Rectal diffuse large B-cell lymphoma misdiagnosed as bleeding cancer in an elderly patient
Yuchun Zhong, Qiansen Zhang, Yujie Fu, Jiusi Liu, Linhui Leng, Wei Xu

TL;DR
An elderly patient with rectal diffuse large B-cell lymphoma was initially misdiagnosed with adenocarcinoma, highlighting the challenges in diagnosing rare rectal cancers.
Contribution
This case report adds to the limited literature on primary rectal DLBCL and emphasizes the importance of considering rare malignancies in elderly patients with rectal bleeding.
Findings
Rectal DLBCL can present with hematochezia and mimic adenocarcinoma in elderly patients.
Avoiding preoperative biopsy in high-risk patients can still lead to accurate diagnosis after surgery.
DLBCL diagnosis requires histopathological confirmation for proper treatment planning.
Abstract
Primary rectal diffuse large B-cell lymphoma (DLBCL) is a rare malignancy that often closely mimics more common rectal pathologies such as adenocarcinoma or inflammatory bowel disease. This resemblance poses considerable diagnostic difficulty, and misdiagnosis may result in delayed treatment and unnecessary procedures, ultimately affecting patient outcomes. An 87-year-old female presented with intermittent hematochezia that acutely worsened two hours before admission. Physical examination identified a rectal mass located 5 cm from the anal verge. Pelvic imaging and colonoscopy were suggestive of hemorrhagic adenocarcinoma. Given the patient’s advanced age, significant anemia, and elevated bleeding risk, a multidisciplinary team decided against preoperative biopsy. Instead, transanal minimally invasive surgery was carried out for local disease control. Final histopathological analysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
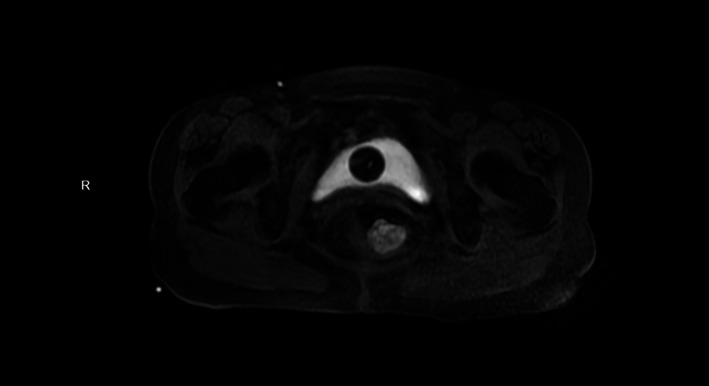 Figure 1
Figure 1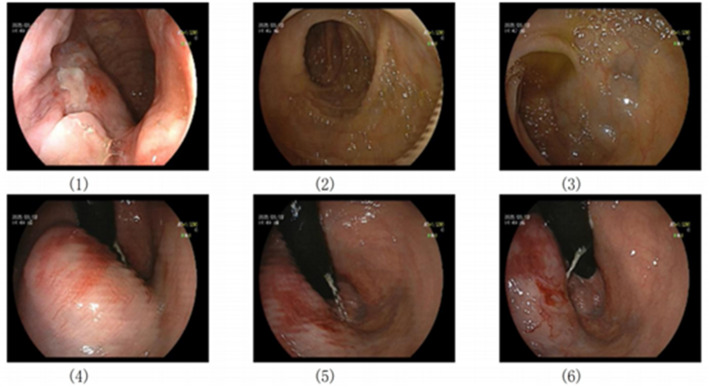 Figure 2
Figure 2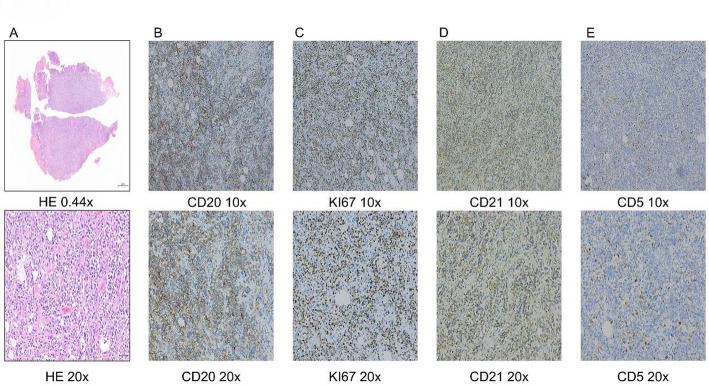 Figure 3
Figure 3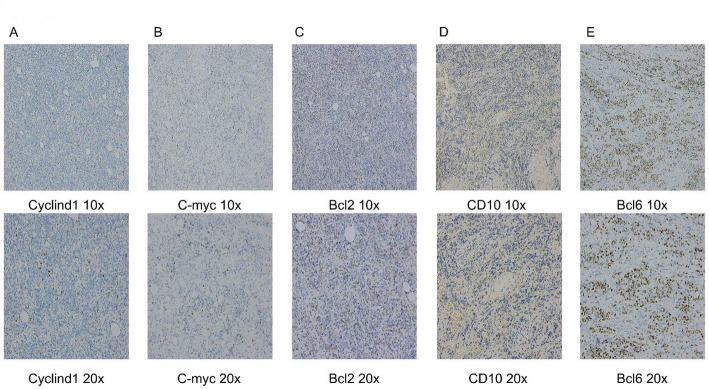 Figure 4
Figure 4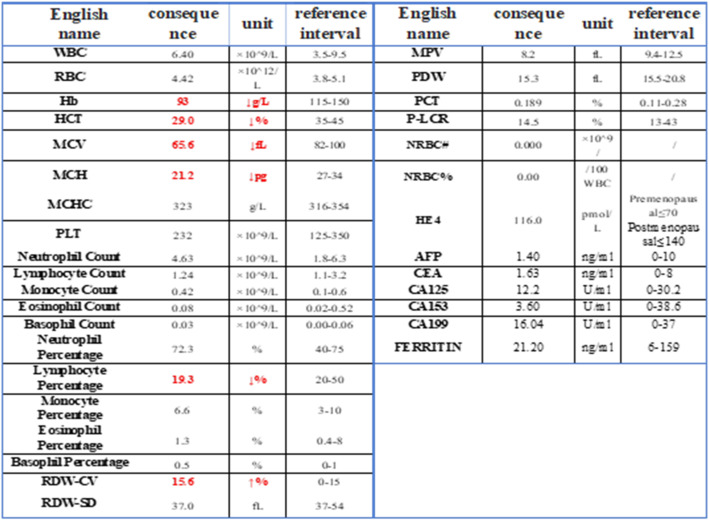 Figure 5
Figure 5- —This work was supported by the Institutional Funding Program of The Second Affiliated Hospital of Nanchang University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · CNS Lymphoma Diagnosis and Treatment · Colorectal and Anal Carcinomas
Introduction
Extranodal lymphomas, such as primary gastric and colorectal mucosa-associated lymphoid tissue (MALT) lymphoma and primary central nervous system lymphoma (PCNSL), account for approximately 30% of cases [1, 2]. Molecular characteristics vary depending on the specific subtype. For instance, in Germinal Center B-Cell like Diffuse Large B-Cell Lymphoma (GCB-DLBCL), as represented in this case, germinal center markers such as CD10 and Bcl-6 serve as key distinguishing features compared to marginal zone B-cell lymphoma (MZBL) [2]. DLBCL is a relatively common, highly aggressive malignancy of the hematolymphoid system, characterized by an age-standardized incidence rate of approximately 0.72 per 10,000 person-years [3]. Its incidence increases with advancing age, predominantly affecting elderly populations. However, primary occurrence in the rectum is exceedingly rare [4]. And the clinical presentation of rectal DLBCL often resembles that of more common rectal pathologies, such as adenocarcinoma or inflammatory bowel disease, further adding to the difficulty of differentiation [5, 6]. This misdiagnosis may delay appropriate therapeutic intervention and may lead to unnecessary medical procedures that ultimately affect patient outcomes [7]. Amid global demographic aging, we present this rare case to enhance clinicians’ recognition of uncommon pathologies in geriatric patients, ultimately contributing to improved diagnostic accuracy and therapeutic outcomes for rare diseases.
Case presentation
An 87-year-old female patient was admitted to our department from the emergency room with recurrent hematochezia (rectal bleeding) persisting for over half a month, which had acutely worsened over the preceding 2 h. The stool was bright red in color with a loose/pasty consistency, and the most recent episode was estimated at approximately 50 ml. The patient reported associated symptoms including dizziness, fatigue, and palpitations, but denied abdominal pain, distension, fever, nausea, or vomiting. Emergency digital rectal examination performed in the knee-chest position revealed a palpable mass on the right rectal wall. The mass was moderately firm in consistency, encircled approximately one-quarter of the rectal lumen, exhibited moderate mobility, and had relatively distinct borders. Blood staining the examination glove was noted upon withdrawal of the finger. Urgent complete blood count revealed: Hemoglobin: 93 g/L (Reference range: 115–150 g/L) (Table 1). Findings of pelvic magnetic resonance imaging (MRI) non-contrast and contrast-enhanced scan: Marked thickening of the right rectal wall with a protruding nodular shadow, measuring approximately 32 × 27 mm, showing isointense signal on T1-weighted images and moderately hyperintense signal on T2-weighted images. The lesion appears hyperintense on DWI and demonstrates significant enhancement after contrast administration, with blurring of the surrounding fat planes. Thus, imaging findings suggest a space-occupying lesion in the right rectal wall, consistent with changes of rectal carcinoma (Fig. 1). Based on the patient’s symptoms, physical examination findings, laboratory results, and imaging findings, a preliminary diagnosis of rectal carcinoma was considered.
Past medical history included hypertension and cerebral infarction. The patient was on long-term therapy with nifedipine and aspirin tablets. She denied any history of other gastrointestinal inflammatory or neoplastic diseases, significant personal or family medical history, or relevant travel exposure.
Fig. 1. Imaging studies: Pelvic magnetic resonance imaging (MRI) with contrast enhancement revealed marked thickening of the right rectal wall, with a protuberant nodular lesion measuring approximately 32 × 27 mm
Relevant medical laboratory examination
On admission, the patient’s vital signs were stable: body temperature 36.5 °C, blood pressure 164/66 mmHg, and pulse rate 88 beats per minute. Physical examination revealed no significant abnormalities in the head, neck, skin, mucous membranes, or superficial lymph nodes. The abdomen was soft without tenderness, rebound tenderness, muscle guarding or palpable masses.
Laboratory investigations
Blood tests revealed: hemoglobin 93 g/L (Reference range: 115–150 g/L); Hematocrit (Hct): 29.0% (Reference range: 35–45%); Mean corpuscular volume (MCV): 65.6 fL (Reference range: 82–100 fL); indicating mild anemia. Other blood parameters were normal. All Tumor markers within normal reference ranges (Table 1).
Table 1. Results of emergency blood routine and tumor markers. Red indicates abnormality
Diagnosis and treatment
To further elucidate the diagnosis, endoscopic examination was pursued. Endoscopy revealed an irregularly elevated mass approximately 5 cm from the anal verge. The lesion exhibited relatively distinct borders, an uneven surface with irregular contours, and multiple scattered bleeding points. The mass occupied approximately one-quarter of the rectal lumen circumference. The patient presented with persistent hematochezia after admission, which responded poorly to initial pharmacologic and endoscopic hemostatic measures. Furthermore, the patient was on long-term aspirin therapy for antiplatelet aggregation due to a previous cerebral infarction. Under these circumstances, although coagulation screening tests showed no significant abnormalities and hemodynamic parameters remained stable, performing an endoscopic biopsy still carried a considerable risk of secondary bleeding. Considering the patient’s advanced age, a history of cerebral infarction that may be associated with increased vascular fragility, and reduced tolerance to blood loss, the multidisciplinary team agreed that the risk of performing a biopsy for histologic diagnosis at this time outweighed its potential benefit. Therefore, the clinical decision was made to prioritize emergent hemostasis and systemic stabilization over proceeding with a biopsy (Fig. 2).
Based on the aforementioned diagnostic findings and the significant risk of hemorrhage, emergent transanal minimally invasive surgery was performed after comprehensive discussion with the patient and her family.
Fig. 2. Colonoscopic Image of the tumor
Histopathological and immunohistochemical analysis
However, definitive histopathological examination of the resected tumor tissue revealed primary rectal diffuse large B-cell lymphoma (DLBCL) (Figs. 3 and 4). HE staining revealed tumor tissue exhibiting a diffuse sheet-like growth pattern. The tumor cells were large to intermediate in size, with large nuclei displaying hyperchromatic or pale, vesicular chromatin. Prominent nucleoli were evident in the majority of cells, and abundant karyorrhexis (nuclear fragmentation) was observed. The stroma showed vascular proliferation, with some vessels exhibiting dilatation and congestion. According to the classification of DLBCL reported in the literature [8], Combined with the definitive immunohistochemical analysis of CD20, KI67, CD21, CD5, Cyclin D1, C-myc, Bcl-2, CD10, and Bcl-6 (Table 2), the tumor tissue was confirmed as rectal diffuse large B-cell lymphoma (DLBCL) of the germinal center B-cell-like (GCB) subtype (Fig. 3).
Fig. 3. Histopathology and Immunohistochemical Staining.Immunohistochemical Analysis: CD20: Diffusely positive (+);Ki-67: Positive (+), approximately 95% (indicating high proliferative index); CD21: Highlighted disrupted follicular dendritic cell meshworks; CD5: Positive (+) in background T-cells (T-cell staining noted);** A**–E Row 1: 10x (HE 0.44x); Row 2: 20x
Fig. 4. Histopathology and Immunohistochemical Staining.Immunohistochemical Analysis: Cyclin D1: Negative (-);C-myc: Positive (+), approximately 10% ;Bcl-2: Positive (+), approximately 40%; CD10: Diffusely positive (+); Bcl-6: Positive (+), approximately 70%;** A**–E Row 1: 10x ; Row 2: 20x
Table 2. Results of immunohistochemical stainingIHCHECD20KI67CD21CD5Results+++(95%)++(Tcell)IHCCyclind1C-mycBcl2CD10Bcl6Results-+(10%)+(40%)++(70%)
Follow-up
Following surgery, the patient was referred to the Department of Medical Oncology and received systemic chemotherapy with the R-CHOP regimen (rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone) for a planned 4 cycles. The treatment was well-tolerated with no grade 3 or higher adverse events reported. During subsequent regular follow-up, no signs of recurrence have been observed.
Discussion
Clinical presentation and diagnostic challenges of rectal DLBCL
Primary gastrointestinal lymphoma represents a rare malignancy; however, its incidence has been steadily increasing [9]. Within this spectrum, the rectal subtype of primary DLBCL constitutes less than 0.2% of all colorectal malignancies [10, 11]. The rectal DLBCL are typically non-specific, commonly including abdominal pain, weight loss, rectal bleeding (hematochezia), and altered bowel habits. These symptoms lack specificity and can easily mimic more common gastrointestinal disorders [12–14]. Additionally, due to this non-specific presentation, patients may initially report systemic signssuch as anemia, fever, and anorexia [12]. Patient age and gender may further influence clinical manifestations, thereby posing additional challenges to timely and accurate diagnosis. For example, the report by Ayesha Nusrat further indicates that the incidence of malignant tumors is higher in boys than in girls, and that non‑Hodgkin lymphoma (NHL) originating from the small and large intestines is associated with better overall survival compared to gastric NHL. Additionally, the types of NHL frequently observed vary across different age groups [15]. In comparison with the present case, studies by Wei Ding, Nao Imuta, and others on DLBCL have more comprehensively revealed the complexity of this disease. Existing reports on DLBCL often describe its coexistence with other types of lymphoma or solid intestinal tumors, underscoring the necessity of a comprehensive diagnostic approach once intestinal DLBCL is suspected [11, 16]. This diagnostic ambiguity often delays therapeutic intervention. In this case, the patient presented with acutely exacerbated hematochezia and anemia refractory to initial symptomatic management. Consequently, clinicians should maintain high vigilance and consider lymphoma in the differential diagnosis when encountering such symptoms [11]. In this case, the patient manifested persistent rectal bleeding with acute exacerbation, which aligns with the reported cases mentioned above.
The symptomatic overlap between rectal DLBCL and other rectal diseases represents a major diagnostic hurdle. Its clinical features may closely resemble those of rectal polyps, ulcerative colitis, and rectal adenocarcinoma, which notably complicates precise diagnostic differentiation [12, 13, 17]. Notably, in this case, contrast-enhanced MRI and visual endoscopic assessment initially suggested rectal adenocarcinoma. The endoscopically observed active tumor bleeding, combined with the patient’s advanced age, anemia, and heightened procedural bleeding risk, precluded biopsy prior to intervention.
The treatment paradigms for rectal DLBCL
Systemic immunochemotherapy (R-CHOP regimen) remains the cornerstone primary treatment for rectal diffuse large B-cell lymphoma. However, current evidence demonstrates that combination therapy integrating surgical intervention and chemotherapy may represents the more effective strategy for improving outcomes in patients with small intestinal or colorectal DLBCL [12, 18–20]. In addition, in addition to differences in treatment modalities that may lead to differences in DLBCL efficacy, the study of Georgian Halcu et al. also showed that patients with high Ki-67 had faster disease progression and shorter average survival. In this case, the Ki-67 was as high as 95%, so it needs to be vigilant [21]. Furthermore, challenges in obtaining definitive diagnostic confirmation prior to intervention and the high incidence of presenting complications (such as obstruction, perforation, or bleeding) may contribute to the initially high resection rates observed in these patients [22]. This case similarly demonstrated refractory hematochezia unresponsive to conservative interventions alongside a high preoperative suspicion of rectal adenocarcinoma that could not be definitively confirmed prior to surgical intervention.
The transanal minimally invasive surgery combined with postoperative adjuvant therapy effectively mitigated ongoing bleeding risks and avoided the physical trauma associated with abdominoperineal resection in this elderly patient. Both the patient and family members expressed strong appreciation for our treatment strategy during pre- and postoperative communications.
Consequently, this case report aims to underscore to clinicians the critical importance of recognizing both the extreme rarity of rectal DLBCL and the diagnostic c complexities arising from its complicating presentations.
Conclusion
This case highlights hematochezia as the cardinal manifestation of rectal DLBCL and underscores the critical importance of definitive histopathological confirmation in elderly patients with unexplained lower gastrointestinal bleeding to mitigate diagnostic delays. However, the extreme rarity of rectal DLBCL (< 0.2% of colorectal malignancies), its mimicry of adenocarcinoma on conventional investigations (digital rectal examination, endoscopy, and imaging), and therapeutic dilemmas arising from acute complications continue to impede optimal management. To improve the guarded prognosis of this aggressive malignancy, implementing structured preoperative diagnostic protocols and evidence-based multimodal therapeutic strategies remains imperative.
The reference list from the paper itself. Each links out to its DOI / PubMed record.