Ethnopharmacological considerations of plants traditionally used by local communities to manage maternal conditions in Tanzania: a scoping review
Mwanaidi Omary, Maryyusta Nguyamu, Jackline Nkoma, Hamisi S. Japhari, Obadia K. Bishoge, Emanuel L. Peter

TL;DR
This study explores traditional herbal use in Tanzania for maternal health, finding that few plants have scientific validation or safety data.
Contribution
The study documents 330 plant species used for maternal conditions in Tanzania and evaluates their scientific and safety evidence for the first time.
Findings
330 plant species from 82 families were identified for managing maternal conditions in Tanzania.
Only 7% of the plants had scientific evidence supporting their traditional use, and 22% had safety data confirming non-toxicity.
Abstract
Despite notable progress in maternal health and a reduction in maternal mortality rates, Tanzania still falls short of global targets. Local women increasingly use herbal medicine to manage maternal conditions, highlighting the need of documenting and evaluate these traditional practices. In this study, we aimed to identify the medicinal plants commonly used by women to manage maternal conditions and to critically evaluate the available scientific evidence regarding their efficacy and safety. A scoping review was conducted in accordance with the framework of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR). Articles were retrieved from PubMed, Web of Science, Scopus, African Index Medicus (AIM), Maternity and Infant Care (MIC), and CINAHL, covering the period from inception to July 2025. Eligible studies were screened…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
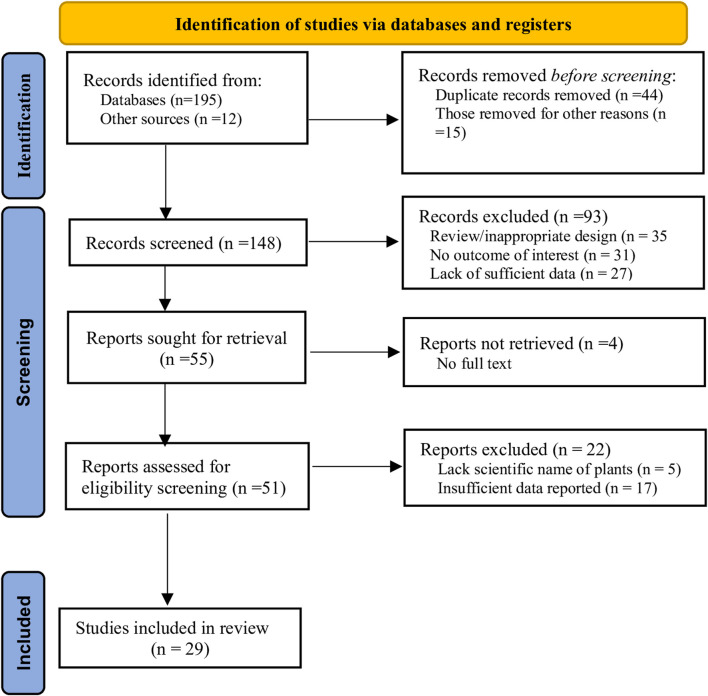 FIGURE 1
FIGURE 1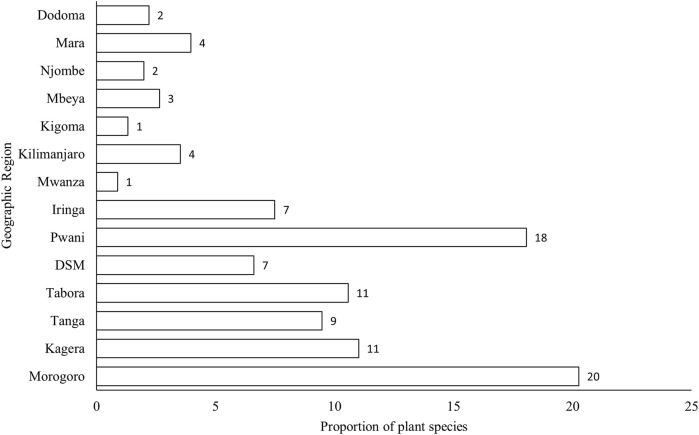 FIGURE 2
FIGURE 2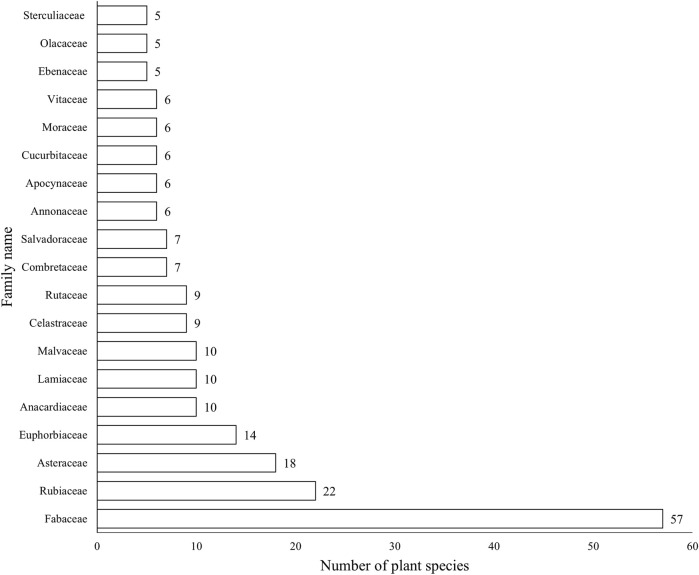 FIGURE 3
FIGURE 3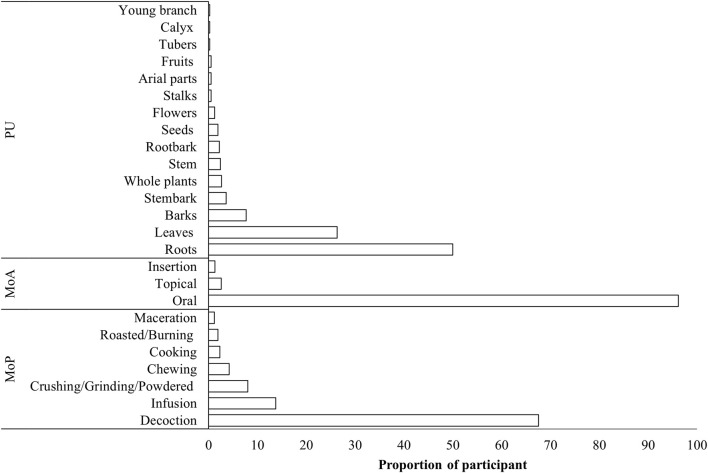 FIGURE 4
FIGURE 4| Maternal condition | Plant species (family) | TIS | TIU | Fidelity level % | References |
|---|---|---|---|---|---|
| Inducing abortion |
| 2 | 4 | 50 |
|
|
| 4 | 5 | 75 |
| |
|
| 3 | 3 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 3 | 75 |
| |
|
| 2 | 2 | 100 |
| |
|
| 3 | 4 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
| Infertility |
| 2 | 2 | 100 |
|
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 3 | 75 |
| |
| Se | 2 | 4 | 50 |
| |
|
| 3 | 3 | 100 |
| |
|
| 2 | 2 | 100 |
| |
| Menstrual problems |
| 2 | 2 | 100 |
|
|
| 2 | 2 | 100 |
| |
| Ehretia amoena Klotzsch (Boraginaceae) | 3 | 4 | 75 |
| |
|
| 2 | 2 | 100 |
| |
|
| 2 | 2 | 100 |
| |
|
| 3 | 3 | 100 |
| |
| Anemia |
| 2 | 2 | 100 |
|
| S/N | Plant name | Type of study | Extract/fractions, dose, and RoA | Pharmacological activity | Mechanism of action | References | ||
|---|---|---|---|---|---|---|---|---|
| 1 |
|
| Methanolic seed extract, 50 mg/kg p.o. | - Irregularity of the estrous cycle | - Decreased the duration of proestrus and estrus phases and increased the duration of metestrus and diestrus |
| ||
| Petroleum ether and ethanol root extracts (100 mg/kg) p.o. | - Post- ovulatory activity | Prevented nidation by up to 100% in albino rats |
| |||||
| 2 |
| Clinical trial | Leaf flour substitution, 40% obtained Fe levels 22.68 ppm, p.o. | - Antianemia activity in pregnant women | Increased MCH, MCV, and MCHC. Increased hemoglobin levels |
| ||
| Powdered | - Reduces the incidence of stunted growth | - |
| |||||
|
| Leaves and seed flour at a concentration of 100 mg per kg | - Impacted cognitive development | - Early maturation of the senses in the offspring compared to the control group |
| ||||
| Clinical trial | Up to 900 mg/day of | Galactagogue | Increased breast milk volume in early postpartum patients |
| ||||
|
| Mixture of | Induces galactagogue activity in lactating Wistar rats | - |
| ||||
| 3 |
|
| Petroleum ether bark extract at concentrations of 3.2 mg/mL to 2 mg/mL | Facilitates labor in rats | - An increase in the contractile force and the frequency of muscle contractions |
| ||
| 4 |
|
| Methanolic extract at a dose of 800 mg/kg, administered intragastrically | No effect on the fertility of male or female mice | - No change in embryo weight |
| ||
| 5 |
| Clinical trial | Two extract doses (3 and 6 mg/day), p.o. | Treats primary dysmenorrhea in female students | - Reduced pain intensity |
| ||
|
| Aqueous leaf extract at a dose of (0.5 mg/mL–4.0 mg/mL) | - Treatment of primary dysmenorrhea | - Inhibited or abolished contractions produced by acetylcholine, oxytocin, bradykinin, carbachol, or potassium chloride in quiescent uterine horn preparations isolated from estrogen- dominated rats |
| ||||
| 6 |
|
| Crude extracts of three species of Aloe; | No abortifacient activity in any of the extracts in rats | - No expulsion or resorption of fetuses |
| ||
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion in rats | Effect on the frequency of contractions |
| ||||
| 7 |
|
| Methanolic and aqueous extracts from the stem bark at doses of 1 and 100 μg mL−1 | Contraceptive efficacy in vitro | - Affected ovarian cell functioning, steroidogenesis, the activity of LH on these processes, and affected normal ovulation and fecundity, leading to contraception |
| ||
| Ether extract of castor bean seed (IC50 = 284.30 ± 5.30 μg mL−1 r = + 0.9790) | Antifertility activity in vitro | - Inhibited the viability of cultured rat Decidual Stromal Cells (DSC), and bioassay- guided fractionation led to the separation of the active constituent, a colorless crystal |
| |||||
|
| Seed extract | - Anti- implantation and abortifacient effects | |
| ||||
| Clinical observation | The seed extract was administered as a single oral dose of 2.3 g–2.5 g | Contraceptive efficacy in women volunteers | |
| ||||
|
| An ether- soluble fraction of a methanol extract of seeds administered at doses of up to 1.2 g/kg and 600 mg/kg | Anti- implantation and anti- conceptive activities in adult female rats and rabbits | Action at several sites, including direct effects on the endometrial implantation site, on the oviduct, and/or disruption of the estrogen/progesterone balance |
| ||||
| Clinical observation | Oral dose of castor oil (60 mL) | Induces labor in women patients (prospective evaluation) | - |
| ||||
|
| Castor oil | Induces labor | - Increase in the contractile activity of the castor oil– exposed myometrial strips |
| ||||
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion in rats | Effect on the force of uterine contractions |
| ||||
| 8 |
|
| Seed extract was administered orally, 6 mL (in baboons) or 3 mL (monkeys) for 6 days | Termination of pregnancy | - Decline of chorionic gonadotrophin (CG) and progesterone |
| ||
| 0.6 mL of seed extracts, p.o. | Termination of pregnancy in rats | - Increases in the weight of mesenteric lymph nodes |
| |||||
| Seed extract at a dose of 3 to mL, p.o. | Induces abortion in primates | |
| |||||
| Ethanolic extract at conc. in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion in rats | - Effect on the frequency of contractions |
| |||||
| 9 |
|
| Aqueous extract at doses of (200 mg/kg–1,000 mg/kg body wt.), p.o. | Beneficial effects on the red blood cells at low doses (200 mg–400 mg/kg) in Wistar albino rats | - |
| ||
| | | Clinical trial | Extract at doses 1,000, 1,500, and 2,000 mL/day, p.o. | Improves hematopoietic parameters in mildly anemic adults | - |
| ||
| 10 |
|
| Aqueous extracts (100 mg/mL–400 mg/mL) | Induces abortion | Increases in uterine smooth muscle cell contractility at the tested dose |
| ||
| 11 |
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | Effect on the force of uterine contractions |
| ||
| 12 |
|
| Aqueous extracts (100 mg/mL–400 mg/mL) | Induces was abortion | Increases in uterine smooth muscle cell contractility at the tested concentration range of 100 to 400 mg/mL |
| ||
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | - Effect on the force of contractions |
| ||||
| 13 |
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | Effect on the force of uterine contractions |
| ||
| 14 |
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | - Effect on the force of uterine contractions |
| ||
| 15 |
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | - Effect on the force of uterine contractions |
| ||
| 16 |
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | Effects on the force of contraction |
| ||
| 17 |
|
| Ethanolic extract at concentrations in the organ bath: 0.04, 0.14, 0.44, and 1.40 mg/mL | Induces abortion | - Effects on the frequency of uterine contractions |
| ||
| 18 |
|
| Aqueous extract at a high dose of 2,000 mg/kg/day | Abortifacient and subfertility effects in female mice | Disrupted the estrous cycle and blastocyst implantation without teratogenesis |
| ||
| | Clinical observation | A dose of 500 mg of dried ginger capsules twice daily | Improves breast milk volume in women during the immediate postpartum period | - |
| |||
| 19 |
| Clinical observation | Hot and sour soup twice a day for a week | Promotes breastfeeding in postnatal mothers | - |
| ||
| 20. M |
|
| The leaves of | Alleviates dysmenorrhea | Inhibited oxytocin- induced uterine contractions in rats |
| ||
| 21 |
|
|
| Increases women's fertility | Restored estrous cyclicity, induced ovulation, reduced blood glucose levels and oxidative stress, improved the lipid profile and sex hormone levels, and prevented ovarian damage in PCOS rats |
| ||
|
| Aqueous extract of | Treats infertility | Reduced s the time frame for implantation in treated rats |
| ||||
| 22 |
|
| Crude extract at doses of 500 mg/kg–750 mg/kg IP | No abortifacient activity in pregnant rats | No expulsion or resorption of the fetuses |
| ||
| 23 |
|
| Aqueous extract (infusion, proportion C. cajan and A. hispidum proportion 1:1.3). Doses of 0, 150, 300, and 600 mg/kg | No abortion effects in pregnant rats | - No significant change in the mean weight of the fetuses |
| ||
| No. | Plant names | Study type | Toxicological evaluations | References |
|---|---|---|---|---|
| 1 |
|
| A 13-week oral toxicity in Sprague–Dawley rats showed no mortalities at the tested dose of up to 36,000 ppm |
|
| 2 |
|
| Approximately three studies on acute oral toxicity tested doses ranging from 200 mg/kg to 2,000 mg/kg of the methanolic (70%) crude extract of seeds, which were nontoxic to Wistar albino rats and mice |
|
| The lethal dose (LD50) of the abrin-derived peptide was found to be 2.25 mg/kg of body weight in normal mice |
| |||
| 4 |
|
| Acute toxicity: mild analgesia was noted at doses ranging from 625 to 5,000 mg/kg; more autonomic system effects were noted at higher doses |
|
| 5 |
|
| Acute toxicity: decoction of leaves had an LD50 value of 1,553.61 mg/kg, classified as low toxicity |
|
| 6 |
|
| Genotoxicity: no genotoxic or mutagenic effects at doses of 500 and 1,000 mg/kg |
|
| 7 |
|
| Acute toxicity: The LD50 of the hydroethanolic leaf extract and infusion was greater than 2,000 mg/kg. The oil did not cause any skin irritation |
|
| Reproductive toxicity: leaf and seed flour were found to be safe to pregnant women at a concentration of 100 mg/kg |
| |||
| 9 |
|
| Acute toxicity: Two studies showed that an acute dose of 5,000 mg/kg of stem extract in rats and mice resulted in no mortality or gross abnormalities. |
|
| 10 |
|
| Acute toxicity: The LD50 was above 2,000 mg/kg for the stem bark extract |
|
| 11 |
|
| Single or repeated dosages of 5, 2.5, and 0.25 g/kg of dried leaves or stems were toxic to Nubian goats. Features of toxicity included inappetence, locomotor disturbances, paresis, especially of the hind limbs, and recumbency |
|
| Daily oral doses of up to 5 g/kg per day of the dried leaves show signs of toxicity in goats in a time- and dose-dependent manner |
| |||
| 12 |
| Clinical trial | No toxic effects at a dose of 800 mg every 8 h a day for 4 days in healthy men |
|
|
| Acute toxicity: ethanolic root extract was non-toxic, and the oral median lethal dose in mice was >1,600 mg/kg |
| ||
| 13 |
|
| Acute toxicity: death and other clinical signs of toxicity at doses of 300, 1,000, and 2,000 mg/kg in rats (LD50 was 500 mg/kg, hence toxic at high doses) |
|
| Acute toxicity: no sign of toxicity in acute toxicity study at doses of up to 3,000 mg/kg of aqueous leaf extract in rats |
| |||
| Sub-chronic toxicity: leaf extract in mice did not result in death or alterations of body weight at doses of 500 mg/kg by gavage |
| |||
| 14 |
|
| Chronic toxicity: oral aqueous extract did not result in mortality or visible signs of toxicity at a dose of 250 mg/kg |
|
| 15 |
|
| Acute toxicity: the methanolic extract did not result in mortality up to a dose of 3,500 mg/kg in mice and rats |
|
| 16 |
|
| Sub-acute toxicity: methanolic stem bark extract at 600 mg/kg was well-tolerated |
|
| Acute toxicity: the extract did not show any toxicity up to 2,000 mg/kg, but above this dose, the mice exhibited an increased respiratory rate and scruffy hair |
| |||
| 17 |
|
| Acute toxicity: leaf extract did not result in mortality, and noted alterations in weight and behavioral abnormalities were observed at oral doses (15.0 g/kg and 11.3 g/kg) |
|
|
| Chronic toxicity: ethanolic root extract to male and female Wistar rats showed no sign of toxicity when administered at doses of 0.2 or 1.0 g/kg |
| ||
| | | Acute toxicity: aqueous extract was safe at a dose of 2,000 mg/kg |
| |
| 18 |
|
| Acute toxicity: The extract at a dose of 10 g/kg did not result in mortality |
|
| 19 |
|
| Cytotoxicity: the extract was the least toxic with an LC50 of 0.17 mg/mL |
|
| 20 |
|
| Aqueous and organic extracts were toxic to brine shrimp (LD50 < 1,000 μg/mL) |
|
| The ethanolic extract was nontoxic with an LC50 value of 38.51 in a brine shrimp lethality assay |
| |||
| 21 |
|
| Cytotoxicity: persica mouthwashes are toxic to macrophages, epithelial cells, fibroblasts, and osteoblasts in a concentration-dependent manner |
|
| 22 |
|
| Acute toxicity: the extract did not show any overt sign of toxicity at a dose of 2,000 mg/kg |
|
| Acute toxicity: the extract did not show any sign of toxicity in mice at doses of up to 5,000 mg/kg |
| |||
| 23 |
|
| Acute toxicity: mice did not show any form of morbidity or mortality at a dose of 10,000 mg/kg of leaf extract |
|
| 24 |
|
| The ethanolic extract was toxic to mice at doses higher than 1,000 mg/kg body weight in an acute toxicity study |
|
| 25 |
|
| Acute toxicity: the root bark extract exhibited no toxic effects at 400 mg/kg |
|
|
| Total oil and its fractions showed mild to moderate cytotoxicity in a brine shrimp lethality bioassay with LC50 = 27.3 μg/mL |
| ||
| 26 |
|
| A methanol leaf and aerial part extract at doses of 100 and 300 mg/kg showed renal hemorrhage and inflammation, and hepatic inflammation in a sub-chronic toxicity study |
|
| 27 |
|
| The extract was nontoxic, with an LC50 value of 424 μg/mL for DCM and 557.92 μg/mL for the ethanol extract |
|
| 28 |
|
| Aqueous and organic extracts of the stem bark were non-toxic to brine shrimp (LD50 > 1,000 μg/mL) |
|
| In an acute toxicity study, no mortalities were observed up to a dose of 2,000 mg/kg of the fruit extract |
| |||
| No acute oral toxicity was observed, and the extracts were considered to be safe at a dose of 3,000 mg/kg |
| |||
| 29 |
|
| Root extract exhibited high toxicity with LC50 values below 12.7 μg/mL in a brine shrimp toxicity test |
|
| 30 |
|
| Chronic toxicity: pulp extract was well-tolerated at the tested dose of 1,000 mg/kg daily for 6 months |
|
| No evidence of clinical signs in rats at a dose of 2,000 mg/mL in acute oral toxicity |
| |||
| In an acute toxicity study, the extract was found to be safe up to 2,000 mg/kg orally |
| |||
| In a brine shrimp toxicity study, the stem bark extract had an LC50 of 516.4 μg/mL, which was considered to be weakly toxic |
| |||
| 31 |
|
| Leaf extracts at a dose of 1,200 mg/kg were shown to be non-toxic in an acute toxicity study |
|
| 32 |
|
| No mortality or visible signs of toxicity at doses of the aqueous extract of 62.5, 125, and 250 mg/kg for 6 months |
|
| 33 |
|
| The extract was non-toxic to mice up to 5,000 mg/kg in an acute toxicity study |
|
| 34 |
|
| The LD50 in mice was above 500 mg/kg |
|
| 35 |
|
| Acute toxicity: no mortality or signs of toxicity were recorded at 5,000 mg/kg |
|
| The essential oil from the stem bark was toxic, with an LC50 value of 1.0009 (µg/mL) in a brine shrimp lethality test |
| |||
| 36 |
|
| Acute toxicity: the aqueous and methanol extracts did not produce any toxic signs or mortality at a dose of 2,000 mg/kg in rats |
|
|
| Cytotoxicity: the hydroethanolic extracts showed low toxicity (IC50 > 500 μg/mL, 24 h) against HepG2 cells |
| ||
| 37 |
|
| Genotoxicity and maternal–fetal safety experiment; the dried leaf extract at doses of up to 1,200 mg/kg did not induce maternal toxicity, and it was neither embryotoxic nor fetotoxic |
|
|
| Acute toxicity: the LD50 value of neem oil was 31.95 g/kg by the oral route, which is nontoxic |
| ||
| Clinical trials | No sign of toxicity to any of the subjects treated with 250 mL of the extract daily (morning and evening) for over 3 months |
| ||
|
| No mortality in mice treated with neem oil for 90 days at doses of 177, 533, or 1,600 mg/kg/day |
| ||
| Acute toxicity: the stem bark extract produced toxicity at high doses of >800 mg/kg |
| |||
| 38 |
|
| LD50 above 5,000 mg/kg for the aqueous or alcoholic calyces extract |
|
| 39 |
|
| No toxic effects were noted for doses of up to 300 mg/kg in experimental chicks |
|
| 40 |
|
| No maternal toxicity or deaths were observed after treatment with latex at a concentration of 0.05% |
|
| 41 |
|
| Acute toxicity: LD50 was 2,000 mg/kg for the aqueous extract |
|
| 42 |
|
| The single oral administration of the extract at a dose of 300 mg/kg did not cause any abnormal behavior in rats |
|
| 43 |
|
| The extract was moderately cytotoxic with a CC50 of 96.7 μg/mL |
|
| The ethanol extract was categorized as mildly toxic (LC50 32.0 μg/mL) |
| |||
| 44 |
|
| Acute toxicity: the LD50 of the extract was above 5,000 mg/kg |
|
| Acute toxicity: The methanol extract of leaves exhibited mild toxic effects in mice at a dose of 5,000 mg/kg |
| |||
| 45 |
|
| Acute toxicity: the phorbol ester showed varied degrees of toxic reactions in a dose-dependent manner; 21.26 mg/kg–36 mg/kg |
|
| The seed extract at 0.05, 0.5, and 1 g/kg/day showed signs of toxicity in Nubian goats and sheep |
| |||
|
| No clinical and biochemical signs of toxicity were observed when the leaf extract was administered at 2,000 mg/kg for 21 days |
| ||
| The seed extract showed mortality in a time- and dose-dependent manner (1 mg/kg–30 mg/kg) |
| |||
| 50% protein supplement level of |
| |||
| 46 |
|
| The LD50 of the aqueous and ethanolic extracts was greater than 2,000 mg/kg |
|
| 47 |
|
| No signs of toxicity in mice after being supplemented with 10% conc. in food |
|
| Acute toxicity: aqueous extract had an LD50 greater than 5,000 mg/kg |
| |||
| 48 |
|
| Acute toxicity: the LD50 was greater than 2,000 mg/kg |
|
| 49 |
|
| Acute toxicity: the LD50 was up to 8,000 mg/kg |
|
| 50 |
|
| Acute toxicity: The LD50 of the crude fruit extract was greater than 1,000 mg/kg |
|
| 51 |
|
| Acute toxicity: the extract had an LD50 greater than 2,000 mg/kg |
|
| 52 |
|
| Acute toxicity: no deaths occurred when the aqueous and methanolic root extracts were administered orally to mice in doses of up to 5 g/kg |
|
| No evidence of toxicity or death in acute and sub-acute toxicity tests in rats at maximum tolerated doses (MTDs) of 5,000 and 2,000 mg/kg body weight, respectively |
| |||
| Ginger oil was not toxic to male or female rats following sub-chronic oral administration of up to 500 mg/kg per day |
| |||
| 53 |
|
| Acute toxicity: onion coat colorant (OC) at doses of 2,500, 5,000, 7,500, and 10,000 mg/kg did not result in mortality |
|
| 54 |
|
| An acute and sub-chronic toxicity study showed that the polyherbal drug (a mixture of the seeds of |
|
| 55 |
|
| The ethanolic extracts of polyherbal drug comprised of |
|
| 56 |
|
| The ethanolic extracts of the tegument and seeds were safe in |
|
| Leaf hydroalcoholic extracts at doses of 100, 300, or 1,000 mg/kg did not induce toxicity after repeated exposure for 28 days in rats |
| |||
| 57 |
|
| Lemon extract was safe for all animal species up to the maximum proposed use levels of 1,000 mg/kg of complete feed and 250 mg/kg of drinking water |
|
| 58 |
|
| An acute and sub-chronic toxicity study showed that the polyherbal drug (a mixture of cloves of |
|
| 59 |
|
| No sign of acute and sub-acute toxicity from the ethanolic leaf extracts at doses of 5,000 mg/kg b.w. and up to 1,200 mg/kg, respectively |
|
|
| Acute toxicity: the aqueous extract of the 50:50 mixture of |
| ||
| 60 |
| Clinical trial | In a pilot randomized positive-controlled trial, aloe syrup was safe and well-tolerated at a dose of 10 mL/d |
|
|
| No acute and sub-acute toxicity effects of Aloe syrup at a maximum concentration of 3,330 mg/kg body weight in rats. The LD50 was higher than 15,000 mg/kg body weight in this acute toxicity study |
| ||
| Methanolic flower extracts revealed no apparent signs of toxicity, nor did they result in death in albino rats in an acute toxicity study at doses of 200 mg/kg, 2, 4, 8, and 10 g/kg |
| |||
| No death or apparent behavioral changes in acute and sub-acute oral toxicity tests at doses of up to 5,000 mg/kg and 800 mg/kg, respectively |
| |||
| Hydroalcoholic leaf extracts were safe in acute and sub-acute toxicity studies at doses of up to 2,560 mg/kg when administered to chicks |
| |||
| 61 |
|
| Acute toxicity: The extract at 2,000 mg/kg did not show any signs of toxicity in mice |
|
| 62 |
|
| Aqueous, methanol, ethyl acetate, and n-hexane extracts from the leaves, roots, and fruits did not show acute toxicity at the highest tested concentration of 1,000 mg/kg in mice |
|
| 63 |
|
| The whole plant extract was highly toxic to brine shrimp, with an LC50 value of 19.1 |
|
| 64 |
|
| The root extract exhibited low toxicity to brine shrimp, with LC50 values between 45.4 and 95.4 μg/mL at doses between 100 and 1,600 mg/kg |
|
| 65 |
|
| Aqueous and ethanolic root extracts were also found to be safe at 2,000 mg/kg in an acute toxicity study in Sprague–Dawley rats |
|
| 66 |
|
| Cytotoxicity results showed that the extract was less toxic to HeLa cells at concentrations of up to 35 mg/mL |
|
| 67 |
|
| An acute toxicity test showed that the extract was slightly toxic, with an estimated median lethal dose of 1,767.77 mg/kg body weight |
|
| Ethanolic stem bark was toxic to brine shrimp and caused chromosomal damage in rat lymphocytes, with an LD50 value of 24.12(µg/mL) |
| |||
| 68 |
|
| The methylene chloride extract of the leaves did not cause any acute toxicity in mice at a dose of 5 × IC50 |
|
| 69 |
|
| Cytotoxicity: the lethal concentration (LC50) for the aqueous extract was 0.476 mg/mL, which was relatively high (low toxicity) compared to the highly toxic berberine LC50 of 9.80 μg/mL |
|
| 70 |
|
| Sub-acute toxicity: the methanol stem bark extract was slightly toxic to the liver |
|
| 71 |
|
| The extracts were non-cytotoxic up to a test dose of 100 μg/mL |
|
| 72 |
|
| The methanolic bark extract was shown to be non-toxic in a brine shrimp bioassay with 8.33% and 15.18% mortality rates after 24 h and 48 h, respectively |
|
| 73 |
|
| The aqueous bark extract did not show any signs of toxicity when administered orally up to 2,000 mg/kg, but rats died when injected intraperitoneally with doses of 1,000 mg/kg |
|
| 74 |
|
| Acute and sub-acute toxicity study: no mortality or clinical signs of toxicity in ethyl acetate-soluble proanthocyanidins of the immature inflorescence at the dose of 2,000 mg/kg body weight in acute and 1.75, 3.5, 7, and 14 mg/kg body weight in sub-acute toxicity studies |
|
| Fermented virgin coconut oil was safe in treated rats at a dose of 5,000 mg/kg in acute, sub-chronic, and chronic studies |
| |||
| 75 |
|
| The extract of dry leaves presents cytotoxicity and low maternal toxicity at concentrations of 500, 1,000, or 2,000 mg/kg |
|
| In acute toxicity and sub-acute toxicity studies, the seed extract revealed no mortality, morbidity, or abnormal pathological or biochemical alterations in Wistar rats at doses of up to 1,000 mg/kg |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEthnobotanical and Medicinal Plants Studies · Phytochemistry Medicinal Plant Applications · Complementary and Alternative Medicine Studies
Introduction
1
Globally, maternal mortality remains a pressing concern, with nearly 800 women estimated to die each day from preventable complications linked to pregnancy and childbirth. A large proportion of these deaths occur in low- and lower-middle-income countries (WHO, 2023). Tanzania has made notable progress in reducing its maternal mortality ratio (MMR), from approximately 530 deaths per 100,000 live births in 2015/2016 to 104 per 100,000 live births in 2022 (TDHS, 2022). Although this decrease in the MMR is a significant achievement, the figure remains above the Sustainable Development Goal (SDG) target 3.1, which aims to lower maternal death to less than 70 maternal deaths per 100,000 live births by 2030 (UN, 2023). Tanzania’s success is attributable to increased political commitment, an increased number of emergency obstetric and newborn care (EmONC) facilities, a growing health workforce, a strengthened obstetric referral network, capacity building, mentorship, and the conduct of maternal and perinatal death reviews and surveillance at all levels (Africa CDC, 2025). Sustaining the current gain in MMR reduction and achieving the SDG targets requires innovative strategies tailored to the local context, such as structured integration of traditional and herbal medicines, especially in regions where such practices are culturally significant and accessible (TDHS, 2022).
Traditional medicine, especially herbal remedies, has long been used by women of reproductive age to manage pregnancy-related conditions (Japhari et al., 2025; Makombe et al., 2023). These remedies are often valued for their accessibility, affordability, and potential to alleviate symptoms such as nausea, fatigue, and stress (Mudonhi and Nunu, 2022). Nonetheless, without proper regulation, quality assurance, and integration into formal health systems, their safety and effectiveness remain uncertain. For instance, studies from Zambia and other countries in Sub-Saharan Africa have documented the common use of plants such as lemons for nausea/vomiting and the common cold, soybean to boost energy, ginger (Zingiber officinale Roscoe; family: Zingiberaceae) for the common cold and nausea/vomiting, and neem (Azadirachta indica A. Juss.; family: Meliaceae) to prevent pregnancy and as an abortifacient (Dika et al., 2017; Hajj et al., 2020; John and Shantakumari, 2015).
Persistent contributors to maternal mortality, including postpartum hemorrhage, infections, hypertensive disorders, delivery complications, and unsafe abortion, remain difficult to control through conventional measures alone (WHO, 2023). This situation thus requires exploring local, innovative solutions to address maternal conditions. Although several ethnopharmacological surveys conducted in Tanzania highlight that women use medicinal plants for managing maternal conditions, recording detailed knowledge of plant species, preparation techniques, and routes of application (Abdallah et al., 2007; Dika et al., 2017; Kessy and Msalale, 2020; Kingo and Maregesi, 2020; Millinga et al., 2022; Moshi et al., 2012; Shangali et al., 2008), scientific evidence to validate their efficacy and safety remains largely unknown (Ahmed et al., 2018). Moreover, there has been no comprehensive review mapping the pharmacological and toxicological evidence of these plants. This situation underscores the need for a systematic review of medicinal plants used for maternal health in Tanzania, along with a critical evaluation of the available pharmacological and toxicological data. The present scoping review addresses this gap by cataloging medicinal plants that are traditionally used for maternal conditions and appraising the extent to which their use is supported by scientific research. This approach provided insights into plant species, their traditional applications, and available scientific evidence validating their use, which not only informs priority plants for future research but also influences practice and policy.
Methods
2
Review procedures
2.1
In this study, we followed the framework of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) (Tricco et al., 2018), ensuring transparency and reproducibility in the review process.
Data sources and selection criteria
2.2
Relevant articles were identified through systematic searches of the PubMed, CINAHL, Scopus, African Index Medicus (AIM), and Maternity and Infant Care (MIC) databases, covering all available publications up to July 2025. The primary search used keywords grouped into three categories; the first category included “medicinal plant (s),” “herbal medicine,” “traditional medicine (s),” and “traditional therapy”; the second category included “maternal condition (s)” and “maternal health”; and the third category included “Tanzania” and “United Republic of Tanzania.” The three search categories were combined with the Boolean logic term “AND,” whereas the keywords within each category were combined with “OR.” The secondary search paired the names of individual plants with specific maternal conditions to obtain experimental evidence and toxicity profiles. The searches were updated before the final synthesis to include the most recent studies.
Screening was carried out independently by two reviewers using the Rayyan web tool (Ouzzani et al., 2016). Two independent reviewers (MO and HS) screened titles and abstracts to identify eligible articles using the predefined criteria. The full texts of the eligible articles were obtained and assessed against the inclusion and exclusion criteria. Any disagreements between the reviewers during the full-text assessment were resolved through discussion and consensus, and when no resolution was reached, a third reviewer (ELP) was involved in the final decision. Articles were considered eligible if they (1) were ethnomedical surveys conducted in Tanzania, (2) reported plants used traditionally by Tanzanian communities, (3) reported ethical approval, (4) were published in either English or Kiswahili, because these are the official languages of the United Republic of Tanzania and it is expected that the majority of research workers in ethnopharmacology can adopt local languages to engage with traditional healers and the general community. Studies were excluded if they (1) lacked the binomial Latin name of the plants, (2) did not report the outcome of interest, or (3) were review articles without primary data.
Quality assessment
2.3
The scientific names of all the reported species were cross-checked with the World Flora Online database at https://wfoplantlist.org/online.org. Any discrepancies between the reported and verified names were noted and tabulated.
Data synthesis and reporting
2.4
Extracted data included Latin binomial names, plant family, vernacular names, voucher number, maternal conditions for which the plants were used, other reported uses, plant part(s), traditional method(s) of preparation, and geographical distribution. Where experimental evidence was available, details such as the extract type, dose, route of administration (RoA), test system (animal or human), mechanisms of action, and toxicity outcomes were captured. The extracted data were migrated to Microsoft Excel, summarized into descriptive statistics, and presented in tables, charts, and spatial mapping. Validation of traditional claims and safety was reported in thematic and tabular forms.
Ethnopharmacological indices
2.5
Two indices were applied to quantify ethnobotanical importance:
- Fidelity level (FL): this index measures how consistently a species is reported for a specific maternal condition relative to all its uses; FL= (Ns/FCs) × 100, where Ns is the number of informants citing the plant for a particular use and FCs is the total number of informants who mentioned the plant for any use (Andrade-Cetto and Heinrich, 2011). In this review, the authors of the retrieved articles (Ns) were regarded as informants to facilitate FL calculation.
- Relative frequency of citation (RFC): This index reflects the popularity of a species based on the proportion of informants who mention it. It is obtained by dividing the number of informants mentioning the use of species X by the total number of informants (Leonti, 2022).
Results
3
Summary of the studies included
3.1
A total of 207 articles were retrieved from databases and through a manual search. These articles were assessed for relevance and screened against the predetermined inclusion criteria. Consequently, 29 articles were finally included (Figure 1). The majority (20) of these articles were ethnomedicinal/ethnobotanical surveys conducted in different regions in Tanzania; five (05) articles were clinical trials, and four (04) were experimental studies.
Flow diagram of the screened, included, and excluded studies.
Traditional use of plants for maternal conditions
3.2
Approximately 330 plant species from 82 families were reported for the traditional management of maternal conditions in Tanzania. Supplementary Table S1 summarizes key information that includes the scientific name of the plant species, their family, local name, voucher number, region, parts used, method of preparation (MoP), RoA, and other uses (Supplementary Table S1).
Distribution of medicinal plants
3.3
The recorded medicinal plants (330) were from 14 regions in Tanzania. The majority (20%) of the medicinal plants used for maternal conditions were found in the Morogoro region, whereas the lowest percentage (1%) was reported in the Mwanza region (Figure 2).
Distribution of medicinal plants in regions in Tanzania.
Diversity of medicinal plants
3.4
A total of 82 plant families were reported by local communities in Tanzania to be used in the management of 11 maternal conditions. The top recorded families were the following: Fabaceae 17% (57 species), Rubiaceae 7% (22 species), Asteraceae 5% (18 species), Euphorbiaceae 4% (14 species), Anacardiaceae 3% (10 species), Lamiaceae 3% (10 species), and Malvaceae 3% (10 species) (Figure 3).
Plant families with high diversity.
Methods of preparation (MoP), modes of application (MoA), and plant parts used (PU)
3.5
The most common MoP for the remedies was decoction (68%), followed by infusion (14%), crushing/grinding (8%), chewing (4%), cooking (2%), roasting/burning (2%), and maceration (1%). The oral route (96%) was the most common MoA, followed by topical applications (3%) and insertion of remedies into the vagina (1%). The most commonly utilized plant part was the root (50%), followed by leaves (26.3%), bark (7.7%), stem bark (3.6%), the whole plant (2.6%), the stem (2.4%), root bark (2.2%), seeds (1.9%), and flowers (1.2%). Other plant parts used included stalks, aerial parts, and fruits (0.5% each), along withtubers, calyxes, and young branches (0.2% each) (Figure 4).
Methods of preparation, modes of application, and plant part used.
Ethnopharmacological indices
3.6
Fidelity level (FL)
3.6.1
The FL is grouped according to the maternal conditions reported. Each maternal condition was mentioned by at least two informants. According to Table 1, A. indica had the highest number of informants for any use and for specific use compared to the other plant species identified for abortion.
Relative frequency of citation (RFC)
3.6.2
Approximately 330 plant species were recorded in the reviewed articles. The plant species with the highest number of citations was A. indica (five citations), followed by A. senegalensis, R. communis, C. cajan (L.), S. brevispica, S. longepedunculata, V. infausta, C. febrifuga, Z. chalybeum, and Aloe sp., with four citations each. These plants were used for 12 maternal conditions, namely, menstruation problems, labor induction, abortion, lactation, pregnancy disorders, infertility, placenta expulsion, uterine problems, anemia, mastitis, galactagogue, and contraception. It should be noted that the reported medicinal plants treat two or more maternal conditions.
Sterility/infertility (117 species) and menstrual disorders (114 species) were the most frequently treated conditions, which highlights their high cultural salience and perceived therapeutic priority in traditional healthcare systems. Moderate numbers of plant species were associated with abortion care (66 species), labor induction (43), and galactagogue use (35), reflecting the broad reliance on herbal remedies throughout pregnancy and childbirth. Fewer species were reported for conditions such as pregnancy complications (20 species), expulsion of the placenta (12), and general uterine problems (9). Rarely reported conditions included mastitis (6 species), miscarriage (5), vaginal prolapse (3), and traditional contraceptive practices (2), suggesting either limited specialized knowledge or underreporting in these areas (Supplementary Table S1).
Medicinal plants cited include the following: Aloe spp. (A. vera and A. lateritia), which were widely used in the coastal and lake regions to regulate menstruation, induce abortion, and support lactation. Bidens pilosa appeared frequently in Lake Zone surveys as an abortifacient and menstrual inducer. Combretum molle was one of the most recurrent species and was used in Pwani, Morogoro, and Tabora for the treatment of infertility, excessive menstrual bleeding, and childbirth facilitation. Combretum zeyheri similarly addressed heavy menstrual flow and infertility in Tanga and Tabora. Cussonia zimmermannii was reported in Pwani for postpartum hemorrhage and labor induction, whereas Ehretia amoena was widely noted in coastal regions for dysmenorrhea, menorrhagia, and infertility. Elaeodendron schlechterianum (in Mara and Tabora) was used for infertility and menstrual pain, and Guizotia scabra was commonly cited as an abortifacient in Kagera and Mara. Jatropha curcas had a specialized role in treating mastitis in Kagera. Kigelia africana (in Mara and Morogoro) was used to stimulate lactation and manage heavy bleeding. Lannea stuhlmannii/L. schweinfurthii (in Morogoro, Pwani, and Kilimanjaro) were important remedies to treat infertility and facilitate childbirth. Maytenus spp. (in Pwani, Tanga, and Tabora) were widely used for infertility and dysmenorrhea. Microglossa pyrifolia supported postpartum care and the treatment of uterine prolapse in Pwani.
Several species of Rhus were also prominent: Rhus natalensis (in Pwani, Tanga, and Kigoma) was used for menstrual disorders, infertility, and pregnancy regulation, and Rhus vulgaris (in Kagera) was used to treat infertility and support childbirth. Sorindeia madagascariensis (in Pwani and Tanga) was frequently used for heavy menstrual bleeding and prolapse. Within the Asteraceae family, Vernonia amygdalina (in Kagera and Kigoma) served as an abortifacient, whereas Vernonia lasiopus (in Kilimanjaro and Tanga) was widely used for infertility, lactation, and ease of childbirth. Vernonia usambarensis (Kilimanjaro) was linked specifically to excessive menstrual bleeding. Zaleya pentandra (in Mara) was used to shorten labor, treat dysmenorrhea, and induce abortion (Supplementary Table S1).
Pharmacological evidence of some recorded medicinal plants
3.7
Of the 330 plant species identified, only 23 medicinal plants have scientific evidence to validate their application in treating fertility issues, pregnancies, labor induction, menstrual problems, and uterine prolapse. The evidence ranges from in vitro (three plant species), in vivo (21), and clinical trials (six). Based on the results, R. communis has in vitro, in vivo, and clinical trials data to support its use as a contraceptive by blocking ovulation, hence preventing nidation from occurring. M. oleifera, Z. officinale, and Phyllanthus sp. have in vivo and clinical data, whereas P. nigrum has only clinical data, and the remaining plant species have either in vivo or in vitro data or both to validate their uses. M. oleifera has anti-anemic effects in pregnant women, reduces the incidence of stunted growth, and can act as a galactagogue. Clinical trials and in vivo studies of P. guava revealed that the plant can treat dysmenorrhea by reducing pain intensity, whereas the leaves of F. exasperata alleviate dysmenorrhea by inhibiting oxytocin-induced uterine contractions in rats. In addition, the in vivo and in vitro studies showed that the following medicinal plants induce abortion: D. cinerea, Aloe sp., R. communis, A. indica, V. amygdalina, B. pilosa, C. africana, O. suave, M. esculenta, O. corymbosa, Canthium sp., and Z. officinale. Meanwhile, C. cajan and C. abbreviata have no abortifacient activity in pregnant rats. In vivo experiments on two species of genus Phyllanthus (P. muellerianus and P. amarus) improved fertility in women by inducing ovulation, restoring the estrous cycle, and treating polycystic ovary syndrome (Table 2).
Toxicological aspects of the mentioned medicinal plants
3.8
Only 74 out of 330 plant species have been studied for toxicity. An acute toxicity study was performed for the majority of the plant species (54), followed by a sub-acute study (18), whereas sub-chronic and chronic studies were conducted for 16 and five plant species, respectively. The results revealed that 38 plant species had no toxic effects based on in vivo and in vitro studies. However, 14 plants showed signs of toxicity, including anemia, inappetence, locomotor disturbances, paresis, renal hemorrhage, decrease in body weight, and inflammation in a dose- and time-dependent manner. These plants include C. tomentosa, S. persica, P. pinnata, O. insignis, P. nigrescens, C. abbreviata, B. micrantha, E. hirta, J. curcas, O. suave, M. obtusifolia, and A. indica (Adu-Amoah et al., 2014; Anywar et al., 2022; Moshi et al., 2010; Nchu et al., 2011; Rajabalian et al., 2009). Additionally, four plant species showed mortality, including Chenopodium and J. curcas (Awasthy et al., 2010; Ez-Zriouli et al., 2023). Based on these results, it should be noted that the majority of medicinal plants used locally (77%) lack scientific evidence proving their safety for human use (Table 3).
Discussion
4
The review shows that women in Tanzania rely on a wide variety of plants for maternal care. These findings highlight both the country’s rich biodiversity and the central role that traditional medicine plays in reproductive health. However, the concentration of plant species in only a subset of regions suggests that significant knowledge remains undocumented, emphasizing the importance of continued ethnobotanical surveys and the need for a national medicinal plant registry.
The predominance of Fabaceae, Asteraceae, and Rubiaceae as leading plant families for maternal remedies aligns with studies conducted in the Philippines, Nigeria, Cameroon, and Ethiopia, where these families also dominated pregnancy-related uses (Asmare et al., 2018; Magtalas et al., 2023; Ogunlakina and Sonibare, 2020; Tsobou et al., 2016). The predominance of Fabaceae and Asteraceae in maternal conditions and contraception was also reported in another study in Uganda (Adia et al., 2025). The observed similarities in diverse ecological zones indicate that these plant families are both extensively distributed and culturally accepted.
Preparation methods were largely based on decoctions, which is likely due to their simplicity and low cost. Furthermore, oral administration was the overwhelmingly preferred route. These preparations and administration patterns were also documented in other African and Asian countries (Adamolekun et al., 2023; Ahmed et al., 2018; Asmare et al., 2018; Magtalas et al., 2023; Mashile et al., 2019). Roots were the most harvested plant part, which raises concerns about ecological sustainability and the potential threat of overexploitation. This calls for complementary strategies, such as cultivating medicinal species or promoting the use of aerial parts where possible (Ahmed et al., 2018; Asmare et al., 2018; Magtalas et al., 2023).
The most frequently mentioned medicinal plants used for labor induction or abortion were C. febrifuga, Aloe sp., R. communis, A. indica, and F. thonningii. These frequently mentioned plants are more specific in their use and, therefore, could be given higher priority for pharmacological studies. Consistent with the present study, a systematic and scoping review conducted in an African context reported that R. communis and Aloe were used to aid labor (Adamolekun et al., 2023; Ahmed et al., 2018; El Hajj and Holst, 2020). R. communis was mentioned to be used as a contraceptive. In addition, Tanzanian women used C. cajan and A. senegalensis for pregnancy-related disorders such as abdominal pain, fever, and nausea. A review from Ethiopia reported that Aloe is used to retain the placenta and to treat breast infections (Asmare et al., 2018). The variation in reported uses of these plants may be due to their locations, variation in chemical composition, historical context, cultural practices, and traditional knowledge.
our review demonstrates that Tanzanian traditional knowledge systems harbor a substantial yet uneven repertoire of medicinal plants used to manage maternal health conditions. While the high diversity of species associated with infertility, menstrual disorders, and peri-partum care underscores the cultural centrality of reproductive health, it also exposes critical gaps in mechanistic understanding, pharmacological validation, and safety profiling. The limited number of species reported for conditions such as miscarriage, postpartum complications, and contraception further highlights areas where ethnomedical knowledge may be fragmented, restricted, or undergoing erosion.
Addressing these disparities requires a shift from descriptive ethnobotany to an integrated, evidence-driven research agenda. Priority should be given to botanical authentication, phytochemical characterization, toxicological assessment, and mechanistic studies capable of linking traditional indications to biological pathways. Equally important is the need for culturally grounded qualitative research to elucidate knowledge transmission patterns, healer specialization, and sociocultural constraints surrounding sensitive reproductive conditions.
Among plants with toxicological data, the majority have only preliminary safety evaluations, which are typically limited to acute and sub-acute toxicity assays. These studies are relevant as they provide foundational data on short-term tolerability, identify early organ-specific toxicities, and inform safe starting doses for more advanced investigations, in line with OECD and WHO guidelines (EMA, 2018). However, reliance on these assays alone presents substantial limitations: they do not capture long-term, cumulative, reproductive, genotoxic, or carcinogenic risks, nor do they assess herb–drug interactions, which are critical in populations with high polypharmacy (Shaw et al., 2012). Consequently, although acute and sub-acute assays are necessary preliminary steps, they provide an incomplete toxicological profile, underscoring the need for comprehensive sub-chronic, chronic, and mechanistic studies before the broad therapeutic or commercial use of herbal products.Pharmacological evidence highlights the effects of the reported medicinal plants on reproductive physiology, underscoring the need for contextualized and dose-specific interpretations. Medicinal plant species, including Abrus precatorius, Ricinus communis, and Azadirachta indica, demonstrate robust antifertility, anti-implantation, and uterotonic activities, thus supporting traditional claims but also raising safety concerns for women of reproductive age. At the same time, plants such as Phyllanthus muellerianus, Psidium guajava, and Ficus exasperata exhibit fertility-supportive or anti-dysmenorrheic properties, suggesting therapeutic value when appropriately applied.
The consistent galactagogue effects of Moringa oleifera, Zingiber officinale, and Piper nigrum, validated in clinical and experimental models, underscore their potential integration into maternal health interventions. Additionally, the hematopoietic benefits observed for Moringa oleifera and Hibiscus sabdariffa further support their utility in managing anemia, which is a critical public health challenge in Tanzania and many low-resource settings. Importantly, plants traditionally regarded as abortifacients, such as Cassia abbreviata, Cajanus cajan, and Aloe species, showed no such activity, revealing the limitations of unverified ethnomedical assumptions. Overall, these findings emphasize the dual need to harness the promising therapeutic properties of these plants while strengthening the regulatory, toxicological, and clinical frameworks to ensure the safe use of reproductive-active botanicals.
By identifying both the richness and the limitations of current traditional practices, in this work, we provide a foundation for strategic prioritization of species with the highest potential for therapeutic advancement. Plant species with high FL/RFC values, such as Azadirachta indica and Ricinus communis, could be prioritized for preclinical and clinical studies. Bridging ethnomedical knowledge with modern biomedical science is essential not only for developing safe, effective, and contextually appropriate maternal healthcare interventions but also for safeguarding cultural heritage and informing national and regional health policy. These findings underscore the urgent need for interdisciplinary collaboration to translate traditional botanical resources into validated, scalable, and equitable solutions for maternal health. However, this review did not include studies from all administrative regions in Tanzania and considered only articles published in Kiswahili or English, which could have understated the actual number of plant species used by local Tanzanian communities for maternal conditions. Thus, the results should be interpreted in light of these limitations.
Conclusion
5
Tanzanian women utilize a wide range of medicinal plants to manage maternal conditions, yet only a small proportion of these plants have been scientifically validated or have safety data. Further pharmacological and toxicological studies are needed to verify their efficacy and ensure maternal safety. Healthcare providers should remain aware of the potential of concurrent herbal use during clinical encounters to ensure optimal patient care. Finally, conservation strategies could be strengthened for the identified root-harvested plant species.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdallah R. K. Hamza K. F. S. Mwamakimbullah R. J. L. (2007). Use of medicinal plants for maternal care in villages around Zaraninge forest reserve in Bagamoyo, Tanzania. J. Tanzan. Assoc. For. 11, 180–191.
- 2Abdu-Aguye I. Sannusi A. Alafiya-Tayo R. A. Bhusnurmath S. R. (1986). Acute toxicity studies with Jatropha curcas L. Hum. Toxicol. 5, 269–274. 10.1177/096032718600500409 3488257 · doi ↗ · pubmed ↗
- 3Abere T. A. Okoto P. E. Agoreyo F. O. (2010). Antidiarrhoea and toxicological evaluation of the leaf extract of Dissotis rotundifolia Triana (Melastomataceae). BMC Complement. Alternative Med. 10, 71. 10.1186/1472-6882-10-71 21083876 PMC 2994789 · doi ↗ · pubmed ↗
- 4Adamolekun M. M. Akpor O. A. Olorunfemi O. Akpor O. B. (2023). Traditional medicine use during pregnancy and labor in African context: a scoping review. J. Integr. Nurs. 5, 66–72. 10.4103/jin.jin_56_22 · doi ↗
- 5Adamu M. Naidoo V. Eloff J. N. (2013). Efficacy and toxicity of thirteen plant leaf acetone extracts used in ethnoveterinary medicine in South Africa on egg hatching and larval development of Haemonchus contortus . BMC Vet. Res. 9, 38. 10.1186/1746-6148-9-38 23442744 PMC 3599279 · doi ↗ · pubmed ↗
- 6Adedapo A. A. Omoloye O. A. Ohore O. G. (2007). Studies on the toxicity of an aqueous extract of the leaves of Abrus precatorius in rats. Onderstepoort J. Vet. Res. 74, 31–36. 10.4102/ojvr.v 74i 1.137 17708151 · doi ↗ · pubmed ↗
- 7Adeyemo-Salami O. A. Makinde J. M. (2013). Acute and sub-acute toxicity studies of the methanol extract of the leaves of Paullinia pinnata (Linn.) in Wistar albino mice and rats. Afr. J. Med. Med. Sci. 42, 81–90. 23909098 · pubmed ↗
- 8Adia M. M. Savina A. Jane N. Joel M. Godwin A. Esezah K. K. (2025). Medicinal plant species used for contraception and reproductive health care in rural Uganda. Heliyon 11, 1–23. 10.1016/j.heliyon.2024.e 41518 39844971 PMC 11750540 · doi ↗ · pubmed ↗