 in OMFS).
Risk of bias for included studies
A risk-of-bias assessment was performed using the Cochrane RoB-2 tool. The overall methodological quality of the included randomized controlled trials was generally favorable. Nineteen of the included studies (76%) were judged to be at low risk of bias. Five studies (20%) were assessed as having some concerns [31, 32, 34, 35, 47]. One study (4%) was judged to be at high risk of bias [41]. The most frequent concerns were related to the randomization process (RoB-2 Domain 1). In contrast, deviations from intended interventions were generally judged to be at low risk of bias. Outcome measurement was also assessed as low risk across most studies. Selective reporting did not emerge as a major source of bias. Despite these limitations, the overall body of evidence can be considered methodologically sound. Nevertheless, the findings should be interpreted with appropriate caution (see Fig. 2).Fig. 2. Risk of bias with the ROB-2 tool. A Traffic light plot; B summary plot
Characteristics of the included studies
For each included RCT, the following data were extracted:
-
Study Characteristics: Publications ranged from 2015 to 2025 (with most after 2020) and were conducted across Europe, Asia, and North America. Geographically, roughly half of the studies were from Asian institutions (e.g., China, South Korea, India, Iran, Thailand), about one-third from Europe (e.g., the UK, Netherlands, France), and the remainder from North America (United States) with one from South America (Brazil). Learner populations were predominantly novice dental trainees, mainly undergraduate dental students (n = 22 studies, 88%) and a smaller number of OMFS residents or surgeons in training (n = 3, 12%).
-
AR/VR Tools: The interventions fell into three broad categories: (a) Haptic simulators (n = 13), such as Simodont, UniDental, SIMtoCARE Dente, and Virteasy, which are high-fidelity VR systems providing force-feedback via haptic devices; (b) Head-mounted displays (HMD) (n = 3), including immersive VR headsets like Oculus Rift and mixed-reality AR glasses like Microsoft HoloLens, offering an interactive 3D visual environment (often without tactile feedback); and (c) Software-based platforms (n = 9), such as mobile AR applications (e.g., AR textbooks), web-based VR modules, or computer-guided navigation systems. These software-based tools typically run on standard computers, tablets, or smartphones without specialized hardware. In terms of reality modality, the vast majority of included studies evaluated VR-based training tools, whereas a minority investigated augmented or mixed-reality approaches. Notably, only two studies (8%) employed AR systems (e.g., an AR anatomy textbook and an AR dynamic navigation system for implant placement), and one study (~4%) utilized a mixed-reality headset (HoloLens), while the remaining ~88% of trials focused on purely VR simulations.
-
Reference standards: The control or comparison groups received traditional training modalities. These included conventional phantom head simulators with plastic teeth, instructor-led didactic teaching or videos, cadaver or model workshops, and other non-AR/VR simulation methods.
-
Performance metrics: Outcome measures encompassed a range of objective technical performance endpoints and subjective learning outcomes. Common primary outcomes were preparation quality scores (e.g. cavity or crown prep grading rubrics), amount of residual errors (such as remaining caries or calculus), procedure completion time, diagnostic or treatment planning accuracy, and for implantology studies, the positional/angular deviation of implant placement. Several studies also assessed secondary outcomes like written exam scores (knowledge retention), learner self-confidence, satisfaction, or other perception questionnaires, to evaluate the educational impact of AR/VR beyond technical skill performance. Detailed characteristics and outcomes for each study are provided in Tables 3, 4 and 5.
Findings of the included studies
Across the included randomized controlled trials, AR/VR interventions were evaluated using three primary technological approaches: haptic simulators, HMDs, and software-based platforms (Tables 2, 3, 4 and 5). Simulation fidelity varied substantially across studies and refers to the extent to which a system reproduces real-world task demands through visual realism, tactile feedback, and procedural interactivity. Because both fidelity and educational design differed markedly between trials, results are reported descriptively by technology type rather than pooled quantitatively.
Haptic simulators were predominantly used to train psychomotor dental skills such as cavity preparation, caries removal, periodontal scaling, veneer or inlay preparation, and restorative procedures. Objective performance outcomes—most commonly preparation accuracy, residual error, or completeness of removal—were superior to conventional training in the majority of trials (Table 2) [28–31, 33, 36–39, 42, 43, 46]. Studies incorporating force-feedback and structured, real-time guidance more frequently reported improvements in accuracy and learning efficiency [29, 30, 42], whereas several trials observed no statistically significant difference between haptic VR and traditional phantom-head training [33, 37, 38, 43, 46]. Differences across trials coincided with variation in the level of guidance, interactivity, and training exposure implemented. Procedural time was inconsistently reported and did not demonstrate a uniform advantage for either approach. Learner confidence and perceived usefulness were more frequently higher in the AR/VR arms. One study suggested that a hybrid sequence combining VR with conventional practice yielded the most favorable outcomes [39].
Head-mounted display–based interventions primarily targeted spatial understanding, anatomy learning, and selected technical skills such as suturing or crown preparation. These trials most often demonstrated improvements in anatomy recognition, spatial orientation, or task execution compared with conventional instruction, alongside consistent gains in learner confidence [34, 47, 48]. In contrast, one HMD study reported no statistically significant difference in objective performance outcomes relative to controls [48]. These neutral findings likely reflect the absence of haptic feedback and the short duration of exposure rather than inferiority of immersive visualization itself. Effects on procedural time were variable and not consistently assessed across studies.
Software-based platforms, including desktop VR environments, web-based simulators, and AR learning objects, were mainly applied to knowledge acquisition, diagnostic reasoning, procedural planning, and selected clinical skills. These interventions generally improved examination scores, diagnostic accuracy, or decision-making performance compared with conventional teaching methods [32, 35, 40, 44, 45, 49–52]. However, effects on hands-on technical accuracy were less consistent than for haptic systems, and a small number of trials reported outcomes comparable to traditional models [45]. This variability reflects substantial differences in software complexity, interactivity, and educational intent, ranging from low-interaction AR overlays to platforms incorporating tracking and structured analytics.
Across all three technology categories, standardized reporting of outcome measures was not feasible. Although outcomes could conceptually be grouped into accuracy, procedural time, learner confidence, and examination or knowledge scores, the specific metrics, scoring systems, tasks, and assessment instruments varied widely between studies. Consequently, results could not be meaningfully harmonized across trials, and synthesis was limited to direction-of-effect reporting within each modality. Despite this heterogeneity, AR/VR interventions were consistently at least as effective as conventional training approaches, with the most robust and reproducible gains observed in objective performance accuracy and learner confidence (Tables 2, 3, 4 and 5).
Discussion
Summary of evidence
The integration of AR and VR technologies in surgical training, particularly within dentistry and OMFS, highlights promising advancements in skill acquisition, learner satisfaction, and innovative educational methods.
As highlighted by Serrano et al., the immersive nature of VR, particularly through advanced simulation tools such as the Simodont Dental Trainer, significantly contributes to refining theoretical knowledge and technical skills among trainees in a safe environment [47]. This aligns with broader findings by Dalanon et al., who reported that the use of AR and VR technologies enhances procedural familiarity, resulting in improved learner engagement and satisfaction as these modalities allow for risk-free practice [54]. The review of the current literature supports the argument that AR/VR contributes positively to the educational experiences of surgical trainees. Trainers and trainees frequently value the ability for instant feedback and practice in risk-free environments. The potential of these tools to increase motivation, enthusiasm, and self-confidence also emphasizes their value as educational tools [55, 56].
Clinical translation
An essential aspect of evaluating AR and VR training lies in the transferability of acquired skills to real clinical environments. Evidence indicates that competencies acquired through immersive simulation, such as hand–eye coordination, spatial awareness, and decision-making, translate effectively to improved performance, accuracy, and confidence in the operating room [15, 20]. Haptic VR simulators in particular strengthen psychomotor control and procedural fluidity, enabling learners to reproduce clinically relevant manoeuvres with greater consistency [8, 15]. Within OMFS, AR systems that support intraoperative guidance and preoperative planning exemplify how virtual training environments can bridge the gap between simulation and real surgery [8, 26]. These tools facilitate continuous rehearsal and reflection, encouraging a shift from isolated technical skill acquisition towards integrated procedural understanding. This holistic approach positions AR and VR not only as adjuncts for training but also as components of a digital surgical ecosystem. It allows for planning, connection of diagnostics, execution, and postoperative evaluation, therefore fostering competency-based learning and improved patient centred care [26, 57, 58].
Beyond indirect impact, virtual reality technology can have benefits for patients in a direct manner as well. Different VR tools suggest to be effective in reducing anxiety before dental treatment [59]. Although studied in verious patient populations, the application of VR as a distractive tool has been mainly used in pediatric patients. It has been proven to alleviate anxiety and pain, resulting in a more positive attitude towards dental procedures. This finally results in overall shorter procedures and improved patient satisfaction [60].
Notably, orthognathic and oncologic surgeries in OMFS have begun to adopt AR and VR for enhanced planning and intraoperative guidance. On the one hand, AR-based navigation in orthographic surgery can overlay virtual osteotomy lines to streamline execution [61]. In head and neck oncology, however, recent studies have demonstrated that AR guidance can significantly increase the precision of tumor resection by clearly delineating surgical margins in real time [21]. Although these applications are still emerging in OMFS, implementations of this type of surgery have achieved success in other surgical fields. In urologic surgery, for example, AR overlays combined with AI-driven planning have already been used to revolutionize procedure planning and intraoperative accuracy. This finding indicates a promising future where similar AI-supported AR navigation could enhance safety and precision [62, 63]. In implant dentistry, computer-assisted guidance, particularly dynamic navigation, consistently improves placement accuracy and attenuates the novice–expert performance gap [11, 64]. Building on this, AI-enabled “virtual-patient” generation from cone beam CT (CBCT)/intraoral scanner (IOS) (automated segmentation with prosthetically driven planning) can be exported one-to-one to dynamic navigation for real-time, plan-concordant execution, enabling a plan–simulate–navigate training loop [65, 66].
Barriers and implementation factors
The implementation possibilities of these AR and VR tools are highly variable, ranging from software to head-mounted devices with haptic feedback. On the one hand, high variability causes heterogeneity in study results and complicates comparisons across different platforms, making it difficult to choose the right tools from such a broad range. On the other hand, their distinct adaptivity allows universities and hospitals to invest in tools that fit their needs and curriculum, resulting in more profitable implementation [46].
Despite multiple implementation possibilities, there is a lack of generalized application due to multiple adoption barriers. Foremost, few data concerning cost-effectiveness are available. Although favourable cost-analyses in other specialties have been published, a high initial cost is a remaining implementation barrier [67]. Second, there are logistical challenges, including the need for dedicated rooms, specialized hardware, and technical support. However, a recent review on the adoption of haptic-enhanced VR training reported that 66% of the schools that bought a VR simulator would recommend this training to other schools [68].
Limitations
Notwithstanding the encouraging advancements in AR/VR applications, methodological heterogeneity and the prevalence of small sample sizes in existing studies limit the generalizability of these findings.
Future directions
Future research on this topic should include long-term RCTs with adequate sample sizes, training protocols, standardized outcome measures, and cost-effectiveness analyses. Moreover, these studies should focus not only on skill acquisition but also on user satisfaction.
Conclusion
This systematic review shows that augmented reality and virtual reality provide training outcomes that are noninferior and often superior to conventional methods in dentistry and oral and maxillofacial surgery. Across 25 randomized trials, these technologies improved objective procedural performance, spatial understanding, and learner confidence. However, the evidence is limited by heterogeneous study designs, small sample sizes, and a lack of data on long-term skill retention and cost-effectiveness. Although augmented and virtual reality are increasingly integrated into educational curricula and allow safe, flexible skill acquisition, their full educational value will depend on standardized outcome measures, adequately powered multicenter studies, and robust economic evaluations.
Supplementary Information
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kanwal L, Gulzar M, Idrees W, Ikram F, Sukhia RH, Fida M. The application of virtual reality and augmented reality in dentistry - a literature review. JPMA J Pak Med Assoc. 2024;74(4 (Supple-4)):S 126–31.10.47391/JPMA.AKU-9S-1938712420 · doi ↗ · pubmed ↗
- 2Hamama H, Harrison KY, Murbay S. Benefits of using virtual reality in cariology teaching. BMC Med Educ. 2024;24(1):1051.10.1186/s 12909-024-05980-4PMC 1142901339334109 · doi ↗ · pubmed ↗
- 3Philip N, Ali K, Duggal M, Daas H, Nazzal H. Effectiveness and Student Perceptions of Haptic Virtual Reality Simulation Training as an Instructional Tool in Pre-Clinical Paediatric Dentistry: a Pilot Pedagogical Study. 2023 [cited 1 AD Jan 1];20(5). Available from: https://www.cochranelibrary.com/central/doi/. 10.1002/central/CN-02534904/full.10.3390/ijerph 20054226 PMC 1000160136901241 · doi ↗ · pubmed ↗
- 4Vannaprathip N, Haddawy P, Schultheis H, Suebnukarn S. SD Mentor: a virtual reality-based intelligent tutoring system for surgical decision making in dentistry. 2025;162:103092.10.1016/j.artmed.2025.10309240015210 · doi ↗ · pubmed ↗
- 5Rosa A, Ronsivalle V, Fiorillo L, Arcuri C. Different uses of conscious sedation for managing dental anxiety during third-molar extraction: clinical evidence and state of the art. J Craniofac Surg. 2024.10.1097/SCS.000000000001051339207162 · doi ↗ · pubmed ↗
- 6Checcucci E, Veccia A, Puliatti S, De Backer P, Piazza P, Kowalewski KF, et al. Author Correction: Metaverse in surgery - origins and future potential. Nat Rev Urol. 2024.10.1038/s 41585-024-00964-x 39443684 · doi ↗ · pubmed ↗