The HEART-GP strategy for ruling out acute coronary syndrome in out-of-hours primary care: a diagnostic accuracy trial protocol
Indra M.B. Melessen, Jelle C.L. Himmelreich, Amy Manten, Edanur Sert, Simone van den Bulk, Tobias N. Bonten, Martijn H. Rutten, Eric P. Moll van Charante, Ralf E. Harskamp

TL;DR
This study tests a new strategy to quickly rule out heart attacks in out-of-hours primary care using a simple blood test and clinical assessment.
Contribution
The HEART-GP strategy combines high-sensitivity troponin testing with clinical evaluation to safely and efficiently rule out acute coronary syndrome in primary care.
Findings
The HEART-GP strategy aims to improve diagnostic safety and reduce emergency department referrals.
The study will compare the strategy's performance against standard care in out-of-hours primary care.
Blinded adjudication ensures unbiased outcome assessment.
Abstract
Acute coronary syndrome (ACS) is a life-threatening condition that requires rapid identification to prevent morbidity and mortality. Differentiating ACS from benign conditions remains difficult in out-of-hours primary care (OOH-PC) settings due to non-specific and overlapping symptom profiles, and limited diagnostic resources. Current guidelines promote a low threshold for emergency department (ED) referral. Despite this cautious approach, ACS cases are still missed. The arrival of high-sensitivity troponin (hs-troponin) point-of-care testing (POCT) may enable safer, faster, and more efficient diagnosis. This multicenter prospective diagnostic accuracy trial evaluates the HEART-GP strategy, combining a single fingerstick hs-troponin test with clinical assessment and optional ECG. Adults (≥18 years) presenting with acute chest pain or discomfort to one of four participating Dutch OOH-PC…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
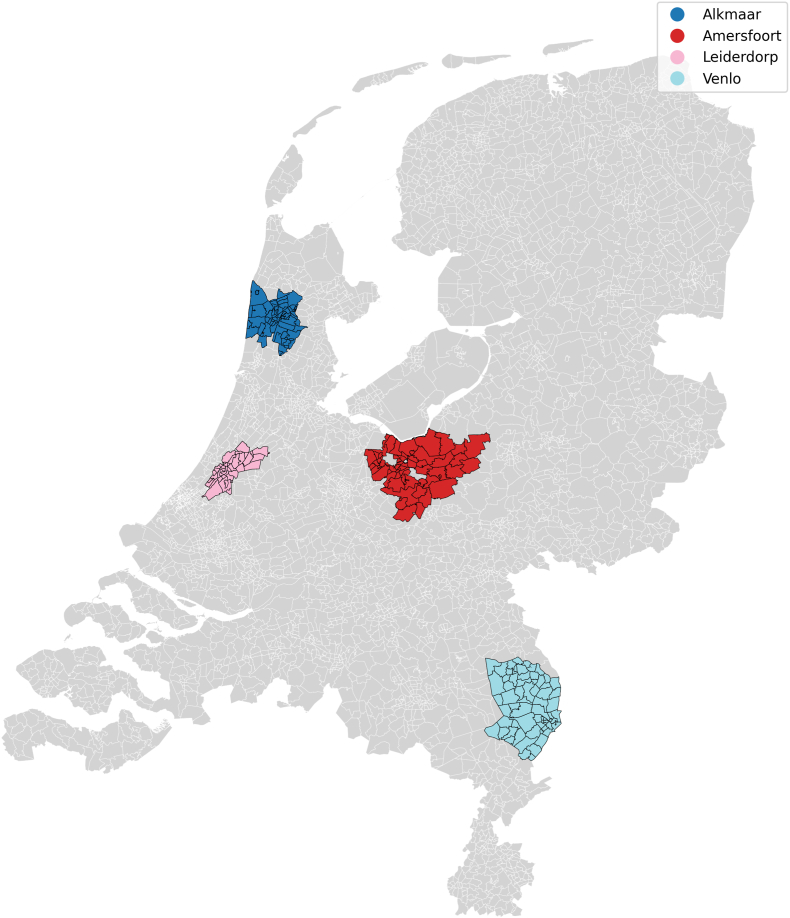 Figure 1
Figure 1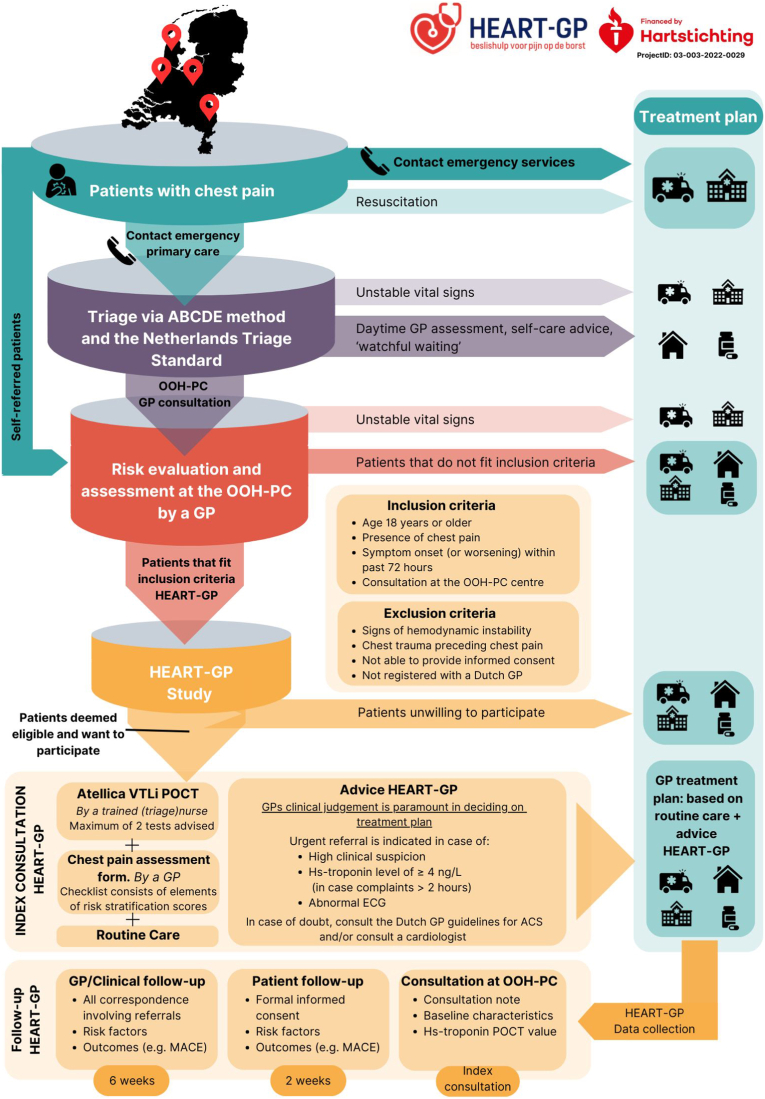 Figure 2
Figure 2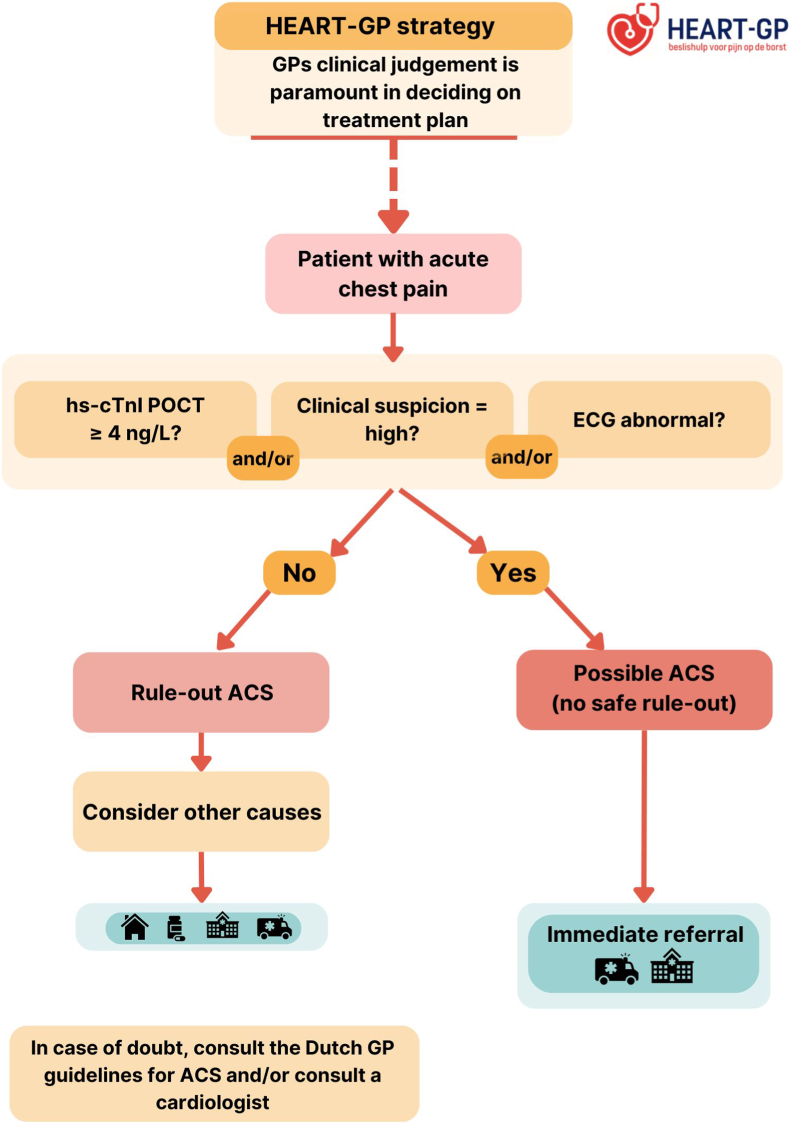 Figure 3
Figure 3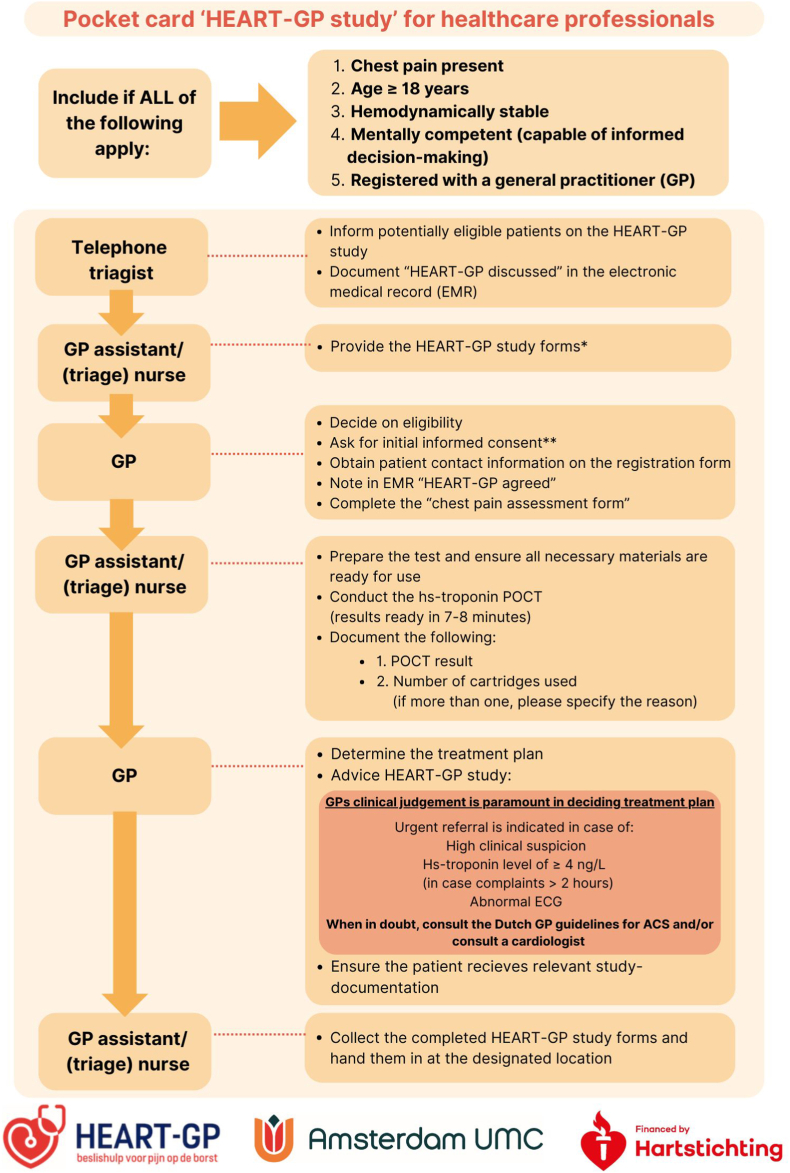 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Health Promotion and Cardiovascular Prevention · Cardiac Health and Mental Health
Introduction
1
Background and rationale
1.1
Acute coronary syndrome (ACS) is a life-threatening condition requiring timely recognition and treatment to prevent severe morbidity and mortality [1]. However its clinical presentation often overlaps with far more common non-cardiac conditions such as musculoskeletal or gastrointestinal disorders [[2], [3], [4]]. The primary diagnostic challenge is to distinguish life-threatening causes, like ACS, from more benign causes. This is particularly pronounced in healthcare systems where general practitioners (GPs) act as the 24/7 first point of contact for urgent care, yet have limited access to reliable diagnostic instruments/tools, such as cardiac troponin testing for detecting myocardial ischemia.
The hallmark symptom for ACS is chest pain, and in Dutch out-of-hours primary care (OOH-PC), GPs annually assess over 160.000 patients with chest pain (i.e. 9 per 1000 inhabitants), representing a substantial share of out-of-hours consultations, as chest pain is in the top 10 of ‘presenting complaints’ [5]. GP assessments rely on clinical judgement, physical examination, and, when available, an electrocardiogram (ECG). These tools may help identify alternative causes for ACS, or confirm ST-elevation, but are insufficient to safely rule out ACS [3]. To minimize the risk of missed ACS, Dutch GP guidelines recommend a low referral threshold [6], and GPs generally adhere to this recommendation, resulting in high referral rates (i.e. 40-70%) for patients with chest pain to the emergency department (ED) [3,7]. This cautious approach increases burden on ambulance services, ED workload, and healthcare costs, while also causing patient distress [8]. Despite high referral rates, 8-19% of ACS cases are initially missed [7,9,10], suggesting that the current assessment strategies in Dutch (OOH-) primary care remain suboptimal, failing to guarantee diagnostic safety while also compromising efficiency.
The development of high-sensitivity troponin (hs-troponin) point-of-care testing (POCT) may constitute a paradigm shift by bringing a rapid, user-friendly and reliable diagnostic rule-out instrument to pre-hospital care. Studies in EDs demonstrated a high diagnostic accuracy of hs-troponin POCT, showing that a single low-level troponin measurement can effectively rule-out ACS [11]. However, these findings may not translate directly to primary care, where ACS prevalence is lower, diagnostic protocols are less standardized, and patient characteristics and work flows differ substantially from hospital settings.
Objectives
1.2
To address this gap, we are conducting a diagnostic trial evaluating a primary care-tailored approach for ruling out ACS in OOH-PC that balances diagnostic safety and efficiency. Our primary objective is to evaluate the diagnostic performance of the HEART-GP strategy, which integrates a single fingerstick-obtained hs-troponin measurement with clinical assessment and an optional ECG, in terms of safety (sensitivity and negative predictive value) and efficiency (reduction in ED referrals) when used in out-of-hours primary care. The primary outcome is major adverse cardiovascular events (MACE), a composite of death, ACS, or urgent revascularization within six weeks of index presentation, reflecting the risk for cardiovascular events rather than a single clinical syndrome.
The secondary objectives are:
- 1.To compare the diagnostic performance (safety and efficiency) of the HEART-GP strategy with current standard care based on (unaided) clinical judgment.
- 2.To evaluate whether using sex-specific versus universal hs-troponin cut-off values improves safety and/or efficiency.
- 3.To assess whether embedding hs-troponin measurements in established clinical risk scores (HEART, INTERCHEST, Marburg Heart Score) further improves diagnostic performance compared to the HEART-GP strategy alone.
Anticipated results
1.3
We anticipate that the HEART-GP strategy will demonstrate improved diagnostic safety along with efficiency gains in OOH-PC. Our straightforward rapid rule-out strategy holds promise to be widely implemented in primary care settings to advance the evaluation of acute chest pain.
Methods
2
This design paper is written according to the Standard for Reporting Diagnostic Accuracy Studies (STARD) 2015 guidelines [12], and according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines on defining standard protocol items for clinical trials [13].
Study design and population
2.1
We designed a prospective diagnostic accuracy trial to evaluate the HEART-GP strategy incorporating point-of-care hs-troponin testing for ruling out MACE in patients presenting with acute chest pain or discomfort in out-of-hours primary care. The trial protocol was prospectively registered in the ISRCTN registry (ISRCTN11954040, https://doi.org/10.1186/ISRCTN11954040) and approved by the CCMO (CIV-NL-22-11-041231, 11-03-2022) and by the Medical Research Ethics Committee of the Amsterdam UMC (NL82428.000.22, 02-03-2023).
Consecutive patient enrollment commenced in March 2023 and has been rolled out since then across four OOH-PC regions in the Netherlands: Alkmaar, Amersfoort, Leiderdorp and Venlo. Together, these regions serve approximately 1 million patients (Fig. 1). Eligible patients are adults (≥18 years) who contact one of the participating OOH-PC centers regarding acute-onset chest pain or discomfort, and are triaged for a face-to-face GP consultation. Patients with signs of hemodynamic instability or chest pain following substantial trauma were excluded since both mandate immediate transfer to the ED and prohibit participation. A complete overview of the trial is displayed in Fig. 2.Fig. 1Healthcare service area of out-of-hours primary care centers in Alkmaar/HONK (253.000 inhabitants), Amersfoort/Eemland (386.000 inhabitants), Leiderdorp/LIMES (90.000 inhabitants) and Venlo/Cohesie (247.000 inhabitants), The Netherlands.Fig. 1. Fig. 2HEART-GP: patient flow, inclusion procedure and follow-upThe upper part depicts the out-of-hours workflow for patients presenting with chest pain within the Dutch healthcare system outside of office hours. The lower part (yellow) outlines the HEART-GP study workflow, including the index consultation and subsequent follow-up procedures.Fig. 2
Study intervention
2.2
HEART-GP strategy incorporating hs-troponin testing (index test)
2.2.1
The intervention involves the HEART-GP strategy (Fig. 3), which combines a single point-of-care high-sensitivity troponin measurement, with clinical assessment and optional ECG. We use the Siemens Atellica VTLi hs-troponin POCT to measure hs-troponin levels from a fingerstick blood sample, which returns results within 8 min. For ethical reasons, the GP is not blinded to the hs-troponin results during the consultation. The specifics of this assay are described elsewhere in further detail, but in essence the whole blood Limit of Detection is 1.6 ng/L and the Limit of Quantitation at 10% CV is 8.9 ng/L [14]. The non-sex specific 99th percentile upper reference limit for this assay is 22.9 ng/L [15]. In our study we applied a lower decision threshold of ≥4 ng/L for rule out purposes, as evidence from prior studies show a sensitivity of 98.8% and a NPV of 99.8% for ruling out ACS in low-risk populations at the emergency department (ED) [11,15].Fig. 3HEART-GP strategyGP: general practitioner, hs-cTnI: high-sensitivity cardiac troponin, POCT: point-of-care test, ACS: acute coronary syndrome.Fig. 3
All (triage) nurses at the participating OOH-PC centers receive standardized training by study personnel to ensure correct execution of the POCT, including sample collection, device operation, and interpretation of results. In the event of a test error, nurses are instructed to repeat the measurement using a maximum of two cartridges. A detailed testing protocol is included in Appendix 1.
The HEART-GP strategy guides decision-making on whether to refer the patient to the (cardiac) ED or manage them in primary care. As part of this strategy, it is of importance to note that the GPs' clinical judgement is paramount in deciding on the treatment plan. For instance, even if a patient's hs-troponin POCT value is below the cut-off of 4 ng/L, based on the discretion of the GP the patient may still be referred.
Symptom assessment form
2.2.2
The treating physician is asked to complete a structured, symptom-based checklist designed to standardize and document clinical assessment. The form includes symptom elements of three risk scores, namely (modified) H(E)ART, INTERCHEST and the Marburg Heart Score (Table 1). In addition, GPs are asked to record their ‘gut feeling/sense of alarm’, as well as whether they would have referred the patient based on their clinical judgement without access to the POCT result. The checklist is completed during the index consultation, instructed to be completed prior to disclosure of troponin result, to ensure unbiased responses. The form contains no recommendations or prompts regarding management decisions.Table 1(Modified) HEART(s), Marburg Heart Score, INTERCHEST risk stratification scores.Table 1(Modified) HEART score [16,17]PointsMarburg Heart Score [18]PointsINTERCHEST [19]PointsHistoryHighly suspicious2Sex/age (Female ≥65, male ≥55 years)Yes1Sex/age (Female ≥65, Male ≥55 years)Yes1Moderately suspicious1No0No0Slightly suspicious0ECGSignificant ST deviation2History of cardio-vascular diseaseYes1History of coronary artery diseaseYes1Non-specific repolarization abnormalities1No0No0Normal0Age≥65 years2Patient assumes the pain is of cardiac originYes1Chest pain related to effortYes145 – 64 years1No0No0<45 years0Risk factorsHistory of atherosclerotic disease or ≥ 3 RF2Pain gets worse with exerciseYes1Pain reproducible by palpationYesMinus 11 – 2 RF1No0No0No known RF0Troponin∗≥23 ng/L (99th percentile)2Pain is not reproducible by palpationYes1Physician initially suspected a serious conditionYes14-23 ng/L1No0No0<4 ng/L0∗Sex-specific HEARTs: sex-specific 99th percentile for troponin (male 27 ng/L, female 18 ng/L) [15]Chest discomfort feels like pressureYes1No0Table 1: ECG: electrocardiogram, RF: risk factors for atherosclerosis, HEART: History, ECG, Age, Risk Factors, Troponin, INTERCHEST: international chest pain prediction.Non-specific repolarization abnormalities: LVH: left ventricular hypertrophy, LBBB: left bundle branch block or PM: pacemaker.Risk factors: Hypertension, Hypercholesterolemia, Diabetes Mellitus, obesity (BMI >30 kg/m2), smoking, positive family history.History of atherosclerotic disease: prior Myocardial Infarction, Transient Ischemic Attack, Cerebrovascular accident, Peripheral Arterial disease or previous Percutaneous Coronary Intervention or Coronary Bypass graft.Textbox 1Out-of-hours primary care in the NetherlandsIn the Dutch healthcare system, GPs serve as round-the-clock gatekeepers to secondary care, except in emergencies requiring immediate ambulance assistance and transport to the ED. OOH-PC centers operate from 17.00 to 08.00 on weekdays and throughout weekends and holidays. They are organized through regional GP cooperatives, serving patients registered with affiliated practices within a defined geographic area (Fig. 1).Upon contact with an OOH-PC center, trained triage nurses, supervised by GPs, conduct telephone triage using the Netherlands Triage Standard (NTS), a standardized, symptom-driven protocol that assigns an urgency level to each case [20]. Although the NTS provides a structured framework, triage nurses or supervising GPs may adjust the final urgency classification based on additional contextual information. This can include the patient's perceived level of distress or whether there were repeated calls for the same symptom within a short timeframe.Patients classified as high urgency are referred directly to the ED without GP assessment. Those with the lowest urgency level receive self-care advice, or are advised to contact their own GP during regular office hours. Patients triaged as intermediate urgency are assessed by a GP at the OOH-PC facility, where they may be treated on-site, referred to the ED for further evaluation, or discharged with appropriate safety-netting advice [21].Alt-text: Textbox 1Textbox 2Why we use major adverse cardiovascular events (MACE)The primary outcome of MACE, a composite of ACS, urgent revascularization, or all-cause death/mortality at 6 weeks follow-up, is an outcome that is patient-centered, objective, and delayed, serving as a suitable reference standard in urgent primary care where not all patients undergo the same in-hospital diagnostic work-up. Using MACE rather than ACS avoids circularity with the index diagnosis and reduces verification bias. It provides a comprehensive and clinically meaningful measure of cardiovascular risk, enhances statistical power, and aligns with established regulatory and methodological standards. All events will be adjudicated with blinding to the index test, with prespecified sensitivity analyses, on the individual components of MACE, performed.Alt-text: Textbox 2
Reference standard (occurrence of MACE)
2.3
We use a delayed-type reference test in which our primary clinical outcome is the occurrence of MACE within 6 weeks from the index consultation (see Textbox 2). A 6-week window was selected to enhance comparability with previous research on MACE after presentation with chest pain in Dutch primary care [22]. MACE is a well-established endpoint accepted by regulatory agencies that captures the overall cardiovascular risk rather than focusing solely on one clinical syndrome. MACE is a composite endpoint, consisting of ACS, urgent coronary revascularization and/or all-cause death. ACS is defined as the occurrence of ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), or unstable angina. Secondary outcomes are (I) the occurrence of (non)fatal myocardial infarction (STEMI or NSTEMI), (II) any hospitalization for a cardiovascular cause (e.g. heart failure, atrial fibrillation, aortic pathology, pulmonary embolism) and (III) all-cause death.
Study flow
2.4
Index contact
2.4.1
The study workflow is described in Fig. 2, Fig. 4. In short, during the consultation the patient receives information about the study's objectives, procedures, potential risks and benefits, and decides on their participation. Upon agreement, initial informed consent is obtained by the treating physician, and hs-troponin POCT is conducted by a trained (triage) nurse. While the POCT runs, the GP completes the ‘chest pain assessment form’. Subsequently, the GP determines the treatment plan ((e.g. discharge with safety-net advice (‘watchful waiting’), consulting a cardiologist or referral to the hospital for further assessment)). At all times, the GP's own clinical judgement serves as the guiding principle in the management following the consultation. For safety reasons, urgent referral is advised in cases of high clinical suspicion of ACS, hs-troponin POCT values ≥ 4 ng/L, and/or an abnormal ECG (if performed), in line with the HEART-GP strategy recommendations. Additionally, GPs are informed to refer all patients with troponin levels exceeding the overall 99th percentile of 22.9 ng/L. Patients who refuse study participation receive routine care only, which focuses on history taking, physical examination and, based on the discretion of the GP, potentially an ECG, as this is not a part of the standard work-up of chest pain in Dutch primary care [6].Fig. 4. Study flow at index consultation∗HEART-GP study forms include the following: pocket card ‘HEART-GP study’ for healthcare professionals, registration form, Chest pain assessment form, Informed consent form, retour envelope, Patient Information Form (PIF) and an accompanying letter.∗∗Initial informed consent is asked during index consultation, the patient is offered the following information beforehand. “This out-of-hours primary care center is conducting research involving patients experiencing ‘chest pain’. As part of the HEART-GP study, you will be asked a few additional questions about your symptoms, and an additional finger-stick test will be performed. This test helps to assess whether further diagnostic evaluation at the hospital may be necessary. Please note: the test does not itself diagnose a heart attack. A result exceeding 4 ng/L*, does not allow for the definitive exclusion of a heart attack. If you agree to participate, the fingerstick test will be conducted and the research team will contact you shortly. They will request your formal informed consent. You may withdraw from the study at any time without consequences. Your personal information will be treated with strict confidentiality.*POCT: point-of-care test, ECG: electrocardiogram, ACS: acute coronary syndrome.Fig. 4
Follow-up contacts and outcome data
2.4.2
Two weeks after the index consultation, research staff will contact participating patients to finalize written informed consent and obtain patient-reported risk factors and outcome data. Furthermore, baseline characteristics, outcome data, and other trial data are prospectively and systematically collected for up to 6 weeks following the index consultation (Fig. 2). Outcome data for all participants, including those lost to follow-up (no follow-up outcomes available), are obtained from medical records at the patients’ general practice and from regional hospital databases. MACE and final diagnoses are adjudicated by an expert panel consisting of two general practitioners with a special interest in cardiovascular care, blinded to troponin POCT results. For verification of MACE and in the event of disagreement, a third independent expert (cardiologist) is consulted.
Data management
2.5
Data are collected using Castor EDC [23], a secure, cloud-based electronic data capture platform with an audit trail. Data is coded, pseudonymized, and stored in accordance with General Data Protection Regulation guidelines to ensure participant confidentiality [24]. To promote data quality and minimize interobserver variability, all assessors received comprehensive training on the study protocol and data entry procedures and Standard Operating Procedures (SOPs) are in place. Quality control measures such as automated range checks are employed to identify and correct discrepancies. Access to the database is restricted to authorized personnel only. Data are handled in accordance with a predefined data management plan, which includes protocols for secure storage, access, and continuous quality monitoring.
Statistical analysis
2.6
Data will be analyzed according to the intention-to-treat principle. Baseline characteristics will be presented as numbers and percentages for categorical variables and as medians with interquartile ranges for non-normally distributed continuous variables. Categorical variables will be compared using Pearson's chi-squared or Fisher's exact test, and continuous variables using the Kruskal–Wallis test. The primary analysis will evaluate the diagnostic performance of the HEART-GP strategy in terms of diagnostic metrics, focusing primarily on safety, defined by sensitivity and negative predictive value for ruling out 6-week MACE, and efficiency, defined as the proportion of patients classified as low-risk. Secondary analyses will compare the diagnostic performance of the HEART-GP strategy with current standard care based on unaided clinical judgment, evaluate whether sex-specific hs-troponin cut-offs improve efficiency without compromising safety, and assess whether incorporating hs-troponin measurements into established clinical risk scores (HEART, INTERCHEST, and Marburg Heart Score) further improves diagnostic accuracy. Discriminatory ability for HEART-GP and comparator scores will be quantified using the area under the receiver operating characteristic curve (AUC). Differences in discriminatory performance will be tested using the DeLong method and the Net Reclassification Improvement (NRI). An exploratory analysis will examine the added value of including ECG findings in a modified HEART score. Missing data will be addressed through multiple imputation to ensure robustness of estimates.
Sample size calculation
2.6.1
Prior ED studies have reported single time-point hs-troponin sensitivities of 97-99% in patients with ≥2 h of symptoms [11]. These sensitivities are considered adequate to safely rule out ACS in primary care [25]. Therefore, we applied a target sensitivity of 98% to calculate the required sample size for our diagnostic accuracy trial, comparing the index test with the reference standard (occurrence of MACE within 6 weeks of the index test). We set a margin of error of 3% around the sensitivity estimate and an alpha of 0.10 (two-sided), reflecting the rule-out focus in primary care. Assuming a MACE prevalence of 7% (literature and historic data range 5-15%), these parameters yield a required 842 participants to ensure adequate statistical power to detect a meaningful diagnostic performance in terms of sensitivity. To account for potential drop-out or a lower event rate, we aim to include at least 900 participants. Sample size calculations were performed following the methods of Akoglu, Bujang and Adnan, and calculated using PASS software [[26], [27], [28]].
Safety and monitoring
2.7
To ensure patient safety, several safeguards are in place. First, hemodynamically unstable patients are excluded from participation. Second, a referral threshold of 4 ng/L is applied (well below the 99th percentile) to minimize the risk of missed cases. Third, internal safety monitoring in complemented by an independent auditing monitor who conducts regular site visits to participating (OOH-PC) centers and performs random inspections of data management procedures. The monitoring body has full excess to the study data at all times. Lastly, an independent Data Safety Monitoring Board (DSMB) has been appointed to oversee patient safety, including monitoring of false negatives and serious adverse events, as well as the adequacy of participant enrollment. Enrollment is continuously monitored at each participating site. If inclusion rates decline, the study team will visit the site to identify barriers and provide support. We will also provide regular updates on recruitment progress with sites, and small incentives are offered upon reaching predefined enrollment milestones.
CRediT authorship contribution statement
Indra M.B. Melessen: Writing – review & editing, Writing – original draft, Visualization, Project administration, Investigation. Jelle C.L. Himmelreich: Writing – review & editing. Amy Manten: Writing – review & editing, Conceptualization. Edanur Sert: Writing – review & editing. Simone van den Bulk: Writing – review & editing, Conceptualization. Tobias N. Bonten: Writing – review & editing. Martijn H. Rutten: Writing – review & editing. Eric P. Moll van Charante: Writing – review & editing. Ralf E. Harskamp: Writing – review & editing, Writing – original draft, Supervision, Methodology, Funding acquisition, Conceptualization.
Patient and public involvement statement
A representative from Harteraad, the patient advisory council for individuals with heart disease, was actively involved in the study design, protocol development, and the creation of patient information materials.
Access to data
Access to the final study dataset will be limited to the principal investigators and designated members of the research team. Any request for access to the dataset or statistical code must be approved by the study's principal investigators and will require a formal data-sharing agreement to ensure data protection and integrity.
Ancillary and post-study care
If participants experience harm related to the study, they will be referred for appropriate medical care, and compensation claims will be handled by the study's insurance, in compliance with Dutch regulations.
Funding
The HEART-GP study project is funded by the Dutch Heart Foundation (project ID: 03-003-2022-0029). Siemens Healthineers (with local support from AxonLab) loanes the Atellica VTLi analyzers, supplies materials at cost, and provides technical support, but has no role in the study design, conduct, or analysis.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: I.M.B. Melessen reports financial support was provided by Netherlands Heart Foundation. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu J.Gale C.P.Hall M.Dondo T.B.Metcalfe E.Oliver G.Editor's choice - impact of initial hospital diagnosis on mortality for acute myocardial infarction: a national cohort study Eur Heart J. Acute Cardiovasc. Care 7220181391482757433310.1177/2048872616661693 PMC 7614828 · doi ↗ · pubmed ↗
- 2Frese T.Mahlmeister J.Heitzer M.Sandholzer H.Chest pain in general practice: Frequency, management, and results of encounter J. Fam. Med. Prim. Care 512016616610.4103/2249-4863.184625 PMC 494315127453845 · doi ↗ · pubmed ↗
- 3Hoorweg B.B.Willemsen R.T.Cleef L.E.Boogaerts T.Buntinx F.Glatz J.F.Frequency of chest pain in primary care, diagnostic tests performed and final diagnoses Heart 103212017172717322863428510.1136/heartjnl-2016-310905 · doi ↗ · pubmed ↗
- 4Bosner S.Becker A.Haasenritter J.Abu Hani M.Keller H.Sonnichsen A.C.Chest pain in primary care: epidemiology and pre-work-up probabilities Eur. J. Gen. Pract.15320091411461988314910.3109/13814780903329528 · doi ↗ · pubmed ↗
- 5Ramerman L.Rijpkema C.Hek K.Beusekom S. van Schmitz J.Elffers B.Baarda E.Verheij R.Hasselaar J.Overbeek L.Zorg via de huisartsenspoedpost. Nivel Zorgregistraties Eerste Lijn: Jaarcijfers 2024 en trendcijfers 2020-20242025 Nivel Utrecht 34
- 6MB.A A. NHG Standaard Acuut Coronair Syndroom 2022
- 7Bruins Slot M.H.Rutten F.H.van der Heijden G.J.Geersing G.J.Glatz J.F.Hoes A.W.Diagnosing acute coronary syndrome in primary care: comparison of the physicians' risk estimation and a clinical decision rule Fam. Pract.28320113233282123947010.1093/fampra/cmq 116 · doi ↗ · pubmed ↗
- 8Bosner S.Haasenritter J.Abu Hani M.Keller H.Sonnichsen A.C.Karatolios K.Accuracy of general practitioners' assessment of chest pain patients for coronary heart disease in primary care: cross-sectional study with follow-up Croat. Med. J.51320102432492056476810.3325//cmj.2010.51.243PMC 2897083 · doi ↗ · pubmed ↗