My Heart and CKD: Pathway to Implementing a Decision Aid for Patients With CKD and Coronary Artery Disease
Julie N. Babione, Pantea Javaheri, Denise Kruger, Todd Wilson, Winnie Pearson, Maureena Loth, Violet March, Wayne Gerber, Bryan J. Har, Michelle M. Graham, Stephen B. Wilton, Krystina B. Lewis, Matthew T. James

TL;DR
My Heart and CKD is a decision aid designed to help patients with chronic kidney disease and coronary artery disease make informed choices about their treatment options through shared decision-making with their care providers.
Contribution
The paper presents a novel pathway for implementing a decision aid specifically tailored for CKD patients with CAD, emphasizing human-centered design and shared decision-making.
Findings
Human-centered design was used to develop the decision aid, incorporating features that support bidirectional communication and relationship building.
Implementation insights influenced key design elements and strategies to facilitate clinical use in varying contexts.
Training and resources, including a continuous medical education program, were identified as essential for effective implementation.
Abstract
Patients with chronic kidney disease (CKD) at times must decide whether to take an invasive approach to management of coronary artery disease (CAD), which involves procedures such as angiography, angioplasty, and surgery, versus attempt management with medications alone. My Heart and CKD is a decision aid to support shared decision-making (SDM) between patients and their care providers in these situations. This report describes the pathway to implement My Heart and CKD , and key learnings that have emerged through this process. Human-centered design was used to develop the decision aid while concurrently identifying design features that could facilitate its incorporation within patient-physician clinical encounters. Interviews exploring use of the decision aid with patients and care providers were qualitatively analyzed according to the theoretical domains framework to identify…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
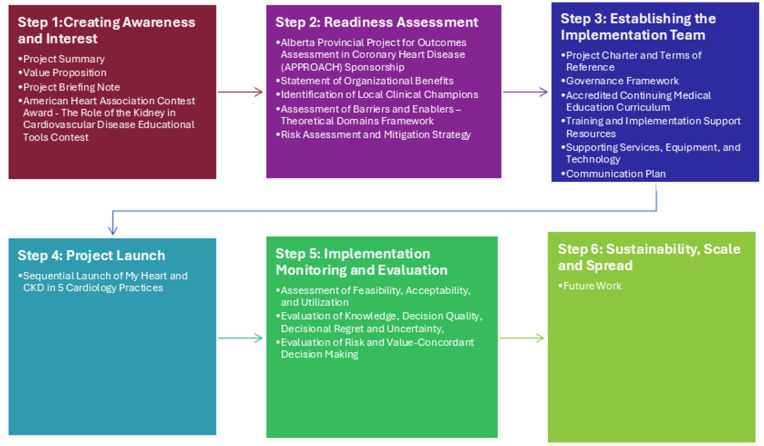 Figure 1
Figure 1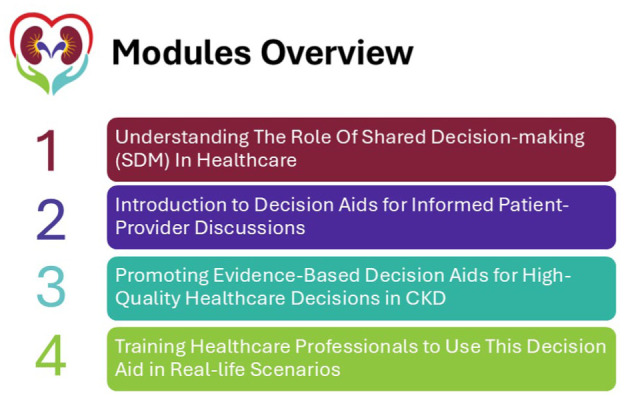 Figure 2
Figure 2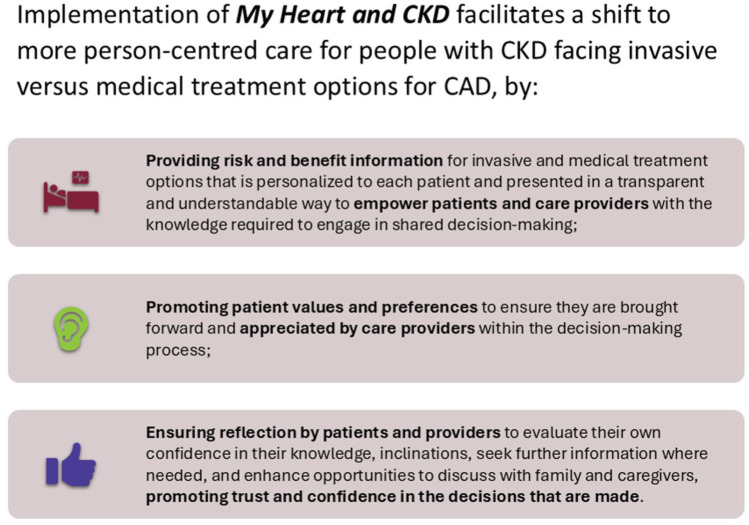 Figure 3
Figure 3- —University of Calgaryhttps://doi.org/10.13039/100008459
- —Libin Cardiovascular Institute, University of Calgaryhttps://doi.org/10.13039/100031571
- —Nephrology Research Group
- —Canadians Seeking Solutions and Innovations to Overcome
- —Strategy for Patient-Oriented Researchhttps://doi.org/10.13039/100021570
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMental Health and Patient Involvement · Health Policy Implementation Science · Patient-Provider Communication in Healthcare
Background
Coronary artery disease (CAD) commonly accompanies chronic kidney disease (CKD), and can result in hospitalizations, reduced quality of life, shortened survival, and has implications for receiving a kidney transplant.^ 1 ^ Patients with CKD and CAD often must decide whether to take an invasive approach to management, which involves procedures such as angiography, and revascularization procedures to diagnose and treat heart disease, versus attempting optimal medication management alone. This can be a challenging decision for patients and care providers to make, due to the complex trade-offs in the benefits of these procedures for treating heart disease versus their unique risks to the kidney health of people with CKD.^ 2 ^
In earlier phases of work, our team engaged with patients with CKD and CAD, and their care providers to develop patient-oriented solutions to address this issue. As a project funded by the patient-oriented research network, Canadians Seeking Solutions for Chronic Kidney Disease (Can-SOLVE CKD), patient partners with lived experience guided all aspects of our research. We first conducted qualitative studies with patients and health care providers to characterize their experiences with CKD and CAD and identify potential strategies to overcome identified challenges in care.^ 2 ^ We then developed and validated predictive models to provide patients and their care providers with personalized benefit-risk information under different treatment options for CAD. We also conducted a discrete choice experiment to better understand the values patients placed on the attributes of different treatment options, and how patient preferences varied.^ 3 ^ Finally, we used human-centered design (HCD),^4 ???-8^ informed by International Patient Decision Aid Society^9,10^ and the Ottawa Decision Support Framework,^ 11 ^ to synthesize current knowledge within a decision aid that we have named ** My Heart and CKD **. This web-based decision aid, available at www.myheartandckd.ca, is intended to support shared decision-making (SDM)^12 ?-14^ between patients with CKD and CAD and their care providers, within a context of trust-building that empowers patients in decision-making by providing personalized information and promoting respect for patients’ values and preferences.
This initiative has now progressed to implementation and evaluation of a SDM approach to invasive versus medical CAD management decisions, supported by the ** My Heart and CKD ** decision aid. Knowledge mobilization and implementation have been prominent throughout our work. Important insights from patients and care providers originated during the design and development of the decision aid and have carried through to current pilot testing the impact of the tool on patient and care provider experiences. In this paper, we describe the pathway taken to implement ** My Heart and CKD ** into clinical care in Canada, and key learnings that have emerged through our work to date.
Methods
This project’s activities revolve around Can-SOLVE CKD’s 4 pillars of: (1) implementation science/knowledge mobilization, (2) Indigenous cultural competency, (3) incorporation of equity, diversity, and inclusion (EDI) principles in knowledge mobilization and implementation efforts, and (4) patient engagement and capacity building. The ways each of these 4 pillars have been applied are described here.
Pillar 1: Implementation Science/Knowledge Mobilization
To ensure capacity within the project team to support implementation, 3 team members completed courses on “The How of Creating Sustainable Change” and “Implementation Scale and Spread” offered by the Centre for Implementation (https://thecenterforimplementation.com/). This allowed us to capture early insights into barriers and facilitators to implementing ** My Heart and CKD **, brought forward by patients and care providers starting from its development. During the design and development phase, we created and refined successive iterations of the decision aid over 3 phases that included interviews with patients and care providers, with review of each iteration. As this process progressed and the decision aid took shape, the focus of discussions increasingly shifted from the design of the tool itself to how the decision aid would be implemented into clinical practice and within workflows in outpatient clinics and hospital settings. Noting these emerging areas of discussion during the development process, we purposefully analyzed the data from these interviews to identify themes related to implementation. Transcripts from all phases were analyzed using content analysis, with implementation-related content deductively categorized using the theoretical domains framework (TDF).^15,16^ Suggestions to facilitate implementation approaches were integrated into the decision aid as it evolved and these findings were also used to identify additional implementation supports that would be needed by patients and physicians to effectively use the decision aid, including a collection of continuous medical education (CME)-accredited training materials and implementation guidance resources for users.
To further augment our implementation strategy, we conducted simulated patient-physician encounters for pre-clinical testing of the decision aid. We created 4 unique patient personas and used them with 2 patients and 2 physicians to simulate and observe encounters using the decision aid in hypothetical outpatient clinic and hospital settings. The sessions were observed by the research team, and the patients and physicians who participated in the simulated clinical encounters were debriefed to understand their experience incorporating the decision aid into a patient-physician encounter, barriers to use during the encounter, and strategies to overcome challenges with its integration. Input from this activity was used to make final refinements to the decision aid and identify additional accompanying implementation training materials and guidance resources required to support clinical use.
We are now conducting an implementation pilot trial that will introduce and evaluate the ** My Heart and CKD ** decision aid in 10 clinical cardiology practices in Canada. In this trial, we will evaluate implementation success, including the feasibility, acceptability, and satisfaction with use of the decision aid from the perspective of patients and health care providers, in addition to the effects of the decision aid on the quality of SDM and decision-making confidence within real world care.
Pillar 2: Indigenous Cultural Competency
We have respectfully worked with Indigenous peoples and engaged representatives of Indigenous communities in the Treaty 7 territories of the Tsuut’ina First Nation, and the Stoney Nakoda First Nation to learn how we can promote SDM using the ** My Heart and CKD ** decision aid in a culturally safe and relevant manner. Training and education of our team through courses from Indigenous Canada, Ownership Access and Privacy (OCAP) training, and resources developed and curated by the Can-SOLVE CKD network (https://cansolveckd.ca/our-work/indigenous-initiatives/) provided our team with a knowledge base from which to apply our work in this area. With support from the Can-SOLVE CKD Network Indigenous Peoples Engagement in Research Circle (IPERC) and Indigenous Liaison Manager, we were introduced and partnered with an Indigenous Knowledge Keeper and an Indigenous person with lived experience with CKD to explore the relevance of the ** My Heart and CKD ** decision aid to Indigenous people experiencing CKD and CAD.
Through in-person meetings, we introduced the objective of our project to support SDM for people with CKD and CAD. Together, we discussed personal and historical experiences of Indigenous peoples with health care, identifying racism, bias and injustices, and barriers to access to care as contributors to distrust of health care providers and the health system by Indigenous peoples. Using the ** My Heart and CKD ** decision aid and promoting SDM was viewed as an approach that could promote a space for trust-building between patients and their health care providers, and more patient-centered care. We identified that introducing SDM and implementation of the decision aid provides an opportunity to embed important teaching on cultural safety and the “6 Rs” of Respect, Relevance, Reciprocity, Relationships, Reflection, and Reconciliation (www.cansolveckd.ca) within our training and implementation program for health care providers. These teachings were integrated into our CME-accredited education program for health care providers to accompany implementation of ** My Heart and CKD **. Adjustments made to the education program included: (1) addition of patient partner insights on relevance of Indigenous cultural competency and safety within our CME program and (2) inclusion of Indigenous ways of knowing and the importance of the 6 Rs within our health care provider training materials.
Pillar 3: Incorporating EDI Principles and Health Equity
Finding optimal treatment approaches to cardiovascular disease and heart health was previously identified as a top 10 research priority by patients with CKD and health care providers in Canada.^ 17 ^ We have approached this topic using HCD^4,5,18,19^ and SDM^13,14,20^ frameworks that promote respect for each person’s unique experiences, values, and preferences for their care. These frameworks are well suited to support understanding personal and systemic contexts and to deliver equitable care and outcomes for all patients. Building upon these objectives, our project naturally progresses to embed EDI-promoting processes within implementation practices. Existing evidence demonstrates that decision aids can improve patient knowledge, reduce their decision uncertainty, improve patient experience, and value-congruent treatment decisions.^21 ?-23^ At the same time, we recognize that thoughtful implementation is also needed, so that decision aids do not exacerbate existing inequities and biases in care delivery.
We developed the ** My Heart and CKD ** website to interface with Google Translate to maximize its accessibility to users with a diversity of spoken languages. Paper-based resources for patients participating in the implementation trial were also translated into French. We identified sex and gender disparities in cardiovascular care as particularly relevant to our initiative because women frequently experience heart disease differently, and there is underrepresentation of females in past studies. Furthermore, women appear to approach health decision-making differently than men, which may be due to sociocultural factors. Research has suggested women receive much less information than they want from health professionals and a lower quality of decision support has been described being provided to females.^ 24 ^ Gender differences have also been reported in how physicians access and process information, with males relying more on heuristics, and women allocating more time to evaluating information.^ 25 ^ Recognizing these gender disparities, we established a sex and gender-balanced research team in composition of patient partners, clinicians, and researchers, and sought to achieve balanced representation of sexes of patients and care providers among study participants. In our implementation pilot trial, we have pre-specified sex and gender-based analyses to explore differences in the effect of the decision aid on outcome measures of both patient and physician experiences.^ 26 ^ Sex and gender differences will be explored, including those of patient-physician sex and gender concordance,^ 27 ^ for patient participant evaluations of decision-making quality and decisional conflict.
Pillar 4: Patient Engagement and Capacity Building
Patient partners with lived experience with CKD and CAD meaningfully contributed to the project from its outset by providing valuable input on the development of the decision aid, co-designing its implementation and evaluation plan, and in disseminating knowledge about the project to study participants and the public. Strategies used to engage patient partners included recurring full team meetings focusing on co-design and creation, participation in development of the education and implementation support resources, patient consent forms, and development of educational videos. A noteworthy contribution of patient partners has been their involvement in the development of the project evaluation framework. This involved meetings to prioritize the primary and secondary outcomes for the implementation pilot trial, and selection of the instruments used to measure patient experience, quality of SDM, and decision conflict from the patient perspective. One patient partner described the development and implementation planning meetings to the Can-SOLVE CKD Research Operations and Knowledge Translation (ROCKeT) Committee as follows:The learning process of the decision tool’s purpose was interesting: learning more about the interventions for heart disease and the relation to renal function. As a patient partner, I helped to review and reword materials and asked questions that caused the research team to “rework” a part. I don’t feel there were any challenges for me, the team was welcoming and ensured patient partners understood the importance of testing out the tool, and very open to any feedback. Team meetings were well attended, I thought, and it was nice to see everyone coming together for this project, whether you were a researcher, doctor, patient or nurse.—Patient Partner
Key Findings
Thirty-two patients and 18 physicians provided implementation perspectives for the decision aid. Among patient participants, 47% were less than 65 years of age and 47% were women. Among the physician participants, 72% were less than 50 years of age and 22% were women. Supporting quotes and themes related to implementation planning across the domains of capability, motivation, and opportunity, organized within the TDF,^ 16 ^ are shown in Table 1.
Table 1.: Insights From Patients and Clinicians According to the Theoretical Domains Framework (TDF) for Implementing the My Heart and CKD Decision Aid.
Both clinicians and patients alike saw benefits in using ** My Heart and CKD **, describing the decision aid as “good” and “useful.” Both groups suggested that it would be helpful to offer the tool in both electronic and paper formats, to accommodate personal preferences and learning styles. The primary barrier identified through interviews was related to time constraints. Whereas patients said they would be happy to take the time to use ** My Heart and CKD **, especially as in-patients, many clinicians expressed concerns about the time required to complete all steps within the decision aid during their time with a patient. Some clinicians said if the patient already had patient specific information collected and filled in, they would be happy to use ** My Heart and CKD ** to go over the results. Some clinicians suggested that nurse practitioners or other care providers, depending on the clinical setting, might be included in the implementation process to help support its use while at the same time ensuring consistent delivery of information to patients by all care providers, although this could add to the workload of nurses.
These findings led us to design the decision aid so that it would support varying use preferences and contexts, encompassing both digital and paper-based forms for use, depending on patient preferences and support available for use of digital technologies. Implementation considerations also influenced the order and arrangement of the content in My Heart and CKD to enhance its integration into the clinical environment of SDM encounters. The decision aid and implementation workflow were developed to be adaptable to variation in the amount of time and discussion that might be required between patients and their care givers or family before assessing patient knowledge and arriving at and documenting a decision.
Findings from our qualitative analyses and pre-clinical simulated patient-physician encounters indicated that additional training and implementation support materials would be needed by users to implement the decision aid. Guided by Can-SOLVE CKD’s 6-Step Pathway to Implementation Guide,^ 28 ^ we thus created a collection of documents, resources, education, and training materials to help local teams implement ** My Heart and CKD **. The specific products developed as part of the Implementation Package for ** My Heart and CKD ** and their relationship to each step on the implementation pathway are shown in Figure 1. Select materials are also available in the Supplement. An outline of the accredited CME program is shown in Figure 2.
Application of the Can-SOLVE CKD network pathway to implementation for the My Heart and CKD decision aid.
Outline of the training modules created for health care providers to support implementing the My Heart and CKD decision aid.
Discussion
We have worked across Can-SOLVE CKD’s 4 major pillars, following the six steps within the Pathway to Implementation to develop an implementation strategy for the ** My Heart and CKD ** decision aid. This decision aid is designed to facilitate SDM and support a shift toward more patient-centered care that addresses variability in risks that exist between patients and aligns care with the values and preferences of individual people living with CKD and CAD. Applying HCD brought to light several implementation themes during the decision-aid development process. The TDF allowed us to identify barriers to use as well as potential facilitators, which influenced the design of the decision aid, as well as the development of a suite of implementation training and support materials. This has prepared us to pilot test the decision aid in cardiology practices in Canada and will also support broader implementation scale and spread of the decision aid to additional practices in the future.
Implementation strategies for decision aids need to carefully balance physician expertise while making room for the patient voice in the shared treatment decision-making process. Throughout the project, patients have shaped the design of ** My Heart and CKD ** as well as implementation strategies. Patients have also been involved with selecting the measurements and instruments we will use to measure knowledge, communication, acceptability, and the quality of SDM, to ensure our intervention improves outcomes that matter to patients. Mid-iteration adjustments to the design of the decision aid were made to enhance feasibility of use and comprehension by patients and provide flexible approaches to integration within clinical workflow to increase the probability of implementation success. Patient partners play an important role in knowledge dissemination about ** My Heart and CKD ** to other patients and physicians. As one patient partner advises:I would say use the tool, go slowly, go carefully, look at all aspects and ask questions. If you don’t understand or you are asking should I, could I, would I? There’s always somebody available to answer any question you have.—Patient Partner
Strengths of our project include the insights of patients with lived experience, clinicians with experiences caring for people with CKD and CAD, and application of evidence-informed frameworks, such as HCD, the Ottawa decision support framework, and the TDF in development and implementation of the decision aid. However, we have encountered several limitations. Much of the iterative development and interviews with patients was affected by the COVID-19 pandemic, which required us to use virtual sessions and may have altered people’s preferences and experiences with use of digital health technologies. This could have either enhanced or suppressed identification of certain barriers or facilitators to implementation of a web-based tool in clinical practice. However, ** My Heart and CKD ** is highly flexible for use in different contexts and was designed with these uncertainties in mind. Patients and their health care teams can initiate tool use in either digital or paper-based contexts depending on patient technology comfort levels, ever-evolving use of technology in clinic environments, and workflows. The tool allows easy movement between the two, emphasizing flexibility as a strength to overcome the limitation.
As we are still in early stages of implementation, we do not yet know for certain how our identified barriers and facilitators will translate into real world use. It is uncertain whether the intended flexibility of ways to use the decision aid will translate into implementation success in clinical practice. However, we have created a range of support materials for different audiences and in different modalities, and in-person implementation supports to help each clinical environment determine which form of use work best for their situation. While in-person support may not be possible beyond the pilot trial (ie, a potential limitation of scale and spread planning), we do intend to collect and apply the insights and experiences gleaned from the pilot trial to refine or development resources to support future broader implementation efforts.
Implications
** My Heart and CKD ** has the potential to be effectively and sustainably implemented within cardiovascular and kidney care, with implications for how care is delivered to people with CAD and CKD. This decision aid promotes personalized, patient-centered care by providing patients with CKD and CAD and their care providers with the tools needed for SDM (Figure 3).
Infographic conveying the value of implementing the My Heart and CKD decision aid.
By mobilizing knowledge through decision support, promoting SDM in a manner that addresses known health inequities, and amplifying patient involvement and recognition of their values and preferences in decision-making, this program of work aligns with Can-SOLVE CKD’s mission to transform kidney care and foster equitable health experiences and outcomes for Canadians living with CKD.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581251389602 – Supplemental material for My Heart and CKD: Pathway to Implementing a Decision Aid for Patients With CKD and Coronary Artery DiseaseSupplemental material, sj-pdf-1-cjk-10.1177_20543581251389602 for My Heart and CKD: Pathway to Implementing a Decision Aid for Patients With CKD and Coronary Artery Disease by Julie N. Babione, Pantea Javaheri, Denise Kruger, Todd Wilson, Winnie Pearson, Maureena Loth, Violet March, Wayne Gerber, Bryan J. Har, Michelle M. Graham, Stephen B. Wilton, Krystina B. Lewis and Matthew T. James in Canadian Journal of Kidney Health and Disease
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarnak MJ Amann K Bangalore S , et al. Chronic kidney disease and coronary artery disease: JACC state-of-the-art review. J Am Coll Cardiol. 2019;74(14):1823-1838. doi:10.1016/j.jacc.2019.08.1017.31582143 · doi ↗ · pubmed ↗
- 2Finlay J Wilson T Javaheri PA , et al. Patient and physician perspectives on shared decision-making for coronary procedures in people with chronic kidney disease: a patient-oriented qualitative study. CMAJ Open. 2020;8(4):E 860-E 868. doi:10.9778/cmajo.20200039.PMC 786703133303572 · doi ↗ · pubmed ↗
- 3Wilson TA Hazlewood GS Sajobi TT , et al. Preferences of patients with chronic kidney disease for invasive versus conservative treatment of acute coronary syndrome: a discrete choice experiment. J Am Heart Assoc. 2023;12(6):28492. doi:10.1161/JAHA.122.028492/FORMAT/EPUB.PMC 1011154036892063 · doi ↗ · pubmed ↗
- 4Bazzano AN Martin J. Designing public health: synergy and discord. Des J. 2017;20(6):735-754. doi:10.1080/14606925.2017.1372976. · doi ↗
- 5Altman M Huang TTK Breland JY. Peer reviewed: design thinking in health care. Prev Chronic Dis. 2018;15(9):180128. doi:10.5888/PCD 15.180128.PMC 617890030264690 · doi ↗ · pubmed ↗
- 6Babione JN Ocampo W Haubrich S , et al. Human-centred design processes for clinical decision support: a pulmonary embolism case study. Int J Med Inform. 2020;142:104196. doi:10.1016/J.IJMEDINF.2020.104196.32947115 · doi ↗ · pubmed ↗
- 7Maguire M. Methods to support human-centred design. Int J Hum Comput Stud. 2001;55(4):587-634. doi:10.1006/IJHC.2001.0503. · doi ↗
- 8IDEO. Field Guide to Human-Centered Design. San Francisco, CA: IDEO; 2015.