A complex case of chronic cutaneous Borrelia burgdorferi sensu stricto infection manifesting as morphea-like sclerosis in the United States
Marisa R. Diiorio, Guohong Huang, Payal C. Shah, Shaofeng Yan, Robert E. LeBlanc, Joel A. Lefferts, Lin A. Brown, Dorothea T. Barton

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1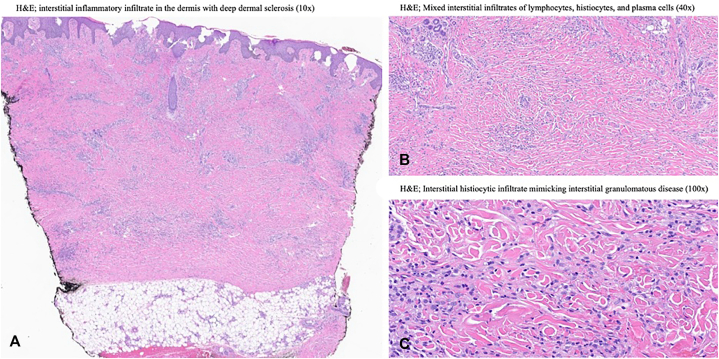 Figure 2
Figure 2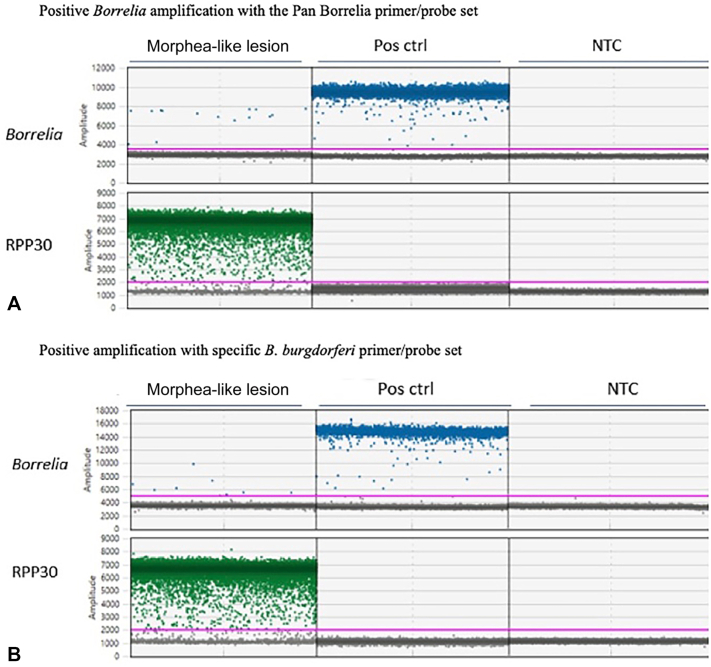 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Vector-borne infectious diseases · Parasitic Diseases Research and Treatment
Introduction
Lyme disease presents with a broad spectrum of cutaneous manifestations, most commonly being erythema migrans, Borrelial lymphocytoma, and acrodermatitis chronica atrophicans (ACA).1 In the United States (U.S.), where Borrelia burgdorferi sensu stricto (B. burgdorferi s.s.) predominates, erythema migrans is the most prevalent and presents as an expanding erythematous patch or plaque in early localized infection.1 In contrast, ACA is a late, chronic manifestation linked to European strains, particularly B. afzelii.2 ACA begins as swollen violaceous plaques on distal extensor surfaces that may progress to thin, atrophic skin, and includes peripheral neuropathy, arthropathy, or nodules over bony prominences in some cases.1^,^2
Beyond these entities, B. burgdorferi has been implicated in fibrosing dermatoses such as morphea and reactive granulomatous dermatitis, which can overlap clinically and histopathologically with ACA.3, 4, 5, 6 ACA reflects an infection-driven process, whereas morphea is an autoimmune sclerosing disorder, often associated with autoantibodies and triggered by trauma, vaccination, or infection.4^,^7 It is typically managed with long-term immunomodulation.4^,^7 Morphea has many subtypes, including generalized, linear, acral, profunda, and the rare nodular variant.7^,^8
Here, we report a diagnostically complex and uncertain case of a chronic fibrosing Borrelia dermatosis, confirmed by droplet digital polymerase chain reaction detection of B. burgdorferi s.s. in lesional tissue, presenting with morphea-like sclerosis and rapid, complete response to doxycycline.
Case summary
A 73-year-old woman presented with a 4-year history of progressive induration, pain, and tingling around the ankles, leading to limited joint mobility and difficulty ambulating. Prior courses of systemic corticosteroids provided minimal benefit. Examination revealed well-demarcated violaceous to red-brown indurated plaques on the dorsal feet and ankles with firm “step-offs” from uninvolved skin (Fig 1, A). Indurated nodules over bony prominences were seen on the mid-spine, bilateral knees, and right elbow (Fig 1, B).Fig 1. Parts A-D, Clinical presentation before and after treatment with doxycycline.
Laboratory studies showed a mildly elevated erythrocyte sedimentation rate and C-reactive protein, positive antinuclear antibody at 1:320, positive anti-B. burgdorferi IgG with negative IgM titers, and a negative extractable nuclear antigen panel. Skin biopsies revealed superficial and deep perivascular and interstitial inflammatory infiltrates with deep dermal sclerosis (Fig 2, A) and decreased dermal CD34 stromal cell staining. The presence of mixed interstitial infiltrates of lymphocytes, histiocytes, and plasma cells were visualized extending into the subcutis (Fig 2, B and C).Fig 2. Parts A-C, Histopathology slides of multiple skin biopsies with hematoxylin and eosin (H&E) staining.
Given the positive anti-Borrelia serologies without a known history of Lyme disease or prior antibiotic treatment, a therapeutic trial of doxycycline (100 mg twice daily for 30 days) was provided. This resulted in rapid, near-complete resolution of the plaques with restoration of joint mobility (Fig 1, C and D). Total DNA extracted from formalin-fixed, paraffin-embedded lesional tissue was analyzed using droplet digital polymerase chain reaction. Positive droplets using B. burgdorferi-specific primer/probe sets were detected (Fig 3, A and B), confirming B. burgdorferi s.s. as the causative species. The droplet digital polymerase chain reaction absolute quantification profile was consistent with only B. burgdorferi, which was further confirmed by Sanger sequencing.Fig 3. Parts A, and B, Positive Borrelia amplification with the Pan Borrelia primer/probe set. NTC, nontemplate control.
The RPP30 gene served as an internal control, and it was targeted with a commercial primer/probe mix from Bio-Rad (Cat # 10031243). (A) Pan Borrelia primer/probe set,6 targeting the 5S-23S intergenic spacer region: 5′-TTCTTCGCCTTAAAGCTCCT-3′ (Forward), 5′-TGGCAAAATAGAGATGGAAGAT-3′ (Reverse), 5′-FAM-ATTACTTTGACCATATTT-MGBNFQ-3′ (Probe) (B) B. burgdorferi-specific primer/probe set, targeting the ospA gene: 5′-TTGAAGGCGTAAAAGCTGAC-3′ (Forward), 5′-ACTAGTGTTTTGCCATCTTC-3′ (Reverse), 5′-FAM-TCTGACGATCTAGGTCAAACCACACT-BHQ1-3′ (Probe). Pos ctrl: positive control. NTC: nontemplate control.
Discussion
We present a rare and diagnostically uncertain case of chronic fibrosing Borrelia-associated dermatosis. ACA and morphea were both strongly considered given overlapping clinical, histopathologic, and molecular features; however, inconsistencies with each entity prevented a unifying diagnosis.
Several aspects of our patient’s presentation overlap with features reported in the largest and most comprehensive study of ACA to date,2 including bilateral acral violaceous plaques of the lower-extremities and nodules on extensor elbows, both with lesional molecular confirmation of B.burgdorferi s.s.,2^,^3^,^6 as well as neuropathic symptoms confined to affected joints.2 However, important inconsistencies exist. Notably, the lesions were sharply well-demarcated, favoring morphea,7 rather than the ill-defined, progressive plaques typical of ACA.2 Additionally, B. burgdorferi s.s. is documented to be a rare cause of ACA, and there was no clinical or histopathologic evidence of cutaneous atrophy. In the medical literature, most but not all patients (59%) exhibit at least 1 atrophic feature at presentation, with a median progression time of 12 months from inflammatory to atrophic stages, and longer symptom duration correlating with an increased likelihood of atrophy.2 In this context, a 4-year disease course without atrophic progression adds further uncertainty to ACA as a unifying diagnosis. Given B. burgdorferi’s association with more atypical ACA features such as arthropathy, it remains plausible that B. burgdorferi infection may incite a more inflammatory phenotype or slower progression to atrophic stages compared with B. afzelii, but this requires further formal investigation.2
B. burgdorferi-associated morphea was also carefully considered for diagnosis.4 The deeply indurated, thickened, well-demarcated plaques without atrophy, along with joint restriction, ANA positivity, and certain histological features (Fig 2, A), could support an autoimmune sclerosing process consistent with morphea.5^,^7^,^8 As often seen with morphea, corticosteroids were ineffective in this patient. Atypically, however, doxycycline achieved rapid and near-complete resolution. While some European reports describe antibiotic-responsive Borrelia-associated morphea, it remains unclear whether these represent primary morphea or Borrelia infection triggering a reactive sclerosing dermatosis.3^,^5 Dermatology literature more generally indicates that effective management of primary morphea requires long-term immunosuppression and often has minimal response to antibiotics.3^,^7 The presence of acral nodules is also atypical,7 and the concurrence of 2 rare morphologic variants (acral and nodular) in a single patient, together with near-complete antibiotic response, contributes to the uncertainty of primary morphea as a unifying diagnosis.7^,^9 However, Borrelia infection triggering reactive morphea may still be possible.
Histopathologic findings further support an infection-driven process. Sclerosing features seen in morphea are present in this patient (Fig 2, A); however, the RGD-like patterns and subcutaneous involvement also seen here (Fig 2, B and C), are well-documented in Borrelia-associated dermatoses, but are not characteristic of morphea.6 Loss of CD34 staining, often cited in morphea, is a nonspecific feature and also occurs in chronic Borrelia-related sclerosis, including ACA.6 Collectively, these histopathologic findings evidence B.burgdorferi infection inducing sclerotic, atrophic, and granulomatous microscopic changes, and underscores the diagnostic complexity of this case.3^,^6
This case offers a rare, molecularly confirmed example of a chronic cutaneous fibrosing Lyme borreliosis in the U.S., demonstrating both pathogen detection and rapid antibiotic response. This reinforces the importance of early serologic and molecular Borrelia testing in sclerosing dermatoses, particularly in endemic regions, before initiating immunosuppressive therapy, which may be avoided. Future investigation to better characterize Borrelia burgdorferi-associated fibrosing dermatoses and responsiveness to antibiotic therapy is worthwhile.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vasudevan B.Chatterjee M.Lyme borreliosis and skin Indian J Dermatol 583201316717410.4103/0019-5154.11082223723463 PMC 3667275 · doi ↗ · pubmed ↗
- 2Ogrinc K.Maraspin V.Lusa L.Cerar Kisek T.Ruzic-Sabljic E.Strle F.Acrodermatitis chronica atrophicans: clinical and microbiological characteristics of a cohort of 693 Slovenian patients J Intern Med 2902202133534810.1111/joim.1326633550695 PMC 9292144 · doi ↗ · pubmed ↗
- 3Aberer E.Wutte N.Atrophosclerodermic manifestations of lyme borreliosis Open Dermatol J 10M 420162743
- 4George E.Nielson C.B.Vincek V.Tick bite-associated morphea: a case report Am J Dermatopathol 4110201974774910.1097/DAD.000000000000129030325752 · doi ↗ · pubmed ↗
- 5Buechner S.A.Rufli T.Atrophoderma of pasini and pierini. Clinical and histopathologic findings and antibodies to Borrelia burgdorferi in thirty-four patients J Am Acad Dermatol 303199444144610.1016/s 0190-9622(94)70053-28113457 · doi ↗ · pubmed ↗
- 6Podbicanin-Ziburt A.Falk T.M.Metze D.Boer-Auer A.Diagnosis of lyme borreliosis with a novel, seminested real-time polymerase chain reaction targeting the 5S-23S intergenic spacer region: clinical features, histopathology, and immunophenotype in 44 patients Am J Dermatopathol 445202233834710.1097/DAD.000000000000211934966044 · doi ↗ · pubmed ↗
- 7Papara C.De Luca D.A.Bieber K.Vorobyev A.Ludwig R.J.Morphea: the 2023 update Front Med (Lausanne)102023110862310.3389/fmed.2023.1108623 PMC 996999136860340 · doi ↗ · pubmed ↗
- 8Fett N.Werth V.P.Update on morphea: part I. Epidemiology, clinical presentation, and pathogenesis J Am Acad Dermatol 6422011217228 quiz 229-22810.1016/j.jaad.2010.05.04521238823 · doi ↗ · pubmed ↗