Thyroid and cortisol endocrinopathies and survival in cancer patients treated with immune checkpoint inhibitors in UAE
Mohamed Alqedra, Bara Fahmayee, Lina Wahba, Jawaher Ansari, Romona D Govender, Saif Al-Shamsi, Raya Almazrouei

TL;DR
This study found that thyroid and cortisol-related side effects in cancer patients treated with immune checkpoint inhibitors are linked to better survival rates.
Contribution
The novel contribution is identifying a favorable survival trend associated with thyroid and cortisol endocrinopathies in ICI-treated cancer patients.
Findings
Thyroid-related events were all post-thyroiditis hypothyroidism, and cortisol-related events were ACTH deficiency.
Patients with endocrinopathies showed improved overall survival compared to those without.
Endocrinopathies occurred most frequently in patients treated with anti–PD-1 agents.
Abstract
Immune checkpoint inhibitors (ICIs) are associated with immune-related adverse events (irAEs) of which endocrinopathies are among the most frequent. This study aimed to identify thyroid and cortisol-related endocrine-related adverse events (ERAEs) in a cohort of patients treated with ICIs and to examine survival differences between patients who developed endocrinopathies and those who did not. We conducted a retrospective review of electronic medical records of adult patients who received ICIs between 2018 and 2023. Data were collected specifically on thyroid and cortisol-related ERAEs. Among 616 patients, 59 (9.6%) developed thyroid or cortisol-related ERAEs. The mean time to onset was 22.7 weeks. All thyroid-related events were post-thyroiditis hypothyroidism (n = 55), while all cortisol-related events were due to adrenocorticotropic hormone (ACTH) deficiency (n = 11). The majority…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
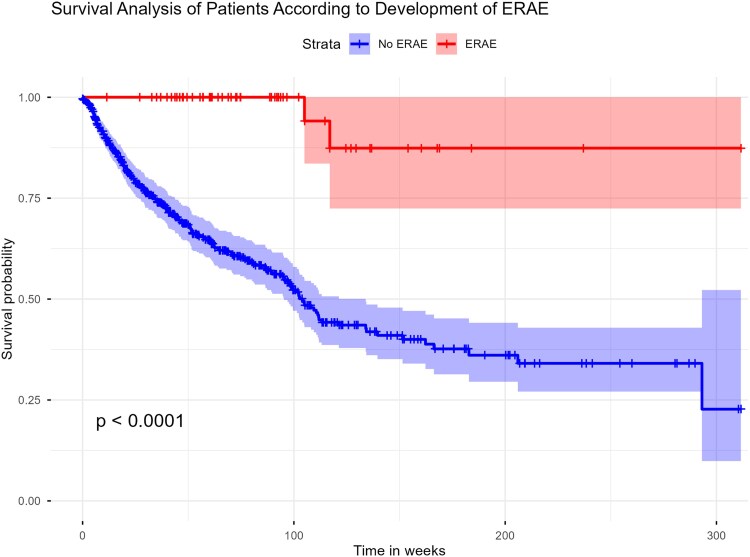 Figure 1
Figure 1| Variable |
|
|---|---|
| Age (SD) | 56.2 (14.0) |
| Gender | |
| Female | 260 (42.2) |
| Male | 356 (57.8) |
| Ethnicity | |
| African | 29 (4.7) |
| Asian | 146 (23.7) |
| Middle East | 335 (54.4) |
| UAE | 97 (15.7) |
| Others | 9 (1.5) |
| Baseline endocrine disease | |
| Nil | 492 (79.9) |
| Graves' disease | 2(0.3) |
| Hypothyroidism | 22 (3.6) |
| DM | 98 (15.9) |
| Hypothyroidism and DM | 2 (0.3) |
| Malignancy type or site | |
| Breast cancer | 64 (10.4) |
| Genitourinary | 97 (15.7) |
| Gastrointestinal tract | 66 (10.7) |
| Gynecological | 69 (11.2) |
| Head and neck | 79 (12.8) |
| Hepatobiliary | 21 (3.4) |
| Lung | 170 (27.6) |
| Lymphoma | 11 (1.8) |
| Melanoma | 26 (4.2) |
| Others | 13 (2.1) |
| Immune checkpoint inhibitor used | |
| Anti CTLA-4 | 19 (3.1) |
| Anti PD-1 | 478 (77.6) |
| Anti PD-1 + anti CTLA-4 | 8 (1.3) |
| Anti PD-L1 | 111 (18.0) |
| Any ERAE, | |
| No | 556 (90.4) |
| Yes | 59 (9.6) |
| ERAE time onset (weeks) | |
| Mean (SD) | 22.7 (15.3) |
| Median (IQR) | 20.0 (22.0) |
| Post thyroiditis hypothyroidism, | |
| Anti CTLA-4 | 4 (7.3) |
| Anti PD-1 | 46 (83.6) |
| Anti PD-1 + anti CTLA-4 | 1 (1.8) |
| Anti PD-L1 | 4 (7.3) |
| ACTH deficiency, | |
| Anti CTLA-4 | 0 (0.0) |
| Anti PD-1 | 8 (72.7) |
| Anti PD-1 + anti CTLA-4 | 2 (18.2) |
| Anti PD-L1 | 1 (9.1) |
| TFT at the time of hypothyroid phase diagnosis, median (IQR) | |
| TSH (mIU/L) | 56 (18.6-138) |
| Free T4 (pmol/L) | 5.4 (1.2-10) |
| ACTH and Cortisol levels at the time of diagnosis, median (IQR) | |
| ACTH (pmole/L) | 0.3 (0.3-1.1) |
| Cortisol (nmol/L) | 15 (3-75) |
| Variables | HR | 95% CI |
|
|---|---|---|---|
| Age at starting of ICPs | 0.99 | 0.97 to 1.01 | .157 |
| Gender (male) | 0.98 | 0.58 to 1.65 | .927 |
| Immune checkpoint inhibitor used | |||
| Anti CTLA-4 | Reference | ||
| Anti PD-1 | 0.62 | 0.22 to 1.73 | .359 |
| Anti PD-1 + anti CTLA-4 | 1.48 | 0.27 to 8.24 | .655 |
| Anti PD-L1 | 0.23 | 0.06 to 0.96 | .043 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Thyroid Cancer Diagnosis and Treatment · Multiple and Secondary Primary Cancers
Immune checkpoint inhibitors (ICIs) have transformed cancer therapy, demonstrating robust response rates and improved survival across several malignancies, including melanoma, renal cell carcinoma, and lung cancer. ICIs are classified into 3 major categories: cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors, programmed cell death protein-1 (PD-1) inhibitors, and programmed death ligand-1 (PD-L1) inhibitors [1]. These agents act by enhancing T-lymphocyte–mediated cytotoxicity and augmenting the adaptive immune response. However, this immune activation also predisposes patients to organ-specific autoimmune toxicities, including endocrine-related adverse events (ERAEs).
Among the most common ERAEs are thyroid dysfunction and anterior pituitary disorders, particularly hypophysitis leading to glucocorticoid deficiency [2]. Less frequently reported endocrine complications include type 1 diabetes mellitus, primary adrenal insufficiency, and hypoparathyroidism [3]. The incidence of ERAEs varies by the type of ICI used, with rates ranging from 12% to 40% [4]. These events typically occur within the first few months of therapy, although delayed onset during or after treatment has also been described [5]. Notably, the development of irAEs has been associated with improved progression-free survival, overall survival, and treatment response [4].
In this study, we report on thyroid and cortisol-related ERAEs among patients treated with ICIs at a tertiary care center in the United Arab Emirates (UAE). We focused specifically on these 2 axes due to robust routine monitoring in our oncology practice. We also evaluated survival outcomes in patients who developed these ERAEs compared to those who did not.
Methods
This retrospective study was conducted at Tawam Hospital, Al Ain, UAE. We identified all patients aged ≥16 years who were prescribed ICIs between 1 January 2018 and 31 March 2023 through oncology pharmacy records. Included ICIs were atezolizumab, durvalumab, nivolumab, pembrolizumab, and the ipilimumab-nivolumab combination. We reviewed medical records to extract demographic and clinical data. The data lock date was 31 July 2024.
Patients were excluded if ICI therapy was not initiated or if they died prior to treatment. All included patients had thyroid function and cortisol levels measured in the morning prior to ICI initiation and before each treatment cycle routinely. Other endocrine tests, such as full pituitary panel or HbA1c, were infrequently performed and thus not analyzed. Consequently, this study reports only on thyroid- and cortisol-related ERAEs. Additionally, pituitary imaging is not performed in our patients and therefore not reported here.
All patients who developed thyroid- or cortisol-related adverse events during immune checkpoint inhibitor therapy were carefully evaluated by certified endocrinologists. Diagnostic work-up followed internationally accepted standards and incorporated biochemical cut-offs, repeat confirmatory measurements, and, when indicated, dynamic assessment with the short Synacthen (cosyntropin) stimulation test [3].
Thyroid ERAEs were defined as new-onset dysfunction after ICI treatment, including central hypothyroidism, primary hypothyroidism (further specified as post-thyroiditis hypothyroidism where applicable), subclinical thyroid dysfunction, and hyperthyroidism. Central hypothyroidism was defined as low free T4 with low or inappropriately normal TSH. Primary hypothyroidism was defined by elevated TSH and low free T4, with review of cases to determine whether hypothyroidism occurred following thyroiditis. Subclinical hypothyroidism was defined as TSH >10 mU/L with normal free T4. Thyroid antibodies were not routinely measured [3].
Adrenal ERAEs were classified as either primary adrenal insufficiency (low cortisol with high adrenocorticotropic hormone [ACTH]) or secondary (central) adrenal insufficiency (low cortisol with low or inappropriately normal ACTH) in the absence of prior steroid exposure. In our cohort, all cases were consistent with secondary adrenal insufficiency. Paired early morning cortisol and ACTH testing was the main diagnostic approach; affected patients showed cortisol concentrations that were low (often <100 nmol/L) with ACTH levels that were inappropriately low or within the lower reference range. When morning cortisol results were indeterminate, repeat testing or Synacthen stimulation was performed to confirm the diagnosis [3]. This structured and standardized approach ensured robust diagnostic accuracy and minimized misclassification of endocrine-related adverse events. All hormone levels were measured using Roche-Cobas Generation II assays. Cancer types were categorized by anatomical site. This study was approved by the Tawam Human Research Ethics Committee (MF20258-2023-937), which waived the requirement for informed consent due to its retrospective nature and anonymized data.
Statistical analysis
Continuous variables are presented as mean ± SD or median with interquartile range; categorical variables as frequencies and percentages. Fisher's exact test was used for categorical comparisons. A Cox proportional hazards model evaluated predictors of ERAEs, including age, sex, and ICI type. Kaplan–Meier survival analysis estimated survival probabilities, and differences between groups were assessed using the log-rank test. Analyses were performed in R version 4.4.1 (The R Foundation, Vienna, Austria). A P-value < .05 was considered statistically significant.
Results
We identified 616 patients who received ICIs. Baseline characteristics are presented in Table 1. The mean age was 56.2 ± 14 years, and 57.8% were male. Patients were primarily from the Middle East (54.4%), followed by Asia (23.7%) and the UAE (15.7%). Pre-existing thyroid disease was present in 26 patients (4.2%), predominantly hypothyroidism (3.9%). Diabetes mellitus was present in 15.9%, including one patient with type 1 diabetes. Lung cancer was the most common malignancy (27.6%).
The most frequently administered ICI was anti-PD-1 (77.6%), followed by anti-PD-L1 (18%). As shown in Table 2, thyroid- and cortisol-related ERAEs were diagnosed in 59 patients (9.6%). Post-thyroiditis hypothyroidism developed in 55/59 patients; no patients developed hyperthyroidism. ACTH deficiency (central adrenal insufficiency) was observed in 11 patients, of whom 7 also had post-thyroiditis hypothyroidism. Most ERAEs occurred in patients receiving anti-PD-1 therapy. Mean time to ERAE onset was 22.7 ± 15.3 weeks overall, 22.3 ± 15.0 weeks for thyroiditis-related hypothyroidism, and 34.0 ± 18.3 weeks for ACTH deficiency. In multivariable analysis (Table 3), use of anti-PD-L1 was the only significant predictor of ERAE development.
Kaplan–Meier survival analysis (Fig. 1) showed significantly better survival among patients with ERAEs compared to those without (log-rank P < .0001). Survival probabilities remained higher over a 312-week follow-up in the ERAE group, whereas the non-ERAE group showed a steeper decline.
Kaplan–Meier survival analysis of patients treated with immune checkpoint inhibitors, stratified by the development of endocrine-related adverse events (ERAEs).
Discussion
This single-center study from the UAE evaluated both thyroid and cortisol-related ERAEs among cancer patients undergoing treatment with ICIs and also explored their association with survival outcomes. The emergence of immune-related adverse events (irAEs), such as thyroid and cortisol-related ERAEs, is not only an anticipated yet challenging aspect of their clinical use, but is also recognized as a potential marker of improved survival outcomes. Patients in this study, who experienced ERAEs, demonstrated a statistically significant higher survival probability compared to those without ERAEs. While similar patterns have been reported globally [6-8], our study provides region-specific insight from the UAE, where such data remain scarce. This contributes valuable context to the Middle Eastern and Gulf literature, where varying rates of ERAEs and survival outcomes suggest regional differences in monitoring practices, treatment regimens, and population characteristics [9-11].
The overall ERAE incidence of 9.6% in this study is comparable to rates reported in large Western datasets and meta-analyses, where endocrine toxicities typically range around 9-13% [4, 12-14], which is notably lower than the rates documented in neighboring Gulf countries: Oman 28% [9], Saudi Arabia 20.85% [10], and Qatar 26.7% [11]. Several factors may explain these differences [9-11]. First, some regional studies included a broader spectrum of endocrine toxicities, such as pituitary dysfunction, diabetes, and gonadal abnormalities whereas our analysis focused specifically on thyroid and cortisol adverse outcomes. Second, the inclusion criteria, as well as differences in screening intensity and diagnostic methods varied; for example, assessment for pituitary hormones or MRI evaluation by some of the centers influenced their results. Third, most of the other studies lack standardized testing protocols for screening potential endocrine adverse effects. Forth, differences in ethnicity, baseline comorbidities, and therapeutic regimens (combination checkpoint blockade vs monotherapy) may all contribute to variability.
Thyroid dysfunction was the most frequent endocrine toxicity in our results, consistent with international and regional data [9, 10, 15]. The majority of cases occurred in patients receiving anti–PD-1 inhibitors, which constituted 77.6% of our treatments. Higher PD-L1 expression in thyroid follicular cells may predispose patients to immune-mediated thyroiditis when treated with these agents [16]. In contrast, ACTH deficiency, observed in 1.79% of our patients, was rare but clinically significant. This lower rate relative to reports among Japanese patients [17] and other cohorts [10] may reflect differences in diagnostic thresholds, imaging frequency, or management protocols. Although pituitary MRI was not routinely performed among our patients, current evidence suggests limited benefit and therefore may not be necessary in most cases of immune checkpoint inhibitor–related hypophysitis or ACTH deficiency [18].
Mean onset of ERAEs in our cohort was approximately 22.7 weeks, similar to previous reports [9]. Prior reports describing ERAEs, documented their development over a wide time frame, averaging between 1 and 2 months [19, 20] and with some events occurring even later [21] highlighting the importance of vigilant hormonal monitoring particularly during the later phases of ICI therapy. The inclusion of cortisol, ACTH, TSH, and free T4 levels at the time of diagnosis strengthens the clinical characterization of these events, facilitating differentiation between primary and secondary etiologies and thus supporting tailored monitoring and management.
Identifying predictive biomarkers for ERAEs remains an ongoing challenge. Although anti–PD-L1 therapy emerged as an independent predictor in our cohort, no biomarker has shown consistent reliability across studies [22]. Future research should integrate longitudinal hormonal assessments, immunologic profiling, and pharmacogenetic data to clarify susceptibility patterns and guide personalized monitoring.
Strengths and limitations
This study's strengths include its extended follow-up period and the implementation of a rigorous protocol for monitoring thyroid hormones and cortisol levels, enabling precise characterization of adverse event patterns. The diverse, real-world patient population enhances the applicability of our findings to similar clinical settings. As retrospective study, it is limited by lack of data on other endocrinopathies due to lack of robust testing and insurance coverage. Additionally, data on non-endocrine adverse events were not collected. Despite these limitations, our results highlight the critical importance of standardized surveillance protocols for early detection and management of endocrine-related adverse events. Educating patients about potential endocrine toxicities—and their potential association with positive treatment outcomes—may improve adherence and support shared decision-making.
Conclusion
In summary, thyroid and cortisol-related ERAEs occurred in 9.6% of cancer patients receiving ICIs in this UAE cohort and were associated with improved survival outcomes. Although the incidence was lower than in neighboring Gulf countries, the findings reinforce the importance of vigilant endocrine monitoring, region-specific reporting, and awareness that these immune-related endocrinopathies may serve not only as adverse effects but also as potential prognostic indicators of treatment efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sanmamed MF, Chen L. A paradigm shift in cancer immunotherapy: from enhancement to normalization. Cell. 2018;175(2):313‐326.30290139 10.1016/j.cell.2018.09.035PMC 6538253 · doi ↗ · pubmed ↗
- 2Kassi E, Angelousi A, Asonitis N, et al Endocrine-related adverse events associated with immune-checkpoint inhibitors in patients with melanoma. Cancer Med. 2019;8(15):6585‐6594.31518074 10.1002/cam 4.2533 PMC 6825974 · doi ↗ · pubmed ↗
- 3Husebye ES, Castinetti F, Criseno S, et al Endocrine-related adverse conditions in patients receiving immune checkpoint inhibition: an ESE clinical practice guideline. Eur J Endocrinol. 2022;187(6):G 1‐G 21.36149449 10.1530/EJE-22-0689 PMC 9641795 · doi ↗ · pubmed ↗
- 4Yang L, Murthy S, Cortellini A, et al Effects of immune checkpoint inhibitor–associated endocrinopathies on cancer survival. Front Endocrinol (Lausanne). 2024;15:1369268.38681767 10.3389/fendo.2024.1369268 PMC 11045886 · doi ↗ · pubmed ↗
- 5Wright JJ, Powers AC, Johnson DB. Endocrine toxicities of immune checkpoint inhibitors. Nat Rev Endocrinol. 2021;17(7):389‐399.33875857 10.1038/s 41574-021-00484-3PMC 8769055 · doi ↗ · pubmed ↗
- 6Petrelli F, Grizzi G, Ghidini M, et al Immune-related adverse events and survival in solid tumors treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Journal of Immunotherapy. 2020;43(1):1‐7.31574022 10.1097/CJI.0000000000000300 · doi ↗ · pubmed ↗
- 7Zhao Z, Wang X, Qu J, et al Immune-related adverse events associated with outcomes in patients with NSCLC treated with anti–PD-1 inhibitors: a systematic review and meta-analysis. Front Oncol. 2021;11:708195.34604047 10.3389/fonc.2021.708195 PMC 8479111 · doi ↗ · pubmed ↗
- 8Vardarli I, Tan S, Brandenburg T, et al Risk and incidence of endocrine immune-related adverse effects under checkpoint inhibitor mono- or combination therapy in solid tumors: a meta-analysis of randomized controlled trials. J Clin Endocrinol Metab. 2024;109(4):1132‐1144.37967245 10.1210/clinem/dgad 670 · doi ↗ · pubmed ↗