Thrombectomy versus Medical Management for Pediatric Acute Ischemic Stroke Due to Isolated M2 Occlusion: A Multicenter Cohort Study
Peter B. Sporns, Kartik D. Bhatia, Prakash Muthusami, Carmen Parra‐Farinas, Christine K. Fox, Adam A. Dmytriw, Basile Kerleroux, Sarah Lee, Jens Fiehler, Christian Lehmann, Franja Dugar, Todd Abruzzo, Lisa Pabst, Stuart Fraser, Lisa R. Sun, Grégoire Boulouis, Tanja Burkard

TL;DR
This study finds that endovascular thrombectomy improves outcomes for children with a specific type of stroke compared to medical therapy alone.
Contribution
The study is the first to evaluate endovascular thrombectomy for isolated M2 occlusions in pediatric stroke patients.
Findings
EVT resulted in better functional outcomes (ped-mRS) at 3-6 months compared to medical therapy.
EVT showed greater neurological improvement (PedNIHSS reduction) within the first week.
EVT had a favorable safety profile with no access-site complications or deaths.
Abstract
Endovascular thrombectomy (EVT) is increasingly used for pediatric large vessel occlusion (LVO) stroke, however, its role in isolated M2 occlusions remains underexplored. This study compared clinical outcomes in children with isolated M2 occlusion treated with EVT versus best medical therapy (BMT). This multicenter cohort study pooled data from 4 pediatric stroke registries (Save ChildS, KidClot, Pediatric LVO Study, and Save ChildS Pro). Children ages 28 days–17 years with isolated M2 occlusion presenting within 24 hours of last seen well were included. Primary outcome was the pediatric modified Rankin scale (ped‐mRS) at 3 to 6 months. Secondary outcomes included changes in Pediatric National Institutes of Health Stroke Scale (PedNIHSS), Pediatric Stroke Outcome Measure (PSOM), and safety endpoints. Forty patients were included, of whom 20 were treated with EVT (median age, 12 years;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
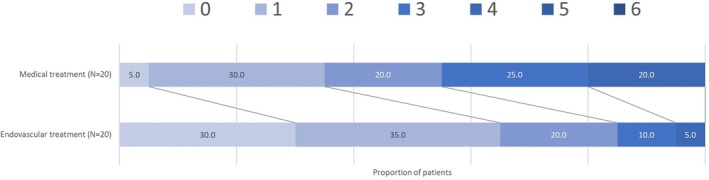 FIGURE 1
FIGURE 1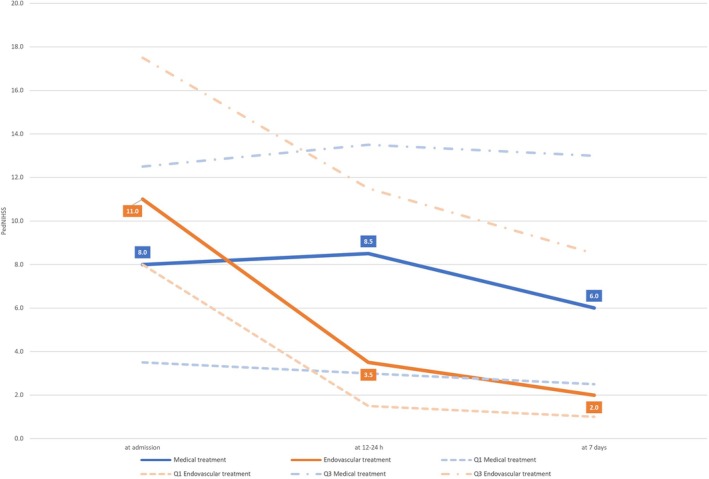 FIGURE 2
FIGURE 2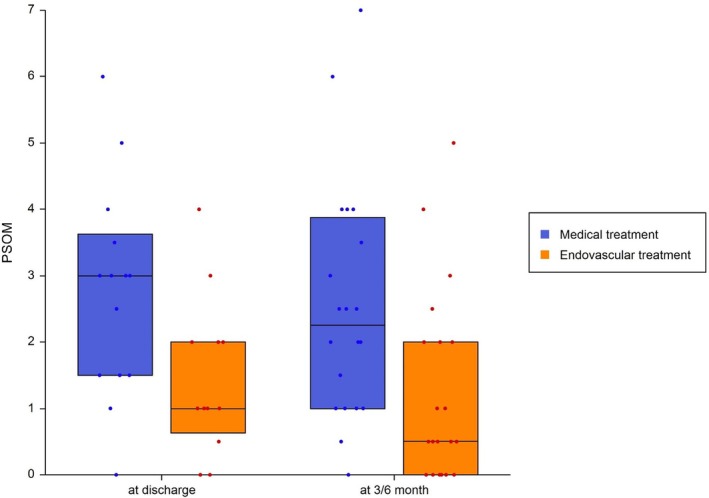 FIGURE 3
FIGURE 3| Endovascular thrombectomy (N = 20) | Best medical treatment (N = 20) |
| |
|---|---|---|---|
| Median age (IQR), yr | 12 (6–15) | 10 (5–14) | 0.278 |
| Sex | 0.525 | ||
| F | 8 (40%) | 10 (50%) | |
| M | 12 (60%) | 10 (50%) | |
| Median PedNIHSS score at hospital arrival (IQR) | 11 (8–18) | 8 (4–13) | 0.069 |
| Median onset to admission (IQR), hours | 1.4 (0.7–2.0) | 3.2 (1.9–7.0) | 0.005 |
| Median onset to recanalization (IQR), hours | 7.0 (3.9–8.0) | – | – |
| Median ASPECTS baseline (IQR) | 9 (8–10) | 7 (6–9) | 0.045 |
| Median interval between symptom onset and admission for known onset strokes (IQR), hours | 2.2 (0.9–4.6) | 3.8 (1.3–7.1) | 0.046 |
| Median interval between symptom onset and first recanalization pass (IQR), hours | 5.7 (4.0–8.4) | – | – |
| Anesthesia performed (%) | |||
| Conscious sedation or none | 15 (13) | – | – |
| General anesthesia | 102 (87) | – | – |
| Type of device used for thrombectomy, n (%) | |||
| Aspiration catheter alone | 31 (26) | – | – |
| Stent retriever alone | 72 (62) | – | – |
| Both aspiration catheter and stent retriever | 14 (12) | – | – |
| Median attempts for thrombectomy (IQR), n | 2 (1–3) | – | – |
| Intravenous tPA, n (%) | 6 (30) | 2 (10) | 0.235 |
| Etiology according to CASCADE classification | 0.163 | ||
|
Small vessel arteriopathy | 0 (0) | 0 (0) | |
|
Focal cerebral arteriopathy | 4 (20) | 7 (35) | |
|
Bilateral cerebral arteriopathy | 0 (0) | 0 (0) | |
|
Aortic/cervical arteriopathy | 0 (0) | 2 (10) | |
|
Cardioembolic | 10 (50) | 4 (20) | |
|
Other | 6 (30) | 6 (30) | |
|
Multi‐factorial | 0 (0) | 1 (5) |
| Endovascular thrombectomy (N = 20) | Best medical treatment (N = 20) |
| |
|---|---|---|---|
| Median score on modified Rankin scale at 3–6 mo (IQR) | 1 (0–2) | 2 (1–3) | 0.015 |
| Median score on Pediatric Stroke Outcome Measure at 3–6 mo (IQR) | 0.5 (0–2) | 2.5 (1–4) | 0.009 |
| Median difference of Pediatric NIHSS at 7 days vs admission (IQR) | −9 (−10 to −6) | −1 (−3 to 0) | <0.001 |
| Median score on Pediatric Stroke Outcome Measure at discharge (IQR) | 1 (1–2) | 3 (1.5–3.5) | 0.033 |
| Median score on modified Rankin scale at 24 mo (IQR) | 1 (0–2) | 2 (1–3) | 0.012 |
| Successful recanalisation (mTICI 2b or better) | 19 (95%) | – | – |
| Complete recanalisation (mTICI 3) | 6 (30%) | – | – |
| Median ASPECTS follow‐up (IQR) | 8 (7–9) | 6 (4–8) | 0.063 |
| Endovascular thrombectomy (N = 20) | Medical treatment (N = 20) |
| |
|---|---|---|---|
| Death (modified Rankin scale 6) at 3–6 mo | 0 (0%) | 0 (0%) | – |
| Symptomatic intracranial hemorrhage | 0 (0%) | 1 (5%) | – |
| Transient intra‐procedural vasospasm | 3 (15%) | – | – |
| Endovascular thrombectomy (N = 14) | Medical treatment (N = 14) |
| |
|---|---|---|---|
| Median score on modified Rankin scale at 3–6 mo (IQR) | 1 (0–2) | 3 (1–4) | 0.029 |
| Median score on Pediatric Stroke Outcome Measure at 3–6 mo (IQR) | 0.5 (0–2) | 2.5 (1.5–4) | 0.013 |
| Median difference of Pediatric NIHSS at 7 days vs admission (IQR) | −8 (−10 to −4) | 0 (−3–0) | 0.014 |
| Median score on modified Rankin scale at 24 mo (IQR) | 1 (0–2) | 3 (1–3) | 0.032 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Coagulation and Thrombosis Mechanisms · Acute Ischemic Stroke Management · Neurological Disorders and Treatments
Arterial ischemic stroke (AIS) affects 1.3 to 1.6 per 100,000 children annually in developed countries, with significant long‐term morbidity and mortality.1, 2, 3 Unlike adults, pediatric stroke is rarely caused by atherosclerosis, and systematic research is limited by recruitment challenges, as seen in the early termination of the TIPS trial.4
In recent years, endovascular thrombectomy (EVT) has become standard of care for adult large vessel occlusion (LVO) stroke.5, 6 Although retrospective studies like Save ChildS7 and Kid Clot8 supported EVT's safety and effectiveness in children, they were limited by the lack of control groups. The prospective multicenter Save ChildS Pro registry recently provided evidence for the safety of EVT for pediatric LVO stroke and showed an association with better neurological outcomes in children with LVO stroke who received EVT compared to those with best medical treatment (BMT) alone.9
Although adult trials show that EVT can benefit patients with isolated occlusions of the M2‐segment of the middle cerebral artery (MCA)10—albeit with smaller effect sizes than for LVOs—pediatric data are sparse. The largest series reported 6 children and focused on technical aspects and factors relevant to decision making, but systematic conclusions could not be drawn.11
To address this evidence gap, we undertook a pooled analysis comparing outcomes between EVT and BMT in pediatric patients with isolated M2 occlusions, using harmonized data from the 4 largest available multicenter cohort studies. We hypothesized that EVT would be associated with better functional outcomes and greater neurological improvement.
Methods
Study Design and Participants
We conducted a secondary analysis of de‐identified data pooled from 4 previously published multicenter pediatric stroke studies: (Save ChildS,7 Kid Clot,8 the Pediatric LVO Stroke Study,12 and Save ChildS Pro9, 13) (Table S1). Inclusion criteria were age 28 days to 17 years at stroke onset, acute ischemic stroke because of isolated M2 occlusion (imaging assessment partly performed by local interdisciplinary stroke team), and clinical presentation within 24 hours since last seen well (LSW). Patients with tandem occlusions or proximal ICA/M1 involvement were excluded.
All patients with M2 occlusions were stratified into 2 groups: those who underwent EVT (n = 20) and those who received BMT alone (n = 20).
Save ChildS Pro was approved by the ethics committee of the University of Münster (Münster, Germany; 2019‐677‐f‐S), in accordance with the Declaration of Helsinki, with waiver for informed consent. Institutional review board approvals and data‐sharing agreements were in place for each contributing registry.
Outcomes
The primary outcome was the pediatric modified Rankin scale (ped‐mRS) score at 3 to 6 months after stroke onset.
Secondary outcomes included difference in Pediatric National Institutes of Health Stroke Scale (PedNIHSS) at 7 days vs admission, Pediatric Stroke Outcome Measure (PSOM) at discharge, PSOM at 3 to 6 months, ped‐mRS at 24 months (interquartile range [IQR]), rate of successful recanalisation (mTICI 2b or better) in the EVT group, rate of symptomatic intracranial hemorrhage (sICH), access site complications, and the rate of intra‐procedural vasospasm in the EVT group.
Statistical Analysis
Continuous variables were compared using the t test or Mann–Whitney U‐test as appropriate. Categorical variables were compared using chi‐squared or Fisher's exact tests. Ordinal data (eg, ped‐mRS, PSOM) were analyzed using ordinal logistic regression or non‐parametric methods. Propensity score matching was performed adjusted for the variables sex, age, PedNIHSS at admission, and Alberta Stroke Program Early Computed Tomography Score (ASPECTS) at admission. Fourteen patients from each treatment group were matched 1:1 with an absolute difference between propensity scores of 0.2 1 adjusting for age, sex, admission PedNIHSS, and ASPECTS. The statistical analysis was carried out using SAS version 9.4 (SAS Institute, Cary, NC). A p‐value <0.05 was considered statistically significant.
Results
A total of 40 pediatric patients with isolated M2 occlusion were included in the study, with 20 receiving EVT and 20 treated with best medical therapy BMT. Baseline demographics and clinical characteristics were similar between groups, including age, sex, and stroke severity at presentation. Median age was 12 years in the EVT group and 10 years in the BMT group. The EVT group had a shorter median time from symptom onset to hospital admission (86 minutes vs 192 minutes, p = 0.022) and had higher baseline ASPECTS scores (9 vs 7, p = 0.036) (Table 1).
At 3 to 6 months, children treated with EVT had better functional outcomes. The median ped‐mRS score was 1 (IQR, 0–2) in the EVT group compared to 2 (IQR, 1–3) in the BMT group (p = 0.015). This benefit persisted at 24 months: at that time point the median ped‐mRS was 1 (IQR, 0–2) in the EVT group and 2 (IQR, 1–3) in the BMT group (p = 0.012) (Table 2, Fig 1).
Distribution of modified Rankin scale scores at 3–6 months following stroke onset. [Color figure can be viewed at www.annalsofneurology.org]
Neurological improvement within the first week after stroke was also greater in the EVT group. The median reduction in PedNIHSS from admission to day 7 was −9 (IQR, −10 to −6) for EVT compared with −1 (IQR, −3 to 0) for BMT (p < 0.001) (Fig 2). At discharge, the PSOM was lower in EVT patients (median, 1; IQR, 1–2) compared to BMT (median, 3; IQR, 1.5–3.5; p = 0.033). At 3 to 6 months, median PSOM scores remained better in the EVT group (0.5; IQR, 0–2) versus BMT (2.5; IQR, 1–4; p = 0.009) (Fig 3).
Course of Pediatric National Institutes of Health Stroke Scale from admission to day 7. [Color figure can be viewed at www.annalsofneurology.org]
PSOM at discharge and 3–6 months post‐stroke. Values in boxplots show median and interquartile range in both the EVT and BMT group at discharge and at follow‐up. Dots are single patients in total range. BMT = best medical therapy; EVT = endovascular thrombectomy; PSOM = Pediatric Stroke Outcome Measure. [Color figure can be viewed at www.annalsofneurology.org]
Successful recanalization (defined as mTICI 2b or better) was achieved in 95% of EVT patients. Complete recanalization (mTICI 3) was achieved in 30%. Safety outcomes were similar across groups. One symptomatic intracranial hemorrhage occurred in the BMT group (5%) and none in the EVT group. There were no deaths or access‐site complications reported. Transient intra‐procedural vasospasm occurred in 3 patients (15%) undergoing EVT (Table 3).
A propensity score–matched analysis of 14 EVT and 14 BMT patients confirmed these findings. In this matched cohort, EVT remained associated with significantly better functional outcomes at 3 to 6 months (median ped‐mRS, 1 vs 3; p = 0.029), better PSOM scores at 3 to 6 months (median, 0.5 vs 2.5; p = 0.013), greater early neurological improvement (median PedNIHSS reduction, −8 vs 0; p = 0.014), and better long‐term outcomes at 24 months (median ped‐mRS, 1 vs 3; p = 0.032) (Table 4).
Discussion
In this multicenter cohort study of children with isolated M2 occlusion, EVT was associated with better functional outcomes compared to BMT alone, despite a trend towards higher PedNIHSS at presentation in the EVT group. The group of children with EVT had higher rates of favorable outcomes (ped‐mRS, PSOM), greater early neurologic improvement, and no increase in symptomatic intracranial hemorrhage or procedural complications. These findings support the expanding role of EVT in carefully selected children with stroke and an isolated M2 occlusion.
Although results from of a meta‐analysis from the HERMES collaboration have suggested benefit of EVT in proximal M2 occlusions with modest effect sizes,10 recent randomized controlled trials including distal intracranial occlusions14, 15 did not show better functional outcomes after EVT compared to BMT alone. Nonetheless our results suggest that for M2 occlusions there is a robust treatment effect of EVT in children, potentially because of greater neuroplasticity, better collateral circulation,16, 17 and fewer comorbidities.1 Notably, successful recanalization (mTICI 2b–3) was achieved in 95% of EVT cases, which may also be attributed to the lower prevalence of intracranial atherosclerosis and the lower rate of difficult vascular access because of vessel tortuosity in children.18 Additionally, focal cerebral arteriopathy, a frequent etiology of stroke in children and a factor possibly complicating EVT, is usually confined to the intracranial carotid artery and the M1‐segment.19, 20 Importantly, the EVT group showed a meaningful reduction in NIHSS at 24 hours, indicating early neurologic benefit.
Although baseline demographics were generally well balanced between treatment groups, some clinically relevant differences were observed. The EVT group had a higher median PedNIHSS score at presentation (11 vs 8), suggesting more severe initial neurological deficits, although this difference did not reach statistical significance (p = 0.081). Additionally, patients in the EVT group presented earlier, with significantly shorter onset‐to‐admission times (86 vs 192 minutes, p = 0.022), and had higher baseline ASPECTS scores (9 vs 7, p = 0.036), indicating smaller initial infarcts.
To mitigate these baseline imbalances and reduce potential confounding, we performed a propensity score matched comparison, which confirmed the superiority of EVT across all primary and secondary outcome measures, supporting the robustness of our findings and suggesting that the observed treatment effect is unlikely to be fully explained by baseline differences alone.
Regarding safety, there was no difference in the rate of symptomatic intracranial hemorrhage between groups, suggesting EVT in M2 occlusion carries an acceptable safety profile.
Overall, our findings suggest that children with acute M2 occlusion should not be automatically excluded from consideration for EVT. In a setting where conducting randomized trials is unlikely feasible because of recruitment challenges for M2 occlusions and the difficulty of randomizing children for a treatment that has shown a strong effect in adults for LVOs, this study provides practical evidence supporting individualized decisions in pediatric stroke management, particularly when access to pediatric stroke expertise and endovascular teams are available. It also emphasizes the importance for international collaborations for the study of rare diseases, which may be used to inform future guidelines.
This study is limited by its retrospective, non‐randomized design and relatively small sample size. Matching attempted to reduce bias, but unmeasured confounders may still influence outcomes. Imaging protocols were heterogeneous and occlusion location and ASPECTS were not centrally adjudicated. Included cohorts were heterogeneous, which may also be a strength by expanding geographic representation and increasing generalizability. Especially, the patients in the EVT group presented earlier and had higher baseline ASPECT scores compared to the BMT group. Last, this presents by far the largest available pediatric M2 occlusion dataset, pooling data from 4 major registries.
Conclusion
This pooled analysis suggests that EVT for pediatric stroke because of isolated M2 occlusion may lead to improved functional outcomes compared with medical therapy alone. Therefore, EVT should be considered in carefully selected pediatric patients with M2 occlusion. Further prospective data and international consensus are needed to guide standardized practice.
AUTHOR CONTRIBUTIONS
P.B.S., and M.W. contributed to the conception and design of the study; P.B.S., K.D.B., P.M., C.P.F., C.K.F., A.A.D., B.K., S.L., J.F., C.L., F.D., T.A., L.P., S.F., L.R.S., G.B., T.B., O.N., M.K., A.K., M.O., M.M., M.P., T.D.L.N.K., and M.W. contributed to the acquisition and analysis of data; P.B.S., T.B., and M.W. contributed to drafting the text or preparing the figures. [Correction added on 25 February 2026, after first online publication: Author contribution text has been revised in this version.]
Potential Conflicts of Interest
Nothing to report.
Supporting information
Table S1. Major studies on hyperacute recanalization in children.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sporns PB , Fullerton HJ , Lee S , et al. Childhood stroke. Nat Rev Dis Prim 2022;8:12.35210461 10.1038/s 41572-022-00337-x · doi ↗ · pubmed ↗
- 2Sun H , Ma B , Jin C , et al. Global, regional, and National Burdens of stroke in children and adolescents from 1990 to 2019: a population‐based study. Stroke 2024;55:1543–1553.38591228 10.1161/STROKEAHA.123.044827 · doi ↗ · pubmed ↗
- 3Sporns PB , Fullerton HJ , Lee S , et al. Current treatment for childhood arterial ischaemic stroke. Lancet Child Adolesc Health 2021;5:825–836. 10.1016/s 2352-4642(21)00167-x.34331864 · doi ↗ · pubmed ↗
- 4Rivkin MJ , de Veber G , Ichord RN , et al. Thrombolysis in pediatric stroke study. Stroke 2015;46:880–885.25613306 10.1161/STROKEAHA.114.008210 PMC 4342311 · doi ↗ · pubmed ↗
- 5Goyal M , Menon BK , van Zwam WH , et al. Endovascular thrombectomy after large‐vessel ischaemic stroke: a meta‐analysis of individual patient data from five randomised trials. Lancet 2016;387:1723–1731.26898852 10.1016/S 0140-6736(16)00163-X · doi ↗ · pubmed ↗
- 6Sporns PB , Fiehler J , Ospel J , et al. Expanding indications for endovascular thrombectomy‐how to leave no patient behind. Ther Adv Neurol Disord 2021;14:1756286421998905. 10.1177/1756286421998905.33796144 PMC 7970189 · doi ↗ · pubmed ↗
- 7Sporns PB , Sträter R , Minnerup J , et al. Feasibility, safety, and outcome of endovascular recanalization in childhood stroke: the save Child S study. JAMA Neurol 2020;77:25–34. 10.1001/jamaneurol.2019.3403.31609380 PMC 6802048 · doi ↗ · pubmed ↗
- 8Kossorotoff M , Kerleroux B , Boulouis G , et al. Recanalization treatments for pediatric acute ischemic stroke in France. JAMA Netw Open 2022;5:e 2231343. 10.1001/JAMANETWORKOPEN.2022.31343.36107427 PMC 9478769 · doi ↗ · pubmed ↗