When Otorrhea Hides Something Unexpected: A Challenging Case Report
Susana Pipa, Liliana Ribeiro, Diogo Portugal, Ana Raquel S Afonso, Bebiana Conde

TL;DR
A rare case of tuberculous otitis media in a Portuguese woman highlights the challenges in diagnosing this condition due to its nonspecific symptoms and delayed detection.
Contribution
This case report emphasizes the importance of considering tuberculosis in chronic otitis media cases with atypical features and unresponsive symptoms.
Findings
Tuberculous otitis media was confirmed through retrospective PCR analysis of ear specimens and bronchoscopy.
The patient showed full recovery after 12 months of antituberculosis therapy.
Early recognition of TOM is crucial to prevent irreversible complications.
Abstract
Tuberculosis remains a major global health concern, predominantly in low and middle-income countries. Tuberculous otitis media (TOM) is a rare form of extrapulmonary tuberculosis, representing a small fraction of tuberculosis and chronic suppurative otitis media cases. The nonspecific and indolent presentation of TOM, besides its rarity, often results in delayed diagnosis, mainly in regions with a low tuberculosis prevalence, with increased risk of irreversible complications. We report a case of TOM in a 36-year-old Portuguese woman with a four-month history of right ear pain, otorrhea, obstruction, and progressive hearing loss. Despite multiple evaluations and empirical antibiotic treatments, symptoms worsened. Otoscopic assessment at our centre revealed chronic necrotizing otitis media with tympanic membrane perforation. Computed tomography demonstrated extensive right-sided mastoid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
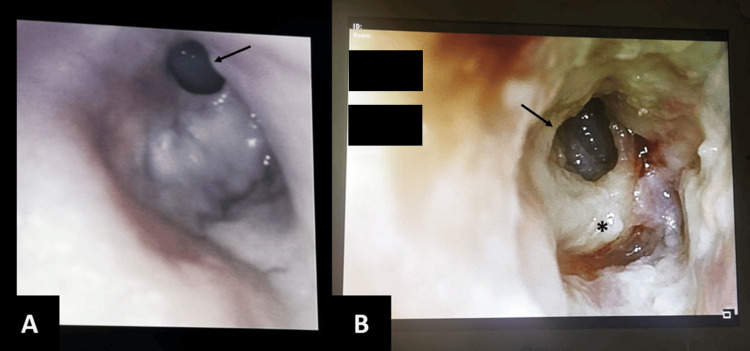 Figure 1
Figure 1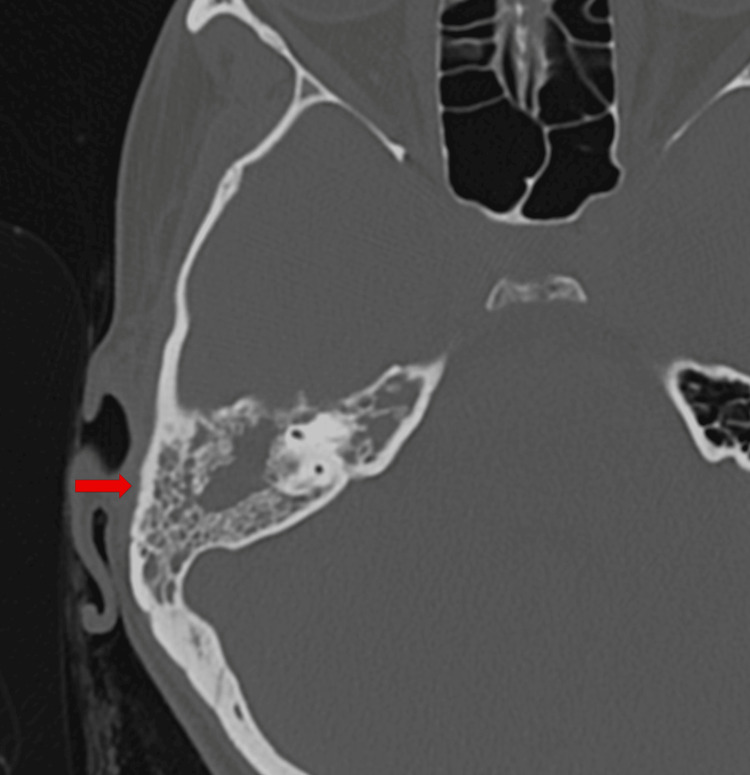 Figure 2
Figure 2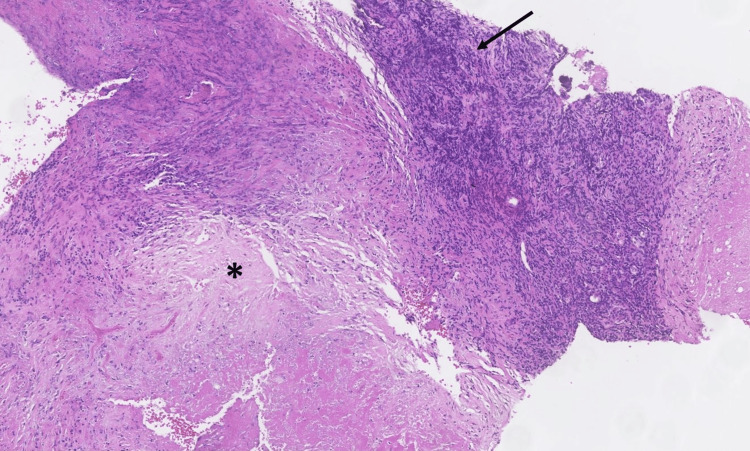 Figure 3
Figure 3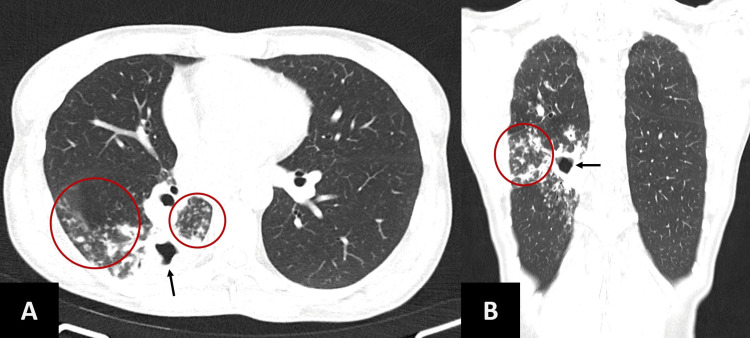 Figure 4
Figure 4 Figure 5
Figure 5| Year/Month | Clinical Events | |
| 2018 | Risk contact with a case of tuberculosis in Thailand; no screening. | |
| 2021 | ||
| March | Initial symptoms: right ear pain and obstruction with hearing loss | Multiple antibiotic courses |
| April | Otoscopy: anterosuperior tympanic perforation | |
| Early July | Otoscopy: evident progression with enlargement of anterosuperior tympanic perforation and necrotic remains of the tympanic membrane | |
| Late July | Otoscopy: multiple tympanic perforations and necrotic remains of the tympanic membrane. Ear CT scan: complete opacification of the mastoid cells, thickening and slight retraction of the tympanic membrane. Audiogram: moderate conductive hearing loss (pure-tone average of 48 dB HL) | |
| Early August | Surgery: mastoidectomy and ossiculoplasty. Histopathologic examination: inflammatory necrotic lesion (granulation and necrotic tissue). No mycobacteriological study of the surgical specimen was performed | |
| Mid August | Irritative cough, weight loss, astheny + chest pain prompted ED evaluation. Chest X-ray showed right hilar opacity. Sputum smear and DNA testing were negative for MTC. Contaminated culture. Empirical amoxicillin/clavulanate and azithromycin | |
| September | Re-aggravation of symptoms prompted a chest CT scan: cavitated lesion in the right lower lobe. Forwarded to pulmonology ED. Acknowledgement of previous risk contact with tuberculosis. Bronchoscopy performed, and bronchial aspirate tested positive for acid-fast bacilli and MTC DNA; no resistance to R or H. Initiated HRZE. Retrospective testing of the surgical specimen: presence of MTC DNA | |
| 2022, March | Otoscopy: neo tympanum viability. Audiometry of the right ear within the normal range (pure-tone average of 19 dB HL) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Ear Surgery and Otitis Media · Ocular Diseases and Behçet’s Syndrome
Introduction
Tuberculosis (TB) remains a major global health concern, responsible for about 1.3 million deaths annually, predominantly in low and middle-income countries [1,2]. Extrapulmonary TB accounts for 15-20% of TB cases [3]. Tuberculous otitis media (TOM) is an extremely rare extrapulmonary TB form, representing only 0.1% of TB cases and 0.04-0.9% of chronic suppurative otitis media [3], although recent studies suggest an incidence of up to 3.6% [4]. It usually follows an indolent course, classically presenting with painless otorrhea and multiple tympanic membrane perforations, though facial nerve palsy, progressive conductive hearing loss and granulation tissue in the middle ear and mastoid are also common features [3,5]. However, chronic otorrhea and tympanic membrane perforation are nonspecific findings shared with chronic suppurative otitis media of more common etiologies, which makes TOM particularly challenging to diagnose [4].
In a retrospective study comparing high-resolution temporal bone CT findings in tuberculous versus non-tuberculous otomastoiditis, no pathognomonic imaging features of TOM were identified. However, the authors concluded that certain radiologic findings may be suggestive of the diagnosis and could aid in early recognition [6]. These include soft-tissue density occupying the entire middle ear cavity, preservation of mastoid air cells without sclerotic changes, mucosal thickening of the bony external auditory canal, and extension of soft tissue into the external auditory canal, without erosion of the scutum.
Histopathological examination remains a reliable diagnostic method, together with microbiological analysis, including mycobacterial culture and molecular techniques, and early detection and appropriate management are determinant for improving outcomes and avoiding disease progression and sequelae [3].
Although some TOM case reports have recently been published, those originate mainly from countries with a high prevalence of TB [5,7]. Recent systematic reviews and European case series confirm the scarcity of TOM reports in Europe, with only isolated cases and small series published over the past 25 years [8,9]. The indolent course of TOM and its rarity in these populations often result in delayed diagnosis and increased risk of irreversible complications, such as permanent hearing loss or facial nerve paralysis [8].
This delayed recognition of TOM in low-prevalence European contexts (mean 13.6 months) makes it important to remind clinicians of this entity [8]. By exposing this clinical case, we intend to emphasize the importance of a detailed epidemiologic anamnesis and the need to consider TB, particularly extrapulmonary TB, in the event of a prolonged, unresponsive infection and granulomatous or necrotizing changes, which may require a high index of suspicion.
This case was previously presented as a poster at the XXIX Northern Congress of Pulmonology and the XXXV Galaico-Duriense Meeting, which occurred between the 24th and 26th of March, 2022.
Case presentation
A 36-year-old Portuguese woman, with a history of allergic rhinitis and sporadic tobacco and inhaled drug use, presented with a four-month history of right ear pain, obstruction, otorrhea, and progressive hearing loss. She had worked in several American and Asian countries in the preceding five years and reported contact with a coworker diagnosed with TB in Thailand, three years earlier, but had never been screened.
Despite evaluation by several otorhinolaryngologists and multiple antibiotic courses, she showed no symptomatic improvement and progressive worsening of the ear alterations over several months (Figures 1A, 1B).
Otoscopy of the right ear. A. The image shows anterosuperior tympanic perforation (arrow) reported in April; B. The image shows evident progression, with enlargement of anterosuperior tympanic perforation (arrow) and necrotic remains of the tympanic membrane () reported in July.*
She was then observed by an otorhinolaryngologist at our centre, who identified chronic necrotising right otitis media, with tympanic perforation in both the anterosuperior and posterior quadrants, as well as necrotic remnants of the tympanic membrane.
Ear CT scan showed complete opacification of the mastoid cells, with partial extension to the mastoid antrum and epitympanum, bilateral pneumatization and opacification of the right petrous apex, partial opacification of the mesotympanum and hypotympanum and thickening and slight retraction of the tympanic membrane, without bone erosion of the ossicular chain, mastoid cortex, or mastoid trabeculae (Figure 2). These imaging findings partially overlap with previously reported CT features suggestive of TOM [6], particularly the extensive soft-tissue involvement of the middle ear with preservation of the ossicular chain and mastoid bone, without evidence of erosion or sclerosis.
Ear CT scan evidencing complete opacification of the right mastoid cells (arrow).CT: computed tomography.
An audiogram evidenced moderate conductive hearing loss in the right ear (pure-tone average of 48 dB HL), and she was promptly submitted to right mastoidectomy and ossiculoplasty.
The histopathological examination of the fragments of the tympanic cavity and mastoid showed flaps of granulation and necrotic tissue, some related to small bone lamellae, compatible with a necrotizing inflammatory lesion (Figure 3).
Histopathological findings from the fragments of tympanic cavity and mastoid (H&E, x10).The image demonstrates flaps of granulation tissue (arrow) and necrotic tissue (), compatible with the origin of a necrotizing inflammatory lesion.*
Two weeks postoperatively, the patient developed a persistent cough, constitutional symptoms with involuntary three-kilogram weight loss and thoracalgia, which prompted clinical evaluation at an emergency department from another hospital. Chest X-ray showed a right hilar opacity, but initial sputum smears and DNA testing were negative for Mycobacterium tuberculosis complex (MTC). She was empirically medicated with amoxicillin/clavulanate and azithromycin for community-acquired pneumonia, with partial improvement at first, but after recurrence of symptoms, a chest CT scan was performed and revealed a cavitated lesion in the upper portion of the right lower lobe (Figures 4A, 4B), raising suspicion for tuberculosis.
Chest CT scan A) Axial view and B) Coronal view.Scans evidencing a cavitated lesion in the upper segment of the right lower lobe (arrows) and ground glass infiltrates around the lesion (circles)CT - Computed tomography
The patient was forwarded to the Pulmonology emergency department. At admission, she was apyretic, without respiratory insufficiency and presenting crackles in the middle third of the right hemithorax at pulmonary auscultation. The sputum culture from the previous evaluation was still being processed at another centre and was later found to be contaminated. Bronchoscopy demonstrated the right bronchial tree globally oedematous, with slight enlargement of the division spurs (Figure 5); aspirate tested positive for acid-fast bacilli and MTC DNA, without rifampicin or isoniazid resistance. HIV testing was negative. First-line quadruple therapy was initiated with rifampicin, isoniazid, ethambutol and pyrazinamide.
Bronchoscopic view of the right bronchial tree. The image demonstrates global mucosal oedema, with slight enlargement of the division spurs. The right main bronchus () and the right upper lobe spur (arrow) are identified.*
Retrospective testing of the surgical specimen confirmed the presence of MTC DNA, establishing TOM with bone involvement (there was no initial mycobacteriological study). Ear evolution was favourable, with neo tympanum viability after six months and significant hearing restoration, with audiometry within the normal range bilaterally (pure-tone average of 19 dB HL on the right ear and 9 DB HL on the left). The patient completed 12 months of therapy with progressive clinical recovery.
In summary, we have a patient with a non-responsive chronic otitis media, with expanding tympanic perforation and necrotizing features. The surgical specimen evidenced granulation and necrotic tissues; however, microbiological analysis was not performed at first. She later developed a cough and systemic constitutional symptoms, which led to both the acknowledgement of previous tuberculosis contact and the diagnosis of cavitated pulmonary tuberculosis. The presence of MTC DNA in the surgical specimen was confirmed only retrospectively, at which point the diagnosis of TOM was established (Table 1).
Discussion
TOM is an uncommon extrapulmonary TB manifestation, particularly in high-income countries. A recent European review confirms that TOM remains a diagnostic challenge due to non-specific symptoms and frequent misdiagnosis as chronic suppurative otitis media. The most common presenting features in European cases are chronic otorrhea (100%), hearing loss (86%), eardrum perforation (44%), ear pain (30%), and facial paralysis (28%). The majority of cases were unilateral (76.7%), although 10 patients (23.3%) presented bilateral disease [8].
Diagnosis is often difficult, especially when otologic symptoms precede pulmonary ones. From the 43 cases identified in this European review, only seven patients were confirmed to have TB disease in other locations [8]. Therefore, direct implantation through the external auditory canal and tympanic membrane should be considered a possible route of spread of TB, and it is crucial to consider TOM even in the absence of other signs of TB. Diagnostic confirmation is most often achieved by biopsy obtained during mastoidectomy (79%), as microbiological cultures and PCR of ear exudate have limited sensitivity and are usually not requested due to low initial suspicion in most cases [8,9].
However, in cases of progressive, unresponsive chronic suppurative otitis media of unclear etiology requiring surgical intervention, microbiological studies, including mycobacterial cultures and MTC DNA, should be performed, as they may allow for earlier diagnosis of TOM. In our case, this approach could have enabled diagnosis approximately one and a half months earlier and initiation of treatment at an earlier stage of the disease. Even in the absence of initial mycobacteriological testing, the presence of necrotizing or granulomatous changes on histopathological examination should prompt consideration of TOM.
In Aguilera-Franco’s review, hearing loss was the most frequent sequela after infection resolution (n=28; 65.12%), while permanent facial paralysis occurred in three patients (6.98%), which, despite the lower incidence, is not negligible due to its severity. Importantly, the risk of sequelae was closely related to diagnostic delay, which ranged from one to 72 months (mean 13.6 months) [8].
In our case, the time from initial symptoms to diagnosis was six months, well below the reported mean [8]. However, this interval might have been shorter with earlier microbiological investigation, or longer in the absence of respiratory symptoms that ultimately raised suspicion of tuberculosis, which illustrates how strongly the diagnostic timeline depends on clinical awareness. Fortunately, our patient recovered without sequelae.
Conclusions
This case highlights the need for heightened clinical suspicion for TOM in patients with chronic or atypical otitis media unresponsive to conventional therapy, particularly if necrotizing or granulomatous changes are present. Early clinical suspicion, a thorough epidemiological history, and integration of clinical, laboratory, and radiological findings, together with prompt microbiological and histopathological evaluation, are critical for timely diagnosis and optimal management. It holds particular clinical value for two reasons. First, it illustrates disease progression through otoscopic images, which may facilitate recognition in clinical practice. Secondly, it demonstrates the potential utility of surgical specimen re-evaluation in cases with suspicious histopathological features, especially in the absence of an initial microbiological study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO's global tuberculosis report 2022 Lancet Microbe Bagcchi S 04202310.1016/S 2666-5247(22)00359-736521512 · doi ↗ · pubmed ↗
- 2World Tuberculosis Day 2024 theme "yes! we can end TB" can be made a reality through concerted global efforts that advance detection, diagnosis, and treatment of tuberculosis infection and disease Int J Infect Dis Goletti D Al-Abri S Migliori GB 106993141 S 20243845842210.1016/j.ijid.2024.106993 · doi ↗ · pubmed ↗
- 3Tuberculosis of the middle ear: a systematic review Am J Otolaryngol Pai KK Omiunu AO Peddu DK 1035714320223596310610.1016/j.amjoto.2022.103571 · doi ↗ · pubmed ↗
- 4Chronic suppurative otitis media: a prospective descriptive study of the microbiology and antimicrobial susceptibility patterns Otolaryngol Head Neck Surg Suttle TK Els T Toman J 909717120243848295910.1002/ohn.708 · doi ↗ · pubmed ↗
- 5Tuberculous otomastoiditis: a diagnostic dilemma Cureus Yee PM Othman IA 016202410.7759/cureus.71307 PMC 1155246239529760 · doi ↗ · pubmed ↗
- 6Tuberculous otomastoiditis on high-resolution temporal bone CT: comparison with nontuberculous otomastoiditis with and without cholesteatoma AJNR Am J Neuroradiol Rho MH Kim DW Kim SS Sung YS Kwon JS Lee SW 493496282007 https://pmc.ncbi.nlm.nih.gov/articles/PMC 7977825/pdf/0353.pdf 17353320 PMC 7977825 · pubmed ↗
- 7Case Report: a rare case of tuberculous otitis media mimicking chronic suppurative otitis media-an ongoing challenge Front Med (Lausanne) Shu C You T Huang M Xu M Zhang J Peng Z 15210111220254072752610.3389/fmed.2025.1521011 PMC 12301375 · doi ↗ · pubmed ↗
- 8Tuberculous otitis media: a case presentation and review of European literature Rev Esp Quimioter Aguilera-Franco M Franco-Acosta A Yépez-Naranjo AF Rodríguez-Granger J Sampedro A Navarro-Mari JM 5195253620233726544810.37201/req/011.2023 PMC 10586746 · doi ↗ · pubmed ↗