Aortic Arch Mural Thrombus Concurrent with Deep Surgical-Site Infection after Colorectal Cancer Surgery in an Enhanced Recovery after Surgery Program: A Case Report
Shuto Nakashima, Yoshiaki Fujimoto, Takuya Honboh, Kosuke Hirose, Taichi Nagano, Huanlin Wang, Jun Okadome, Fumihiko Hirai, Noboru Harada, Seiya Kato, Hiroyuki Ito, Noriaki Sadanaga, Tomoharu Yoshizumi

TL;DR
A patient developed a dangerous blood clot in the aorta alongside a deep infection after colorectal cancer surgery, highlighting risks in early post-discharge recovery.
Contribution
This case highlights the rare but serious complication of aortic mural thrombus in the context of ERAS protocols and deep surgical-site infection.
Findings
Aortic mural thrombus developed alongside Streptococcus anginosus-positive deep surgical-site infection without bacteremia or aortitis.
The patient experienced acute carotid occlusion and died from septic shock and coagulation issues.
The case suggests a vulnerable period for complications between postoperative days 7–10 in ERAS pathways.
Abstract
Aortic mural thrombus (AMT) in a non-atherosclerotic aorta is rare but potentially catastrophic and may be difficult to distinguish from septic aortic pathology when it occurs alongside a deep postoperative infection. Enhanced recovery after surgery (ERAS) shortens hospital stay and shifts the recognition of serious complications to the early post-discharge period. We report the case of a patient who underwent colorectal cancer surgery within an ERAS protocol who developed a large AMT on POD 10, coincident with Streptococcus anginosus-positive deep surgical-site infection (SSI) but without bacteremia or aortitis on imaging. A 76-year-old male with stage IVc cecal adenocarcinoma and diabetes underwent robotic-assisted ileocecal resection via the ERAS pathway. Prophylactic cefmetazole was discontinued within 24 h, and the patient was discharged on POD 5 with down-trending but elevated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
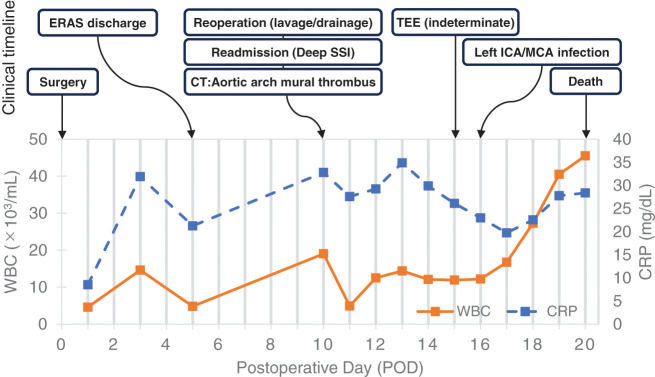 Fig. 1
Fig. 1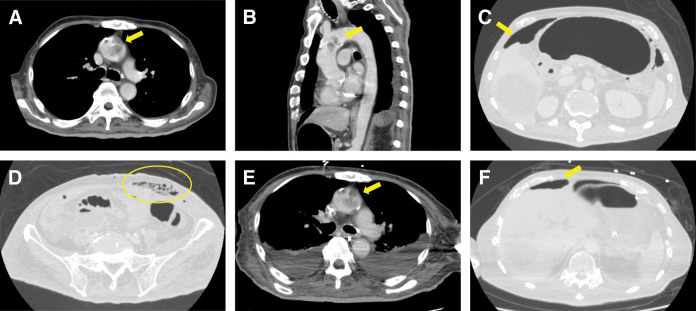 Fig. 2
Fig. 2| Feature | Septic aortic thrombosis | Bland mural thrombus | NBTE | IE | This case |
|---|---|---|---|---|---|
| CT findings (wall thickening/enhancement/periaortic fat stranding) | ○ | ○ | ▲ | × | ▲ |
| Blood culture | ○ | × | × | ○ | × |
| Identification of infection source | ○ | × | × | ○ | × |
| TEE findings | ○ | ▲ | × | ○ | ▲ |
| Inflammatory markers | ○ | ▲ | ▲ | ○ | ▲ |
| Clinical course (response of thrombus) | ▲ | ○ | × | ○ | ○ |
| Pathology/Autopsy (NA) | × | ○ | × | × | ○ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Thrombus and Embolism · Infectious Aortic and Vascular Conditions · Infective Endocarditis Diagnosis and Management
Abbreviations
AMT aortic mural thrombus ERAS enhanced recovery after surgery ICA internal carotid artery IE infective endocarditis LLQ left lower quadrant MCA middle cerebral artery NBTE nonbacterial thrombotic endocarditis NET neutrophil extracellular trap SAG Streptococcus anginosus group SSI surgical-site infection TEE transesophageal echocardiography VTE venous thromboembolism
INTRODUCTION
ERAS reduces postoperative morbidity and length of stay in colorectal surgery, but shifts complication recognition toward an earlier post-discharge window.^1)^ In a large cohort of more than 21000 colorectal cancer resections, nearly one-third of postoperative venous thromboembolic events were diagnosed after discharge, with a median time to diagnosis of 9 days (interquartile range: 4–16 days), indicating that serious thrombotic complications frequently cluster within the first 2 postoperative weeks.^2)^ Therefore, tailoring surveillance and safety net strategies in the early post-discharge period is becoming increasingly important in colorectal oncology.
Among the vascular events that occur during this interval, AMT is uncommon but potentially catastrophic; disturbed flow in the aortic arch promotes thrombus formation and embolization.^3)^ Differentiating bland AMT from infective pathology is critical. Infective aortitis or mycotic aneurysm typically shows CT findings such as mural thickening, enhancement, and periaortic fat stranding, whereas bland AMT may lack these features and often occur without bacteremia.^4)^
SAG is strongly associated with deep abscesses and can markedly amplify local and systemic inflammation in intra-abdominal infections, which may contribute to a prothrombotic milieu in susceptible hosts.^5)^ In parallel, malignancy-related NBTE causes sterile valvular vegetation and embolic phenomena despite negative blood cultures, and remains an important differential diagnosis in cancer patients with arterial events.^6)^
We report the case of a patient with ERAS colorectal cancer surgery who developed a large AMT on POD 10, coincident with SAG-positive deep SSI, but without bacteremia or aortitis on imaging. What this case adds is an ERAS-phase constellation rarely described—POD 10 AMT with SAG-positive deep SSI in the absence of aortitis and bacteremia—that supports a pragmatic diagnostic pathway favoring bland thrombus (while retaining NBTE/IE in the differential diagnosis) and defines ERAS safety-net triggers (CRP-guided discharge, selective low-dose imaging, review on POD 7 ± 1).
CASE PRESENTATION
Patient and comorbidities
The patient, a 76-year-old male, presented with stage IVc cecal adenocarcinoma and type 2 diabetes (HbA1c, 7.6%); he had received no prior systemic anticancer therapy.
Index operation (POD 0) and indication
Semi-elective surgery was performed for malignant large-bowel obstruction and appendicitis secondary to the primary tumor. The patient underwent robotic-assisted ileocecal resection via the ERAS pathway. Intraoperatively, the tumor infiltrated the retroperitoneum with partial rupture/perforation. The terminal ileum was edematous and erythematous with an inflammatory obstruction, and appendiceal abscesses were absent. Prophylactic cefmetazole treatment was discontinued within 24 h.
Early postoperative course (POD 1–5)
The patient remained afebrile (<37°C). Laboratory trends were as follows: WBC 4.6→14.6→4.8 ×10³/μL; CRP 8.52→31.9→21.3 mg/dL (PODs 1→3→5), indicating a peak on POD 3 followed by a downward trend. Clinical improvement was observed, without wound contamination, abdominal pain, or signs of SSI. Pharmacological VTE prophylaxis with enoxaparin 2000 IU (20 mg) was administered subcutaneously twice daily on PODs 2–5. No intra-abdominal drain was placed, in accordance with our institutional policy of not routinely placing drains after right hemicolectomy. He was discharged on POD 5, tolerating a regular diet with restored bowel function and presenting a decreasing CRP level, while remaining clinically stable. The overall clinical trajectory from PODs 0 to 20 is illustrated in Fig. 1.
Clinical timeline from PODs 0–20. The upper panel depicts key clinical events, including ERAS-based discharge on POD 5, readmission on POD 10 with deep surgical-site infection on POD 10, detection of an aortic arch mural thrombus on contrast-enhanced CT, and subsequent development of a left internal carotid artery/middle cerebral artery infarction on POD 16. The lower panel shows serial changes in white blood cell count and C-reactive protein levels over the same period.
Readmission (POD 10)
On POD 10, the patient was readmitted due to fever and decreased mobility. Vital signs were as follows: blood pressure, 126/60 mmHg; heart rate, 135 beats per minute, SpO^2^, 98% on room air; and Japan Coma Scale score of 0. The LLQ port site had a scant purulent exudate. Laboratory findings showed WBC 19 × 10³/μL and CRP 32.8 mg/dL.
Imaging (POD 10)
Contrast-enhanced CT (Fig. 2A–2D) showed a coarse mural filling defect in the aortic arch (~38 mm) without associated aortic wall thickening, abnormal mural enhancement, periaortic fat stranding, aneurysmal dilatation, or complex atherosclerotic plaque. The abdomen demonstrated an LLQ port-site fascial infection with gas, encapsulated collections at the LLQ port site and right paracolic gutter, and diffuse extraluminal gas, consistent with a deep SSI and intra-abdominal abscesses. No definite anastomotic leakage was observed.
Contrast-enhanced CT findings of aortic arch mural thrombus without aortitis and concomitant deep port-site infection. On POD 10, axial and sagittal images of the aortic arch (A, B) show a coarse mural filling defect consistent with a large thrombus (arrows), without associated aortic wall thickening, abnormal mural enhancement, periaortic fat stranding, aneurysmal dilatation, or complex atherosclerotic plaque. Abdominal CT on POD 10 (C, D) demonstrates deep port-site infection, with gas tracking along the fascial plane and encapsulated fluid collections (contour line and arrows). Follow-up CT on POD 16 (E, F) shows a slightly smaller but persistent aortic arch thrombus and decreased intraperitoneal free gas (arrows), in line with partial resolution of the intra-abdominal septic focus.
Reoperation (POD 10)
The patient underwent open abdominal lavage and drainage. Turbid ascites and abscess formation were widely distributed from the right abdomen to the pelvis along the previous surgical field. The ileocolic anastomosis was intact, with no evidence of anastomotic leakage or bowel perforation. An abscess was also identified around the LLQ port site, consistent with a deep SSI, and was considered the primary source with secondary intraperitoneal spread, in accordance with the preoperative CT findings.
Three drains were placed toward the right subphrenic space, pelvic cavity, and left subphrenic space. Because the LLQ port site infection was associated with extensive gas-forming fasciitis, a cruciate incision of the anterior rectus sheath was additionally performed.
Microbiology (pre-antibiotic change, POD 10)
Two sets of blood cultures (arterial and venous) were negative.
Abscess cultures (semiquantitative) yielded: SAG 3+; Klebsiella oxytoca 1+, scant growth of Pseudomonas aeruginosa, and presence of Klebsiella pneumoniae, Bacteroides fragilis, and Parvimonas micra.
Wound cultures showed scant growth of P. aeruginosa, and presence of K. pneumoniae, and Enterococcus casseliflavus.
Management (POD 10 onward)
Broad-spectrum antibiotics were adjusted to 3 g piperacillin-tazobactam every 8 h (PODs 10–16), followed by 1 g ceftriaxone every 12 h and 500 mg metronidazole every 8 h (PODs 17–20). Unfractionated heparin 9600 IU/day was administered on PODs 10–18. The patient required ICU care with mechanical ventilation (PODs 10–20) and continuous hemodiafiltration (PODs 12–19) for oliguric renal failure.
Inflammatory trend
The WBC count (×10³/μL) evolved as follows: 19→12.5→14.4→12.1→11.9→12.2→16.7→27.3→40.5→45.5 (PODs 10–19). CRP (mg/dL) changed as follows: 32.8→29.2→34.9→29.9→26.1→23.0→19.7→22.5→27.8→28.3.
Post-reoperation course
Following reoperation, the intra-abdominal infection showed a favorable response to surgical drainage and antimicrobial therapy, with an initial improvement in inflammatory markers and resolution of systemic inflammatory signs.
No evidence of persistent or new intra-abdominal abscess formation was observed on follow-up imaging.
Blood cultures remained negative, and no other infectious foci, including pneumonia, urinary tract infection, or catheter-related infection, were identified during the subsequent clinical course.
However, despite this initial response, systemic inflammation later worsened during the clinical course, preceding the patient’s deterioration.
Cardiovascular assessment and events
TEE revealed a mural mass in the aortic arch corresponding to the CT lesion but no definite valvular vegetation or leaflet thickening. No typical oscillating masses were observed on the aortic or mitral valves and no new significant valvular regurgitation was observed. Overall, this study did not provide clear evidence of IE or NBTE.
On POD 16, the patient developed an acute left common ICA occlusion with a large left MCA infarction and a midline shift. Follow-up CT on POD 16 (Fig. 2E and 2F) showed that the aortic thrombus was slightly smaller but persistent, with decreasing free gas, ascites, and peritoneal thickening consistent with peritonitis.
Outcome
Despite initial local control of the intra-abdominal infection after reoperation, the patient experienced progressive systemic deterioration, even despite escalation of antimicrobial, anticoagulation, and organ-supportive therapies. He died on POD 20 from septic shock and disseminated intravascular coagulation. An autopsy was not performed, according to the family's wishes.
DISCUSSION
In this ERAS oncology case, the patient developed an AMT in the early post-discharge window, contemporaneous with a SAG-positive deep SSI, and without bacteremia or aortitis on imaging. ERAS reduces morbidity and length of stay; however, when applied to colorectal oncology, it may shift recognition of serious complications to the first 1–2 weeks after discharge, a period in which large registry data show that postoperative thrombotic events frequently cluster around PODs 7–10.^1,2)^ This pattern supports the need for an explicit safety network for high-risk patients. Large database analyses have shown that a meaningful proportion of postoperative VTE events are diagnosed after discharge, and have identified patient- and procedure-related factors associated with post-discharge VTE (e.g., advanced malignancy, obesity, steroid use, open surgery, and prolonged hospitalization).^7)^ Importantly, these findings indicate that thrombotic risk may still be present even in the absence of some traditional risk factors, underscoring the need for individualized risk assessment and risk-stratified post-discharge surveillance. Likewise, postoperative inflammatory markers can help identify patients at higher risk of infectious complications after colorectal surgery; several studies have reported that postoperative CRP measurement (particularly around PODs 3–5) has clinical utility for predicting or ruling out infective complications including anastomotic leak, which can inform discharge planning and post-discharge surveillance.^8)^ In this case, although the CRP level remained elevated at discharge, it had already peaked and showed a clear downward trend, and the patient met the other clinical discharge criteria under the ERAS protocol, including the absence of fever, stable abdominal findings, and recovery of gastrointestinal function. Nevertheless, this case suggests that patients with locally advanced colorectal cancer accompanied by inflammatory features may require more cautious postoperative monitoring, even when laboratory parameters appear to be improving. However, continued inpatient observation was also considered reasonable given the locally advanced disease with inflammatory features, but discharge was ultimately chosen in accordance with the patient’s strong preference after shared decision-making.
The key diagnostic question is whether an identified AMT is septic or bland (Table 1). Infective aortitis or mycotic aneurysms typically show mural thickening, enhancement, and periaortic stranding on CT and are often bacteremic.^4)^ In our patient, the aortic arch had a non-aneurysmal contour without ulcerated or complex atherosclerotic plaque or mural thickening, abnormal enhancement, or periaortic fat stranding, and serial blood cultures remained negative—findings that favor bland AMT in an apparently non-atherosclerotic aorta driven by hypercoagulability rather than overt aortic wall infection.^3,4)^
Cancer and sepsis drive hypercoagulability through tissue factor upregulation, endothelial injury, platelet activation, and NET formation, predisposing patients to arterial thrombosis even without plaque rupture.^9,10)^ Flow separation in the aortic arch increases the embolic risk, which is consistent with subsequent carotid occlusion and MCA infarction.^3,9)^
NBTE remains a relevant differential diagnosis for malignancies with arterial events and negative cultures.^6)^ In this patient, TEE did not reveal discrete valvular vegetations, typical oscillating masses, or new significant valvular regurgitation, making clinically overt IE or NBTE unlikely. However, given the single-timepoint assessment, advanced malignancy, and profound systemic inflammation, small sterile valvular thrombi below the resolution of echocardiography could not be completely excluded.
SAG commonly causes intra-abdominal abscesses and is associated with marked local and systemic inflammatory responses. In this setting, SAG-positive deep SSI is more plausibly viewed as one of several triggers of sepsis-induced coagulopathy rather than a direct cause of thrombosis, potentially contributing to a prothrombotic state in combination with underlying malignancy and postoperative stress.^5,10)^
Management of non-atherosclerotic AMT is individualized: anticoagulation alone yields resolution in many series, while mobile thrombi, recurrent emboli, or anatomy at risk may justify endovascular or surgical intervention.^11–13)^ In our case, rapid neurological deterioration and multiorgan failure precluded the consideration of invasive arch interventions.
Practice implications
For high-risk ERAS colorectal cases, our experience suggests the following measures:
(i)Recognizing approximately PODs 7–10 as a potentially vulnerable period for serious complications and providing explicit return precautions and structured follow-up in this interval, as suggested by prior thromboembolic timing data and the present case.^1,2)^(ii)When CT shows a mural thrombus without aortitis and cultures are negative, prioritizing bland AMT while reassessing for NBTE.^3,4,6)^(iii)Combining rigorous source control and targeted antibiotics for SAG-positive SSI with optimized anticoagulation.^5,11–13)^
Limitations
A lack of autopsy prevented pathological confirmation of the thrombus type and NBTE; nonetheless, imaging, cultures, and clinical course support a bland AMT with NBTE in the differential diagnosis.
CONCLUSIONS
In our patient with ERAS colorectal cancer surgery, a POD 10 AMT occurred alongside a SAG-positive deep SSI without aortitis on CT and with negative blood cultures, supporting a bland-first interpretation driven by malignancy- and sepsis-related hypercoagulability; NBTE/IE was retained in the differential diagnosis. Recognizing approximately PODs 7–10 as a potentially vulnerable window, as suggested by prior data and this case, a focused safety bundle, comprising CRP-guided discharge thresholds, selective low-dose imaging, review on POD 7 ± 1, and individualized anticoagulation with rigorous source control, offers practical steps to reduce similar events in high-risk ERAS cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oodit R, Biccard BM, Panieri E, et al. Guidelines for perioperative care in elective abdominal and pelvic surgery at primary and secondary hospitals in low-middle-income countries (LMIC’s): Enhanced Recovery After Surgery (ERAS) society recommendation. World J Surg 2022; 46: 1826–43.35641574 10.1007/s 00268-022-06587-w PMC 9154207 · doi ↗ · pubmed ↗
- 2Davenport DL, Vargas HD, Kasten MW, et al. Timing and perioperative risk factors for in-hospital and post-discharge venous thromboembolism after colorectal cancer resection. Clin Appl Thromb Hemost 2012; 18: 569–75.22345485 10.1177/1076029611433642 · doi ↗ · pubmed ↗
- 3Yagyu T, Naito M, Kumada M, et al. Aortic mural thrombus in the non-atherosclerotic aorta of patients with multiple hypercoagulable factors. Intern Med 2019; 58: 381–5.30210102 10.2169/internalmedicine.0691-17PMC 6395124 · doi ↗ · pubmed ↗
- 4Jutidamrongphan W, Kritpracha B, Sörelius K, et al. Features of infective native aortic aneurysms on computed tomography. Insights Imaging 2022; 13: 2.35000044 10.1186/s 13244-021-01135-x PMC 8742798 · doi ↗ · pubmed ↗
- 5Pilarczyk-Zurek M, Sitkiewicz I, Koziel J. The clinical view on streptococcus anginosus group - opportunistic pathogens coming out of hiding. Front Microbiol 2022; 13: 956677.35898914 10.3389/fmicb.2022.956677 PMC 9309248 · doi ↗ · pubmed ↗
- 6Zmaili M, Alzubi J, Lo Presti Vega S, et al. Non-bacterial thrombotic endocarditis: a state-of-the-art contemporary review. Prog Cardiovasc Dis 2022; 74: 99–110.36279942 10.1016/j.pcad.2022.10.009 · doi ↗ · pubmed ↗
- 7Thomas DC, Arnold BN, Hoag JR, et al. Timing and risk factors associated with venous thromboembolism after lung cancer resection. Ann Thorac Surg 2018; 105: 1469–75.29501644 10.1016/j.athoracsur.2018.01.072 · doi ↗ · pubmed ↗
- 8Platt JJ, Ramanathan ML, Crosbie RA, et al. C-reactive protein as a predictor of postoperative infective complications after curative resection in patients with colorectal cancer. Ann Surg Oncol 2012; 19: 4168–77.22805866 10.1245/s 10434-012-2498-9 · doi ↗ · pubmed ↗