High adherence to angiotensin-converting enzyme inhibitor in children and adolescents with Alport syndrome: objective verification using liquid chromatography-mass spectrometry
Jan Boeckhaus, Burkhard Tönshoff, Lutz T. Weber, Dieter Haffner, Lars Pape, Kay Latta, Henry Fehrenbach, Baerbel Lange-Sperandio, Matthias Kettwig, Sabine König, Ulrike John-Kroegel, Jutta Gellermann, Matthias Galiano, Angelika Hafke, Frank Streit, Oliver Gross

TL;DR
This study used a precise method to confirm that children with Alport syndrome consistently took their prescribed kidney disease medication.
Contribution
A novel LCMS-based method was developed and validated to objectively verify ACEi adherence in pediatric Alport syndrome patients.
Findings
High adherence to ACEi was confirmed in 96% and 95% of children at two separate measurements.
The LCMS method accurately detected drug intake without prior notification to participants.
All negative control samples were correctly identified, validating the method's reliability.
Abstract
Kidney failure (KF) in children and adolescents leads to reduced lifespan and compromised health. Alport syndrome (AS) is a leading hereditary cause of KF in children. Angiotensin-converting enzyme inhibitors (ACEi) have demonstrated efficacy in delaying KF in young people living with AS, but non-adherence can compromise their therapeutic benefits. To investigate the adherence to ACEi in children and adolescents with AS, a liquid chromatography-mass spectrometry (LCMS)-based method was developed for objective verification of recent medication intake at two different time points in this cohort study. Urine samples from 58 children enrolled in the EARLY PRO-TECT Alport trial were analyzed. An LCMS-based method was established and validated to simultaneously screen and quantify both ramipril and ramiprilat in urine samples. Participants were not informed in advance of the medication…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
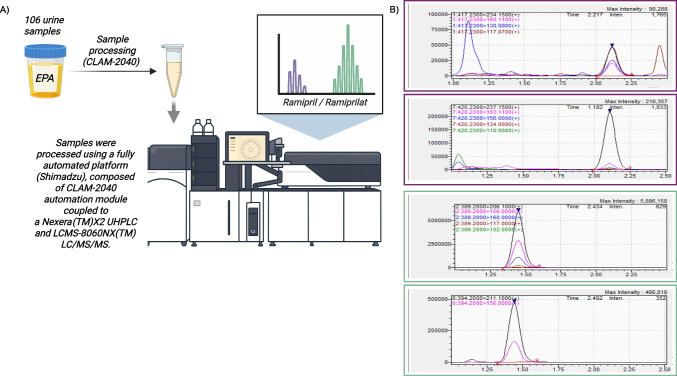 Figure 1
Figure 1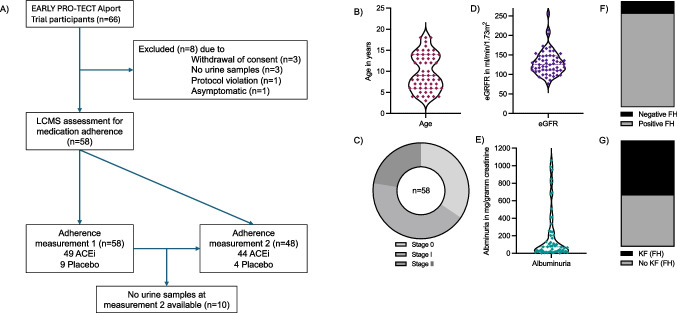 Figure 2
Figure 2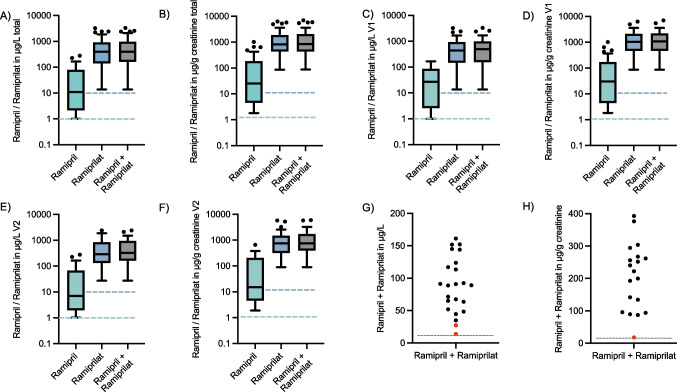 Figure 3
Figure 3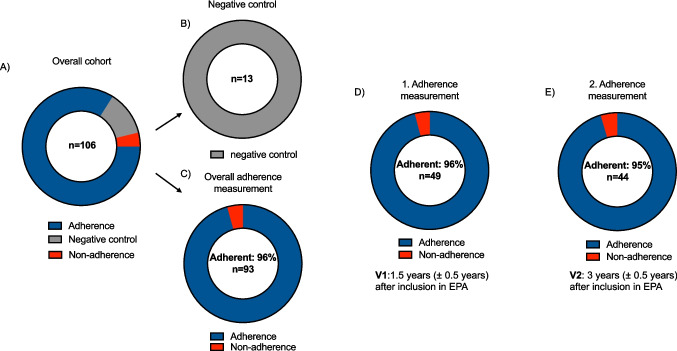 Figure 4
Figure 4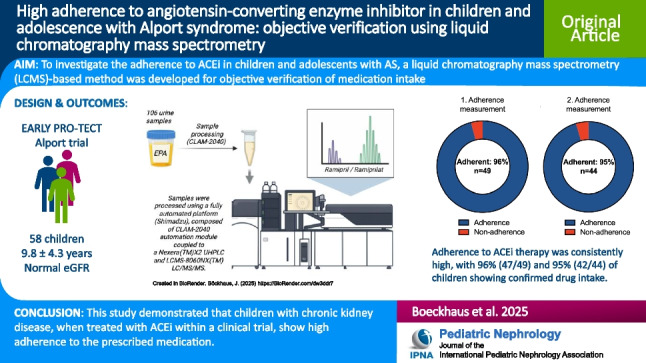 Figure 5
Figure 5- —http://dx.doi.org/10.13039/501100002347Bundesministerium für Bildung und Forschung
- —German Alport Patient Group
- —Herzzentrum Göttingen (1018)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplement system in diseases · Cell Adhesion Molecules Research · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Background
Kidney failure (KF) leads to reduced lifespan in children and adolescents [1, 2]. Alport syndrome (AS) is a leading hereditary cause of KF in children [3–5]. In most registries, CAKUT is the most common pediatric cause of kidney failure, and the relative frequency of Alport syndrome varies by region. AS is caused by a defect in type IV collagen, which is an essential component of the basement membrane in the kidney, eyes, and cochlea [6, 7]. The disruption of type IV collagen structure results in impaired function of the glomerular basement membrane filtration barrier, leading to hematuria, increased albuminuria, and, consequently, a high risk for progression to KF [8]. The disease often manifests further with progressive sensorineural hearing loss and ocular lesions [9–11]. The predominant mode of inheritance for AS is X-linked, attributed to pathogenic variants within the COL4A5 gene. Autosomal recessive or dominant inheritance patterns, affecting the COL4A3 or COL4A4 genes, account for up to 30% [12–15]. Furthermore, digenic inheritance has been reported [16, 17]. Renin-angiotensin system inhibition (RASi) with angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs) has demonstrated efficacy in delaying KF in patients with AS [18–20]. Ramipril, an ACEi, was investigated in the randomized placebo-controlled EARLY PRO-TECT Alport trial (NCT01485978) and showed a trend towards slowed disease progression with early treatment, without safety concerns compared to placebo [21]. Despite the established benefits of RASi, achieving optimal therapeutic outcomes hinges on patient adherence to prescribed medication [22]. Medication non-adherence has a negative impact on outcomes for children with chronic illnesses, including those with chronic kidney disease (CKD) or KF [23–26]. Due to the long-term requirement for medication intake, the treatment of asymptomatic disease in early CKD, and the often complex treatment regimens in advanced CKD, adherence in pediatric CKD is particularly challenging [27]. Consequently, non-adherence can be a significant obstacle to effective treatment in this vulnerable population, potentially compromising the therapeutic benefits of prescribed treatments [28]. Recognizing the limitations of adherence measures such as self-reporting, a liquid chromatography-mass spectrometry-based method was used to provide objective verification of medication intake [29]. Considering the positive family history often present in patients with AS, and the demonstrated safety of ramipril, we hypothesized that the medication intake at two time points representing adherence to medication in this population would surpass rates previously reported in the literature [21, 30]. To investigate this, we analyzed urine samples collected from children enrolled in the EARLY PRO-TECT Alport trial.
Methods
Clinical data and sampling of urine
The participant cohort was previously described as part of the EARLY PRO-TECT Alport trial, a randomized, placebo-controlled, double-blind study with an open-label control arm (ClinicalTrials.gov: NCT01485978) [21, 30–34]. Children aged 2 to 18 years with confirmed AS and normal glomerular filtration rates were enrolled. The treatment period lasted 3 to 6 years. Disease progression was defined as doubling or tripling of albuminuria [21]. The study was conducted in accordance with the Declaration of Helsinki (1964, and its later amendments) and approved by the ethics committees of the University Medical Center Göttingen (AZ 11/06/11) and all participating centers. Written informed consent, including the use of collected biosamples for research purposes, was obtained from all legal guardians, and assent from participants aged 6 and older. From the initial cohort of 66 children in the EARLY PRO-TECT Alport trial, eight participants were not included in this study due to withdrawal of consent (n = 3), unavailability of urine samples (n = 3), protocol violation (n = 1), or being asymptomatic (n = 1). For this study, urine samples were selected at two time points: V1, 1.5 years (± 0.5 years) and, if available, V2, 3 years (± 0.5 years) after inclusion in the trial to assess medication adherence.
Intervention and outcome measures
Stages of AS were defined as stage 0, albuminuria < 30 mg/g creatinine; stage I, albuminuria 30–300 mg albumin/g creatinine; and stage II, albuminuria > 300 mg/g creatinine [35]. The baseline for this study was defined as the first adherence measurement. Participants were not informed in advance of the adherence measurements. Analysis also included samples from the placebo arm (negative controls). The investigator responsible for the analysis of the samples was not informed a priori of the inclusion of negative controls. In this study, adherence was defined as objective evidence of recent medication intake at the time of each study visit, confirmed by the presence of ramipril/ramiprilat in the urine sample. The lower limit of quantification (LLOQ) was 1 µg/L for ramipril and 10 µg/L for ramiprilat [36, 37]. Therefore, samples where the sum of ramipril and ramiprilat was less than 10 µg/L were defined as non-adherent. Additionally, in samples with concentrations above the LLOQ, the blinded investigator responsible for conducting the sample measurements assessed samples as adherent or non-adherent in patients with two measurements, based on baseline values and the trend of the ramipril to ramiprilat ratio. In a second step, to normalize for urine dilution effects, concentrations of ramipril and ramiprilat were normalized to urinary creatinine concentration. The creatinine-normalized LLOQ was calculated using the mean creatinine concentration of this sample cohort (1.8 µg/g creatinine for ramipril and 18 µg/g creatinine for ramiprilat).
Quantitative analysis of ramipril and ramiprilat
Ramipril and ramiprilat in urine were quantified using an automated liquid chromatography-mass spectrometry (LCMS) method (Fig. 1). Calibration standards and quality control samples were prepared using commercially sourced standards. Samples were automatically processed using a CLAM-2040 system (Shimadzu Corporation, Duisburg, Germany) coupled to a Nexera LCMS-8060NX (Shimadzu Corporation, Duisburg, Germany), including protein precipitation and filtration. The chromatographic system consisted of two Shimadzu LC-30AD pumps (NexeraX2), a CTO40AC oven and a SIL-40AC autosampler (Shimadzu Corporation, Duisburg, Germany). Chromatographic separation was achieved using a C18 column with a gradient mobile phase of water and methanol containing acetic acid and ammonium acetate. Mass spectrometric detection was performed using a LCMS-8050 triple quadrupole mass spectrometer (Shimadzu Corporation, Duisburg, Germany) with positive electrospray ionization. Scheduled multiple reaction monitoring (MRM) was utilized for quantification. The method demonstrated linearity across the calibration range and acceptable within- and between-run imprecision.Fig. 1. Quantitative analysis of ramipril and ramiprilat in urine using automated liquid chromatography-mass spectrometry. A Schematic representation of the analytical workflow (Created in BioRender. Böckhaus, J. (2025) https://BioRender.com/dw3ddr7); B representative chromatogram of a urine sample showing low ramipril and high ramiprilat concentrations
Lower limits of quantification were established for both ramipril and ramiprilat. Calibration stability was proven over a period of 8 days. A detailed description of the reagents, sample preparation, and LCMS parameters is provided in the supplementary material.
Statistical methods
Statistical comparisons were not formally powered or prespecified. Continuous variables were presented as mean and standard deviation (SD) or as median and interquartile range (IQR), categorical variables as percentages. For roughly normally distributed values, group means were compared using an unpaired Student’s t-test. Binomial 95% confidence intervals (CIs) were calculated using the Clopper-Pearson exact method. Per-patient concordance metrics were determined using a 2 × 2 contingency table for patients with paired samples. Data analysis was performed using IBM SPSS Statistics (version 30 for MacOS, IBM Corporation, Armonk, NY, USA). GraphPad Prism (version 10 for macOS, GraphPad Software, San Diego, California, USA) and Biorender (Toronto, Ontario, Canada) were used to generate figures.
Results
Demographics and clinical characteristics
Figure 2 presents a sampling schema and clinical and demographic characteristics of the 58 children included in this study. Of these, 57 were male (98%). The mean age at baseline was 9.8 ± 4.3 years. The mode of inheritance was X-linked in 47 children (81%), autosomal recessive in 9 children (16%), and unknown in 2 children (3%). Twenty children were in AS stage 0 (34%), 25 in AS stage I (43%), and 13 in AS stage II (22%). The mean estimated glomerular filtration rate (eGFR) was 130 ± 32 mL/min/1.73 m^2^, with a median albuminuria of 73 mg/gram creatinine (interquartile range [IQR] 20–250; n = 57). At first adherence measurement, 49 children were treated with RASi (84%), with 39 participants in the open-label control arm having already received RASi treatment before inclusion in the trial. The mean duration of RASi treatment at first adherence measurement was 36 ± 29 months, with a maximum duration of 121 months. A positive family history was reported in 88% of the children, with 48% having a family member with KF (Table 1).Fig. 2. Sampling schema and clinical and demographic characteristics. A Sampling schema. ACEi, angiotensin-converting enzyme inhibitor; LCMS, liquid chromatography-mass spectrometry. B Age in years (n = 58); C stages of Alport syndrome (AS) at baseline (n=58); D estimated glomerular filtration (eGFR) in mL/min/1.73 m^2^ (n = 58); E albuminuria in mg/gram creatinine (n = 57, two extreme values were not displayed; 2544; 4603 mg/g creatinine); F positive and negative family history (FH) for AS (n = 58); G positive and negative family history for kidney failure (KF) (n = 58)Table 1. Demographic and clinical characteristics at measurement of adherenceNumberMale no. (%)5857 (98)Age (years)589.8 ± 4.3Mode of inheritance (%)58 X-linked47 (81) Autosomal recessive9 (16) Unknown2 (3)AS stage (%)58 020 (34) I25 (43) II13 (22)eGFR58130 ± 32 (mL/min/1.73 m^2^)Albuminuria5773 (20–250) (mg/g creatinine)RASi5849 (84)RASi inhibitors of the renin-angiotensin system. AS stage 0, albuminuria < 30 mg/g creatinine, AS stage I albuminuria 30–300 mg/g creatinine, AS stage II, albuminuria > 300 mg/g creatinine. Values are mean + SD, median (IQR), or n (%) as appropriate
Adherence measurement
A total of 106 urine samples were analyzed at two different time points. In urine samples where concentrations were above the LLOQ, the mean ramipril concentration was 46.1 ± 63.1 µg/L (n = 70), and the mean ramiprilat concentration was 609.9 ± 623.6 µg/L (n = 91) (Table 2; Supplementary Table 1). Table 2. Urine ramipril and ramiprilat concentrationsAnalyteOverallFirst adherence measurement (V1)Second adherence measurement (V2)Ramipril (µg/L)46.1 ± 63.1 (70)46.7 ± 53.6 (36)45.5 ± 72.6 (34)Ramiprilat (µg/L)609.9 ± 623.6 (91)678.3 ± 686.7 (48)533.6 ± 542.5 (43)Sum (ramipril + ramiprilat) (µg/L)645.5 ± 648.7 (91)713.5 ± 709.7 (48)569.7 ± 571.9 (43)The sum of ramipril and its active metabolite, ramiprilat, is used to provide a comprehensive measure of medication intake. Ramipril, an inactive prodrug, is converted into its active form, ramiprilat. By combining the levels of both compounds, the measurement accounts for individual metabolic differences, offering a more robust indicator of medication adherence. Concentrations below the LLOQ were excluded from this analysis. Numbers in parentheses represent the number of samples above the LLOQ used in the analysis
At first adherence measurement, nine children (16%) were not treated with ACEi (negative control). All nine negative control samples (100%) were correctly identified. Of the 49 children receiving ACEi, adherence measurement confirmed recent medication intake in 47 (96%; 95% CI, 86% to 99.5%), while two samples were classified as non-adherent: one due to both ramipril and ramiprilat concentrations being below the LLOQ, and the other because the sum of ramipril and ramiprilat was only marginally above the LLOQ (Fig. 3). These urine samples were from two brothers with X-linked AS in the open-label study arm: a 14-year-old boy (AS stage I) on RASi for 8 years who progressed 1 year after the adherence measurement, and a 13-year-old boy (AS stage II) on treatment with RASi for 10 years who progressed 6 months after entering the EARLY PRO-TECT Alport trial.Fig. 3A–F Tukey plots showing the distribution of all samples with drug levels above the lower limit of quantification (LLOQ). Distribution of all samples in A µg/L (n = 91) and B µg/g creatinine (n = 84). Distribution of samples from visit 1 in C µg/L (n = 48) and D µg/g creatinine (n = 44). Distribution of samples from visit 2 in E µg/L (n = 43) and F µg/g creatinine (n = 40). Dotted lines indicate the LLOQ for ramipril (green) and ramiprilat (blue). Scatter plots of samples with lower ramipril and ramiprilat concentrations in G µg/L (n = 23) and H µg/g creatinine (n = 19), data points shown in red were classified as non-adherent
At first measurement, adherence was observed in 18 of 20 participants (90%; 95% CI 68.3% to 98.8%) with disease progression and in 29 of 29 participants (100%; 95% CI 88.1% to 100%) without disease progression during the trial. Forty of 42 (95%; 95% CI 84% to 99.4%) with a positive family history demonstrated adherence, compared to 7 of 7 (100%; 95% CI 59.2% to 100%) with a negative family history. Specifically, adherence was confirmed in 21 of 23 participants (91%; 95% CI 72% to 98.9%) with family members affected by KF and in 26 of 26 participants (100%; 95% CI 86.5% to 100%) without family members affected by KF. Furthermore, 37 of 39 pretreated participants (95%; 95% CI 82.9% to 99.4%) showed adherence, while 10 of 10 participants (100%; 95% CI 69.1% to 100%) who started ACEi at inclusion into the clinical trial adhered.
In those with available urine samples, a second adherence assessment 1 to 2 years after the first measurement was carried out (n = 48). At the second adherence measurement, 44 of the 48 children were receiving ACEi (92%). All four negative controls were correctly identified. Adherence measurement was positive in 42 of 44 children (95%; 95% CI 84.5% to 99.4%) (Fig. 4). Of the non-adherent samples, one exhibited ramipril and ramiprilat concentrations below the LLOQ. The other was classified as non-adherent because concentrations of both analytes were significantly lower compared to the initial adherence measurement. These negative adherence measurements were observed in two boys in AS stage 0 (ages 4 and 6) in the open-label arm. Both had a positive family history, including a family member with KF. Notably, in both children, the initial adherence measurement was positive, and both exhibited no disease progression during the study. In three children, who were switched from placebo (first measurement, negative controls) to ramipril due to disease progression, the second measurement confirmed the intake of ramipril in all three children. In patients with urine measurements above the LLOQ at both time points, the aggregation of ramipril and ramiprilat did not differ significantly (732.7 ± 622.2 µg/L at the first measurement and 583.6 ± 584.4 µg/L at the second measurement; n = 40; p = 0.27). Per-patient adherence concordance was assessed among 41 children with urine measurements at both time points. The overall percent agreement between the initial and second adherence measurement was 95.1% (39/41 patients). Specifically, 39 of 41 (95.1%) patients were consistently classified as adherent, and zero (0/41) patients were consistently classified as non-adherent.Fig. 4. Illustration of medication adherence. Donut graphs show the proportion of A the overall cohort of 106 measurements, including 13 negative controls; B correctly identified negative controls (n = 13, 100%); C adherence and non-adherence at both time points of the study (n = 93; 96% adherence); D adherence and non-adherence at first adherence measurement (n = 49; 96% adherence); E adherence and non-adherence at the second adherence measurement (n = 44; 95% adherence). V1, visit 1; V2, visit 2; EPA, EARLY PRO-TECT Alport trial
To investigate the robustness of the analysis against potential urine dilution effects, concentrations of ramipril and ramiprilat were normalized to urinary creatinine concentration using the mean urinary creatinine concentration of this cohort (55.6 mg/dL; n = 98). In urine samples where concentrations were above the LLOQ, the mean ramipril concentration was 123 ± 195.4 µg/g creatinine (n = 61), and the mean ramiprilat concentration was 1493.2 ± 2140.4 µg/g creatinine (n = 84). The classification of all samples remained consistent with the initial analysis using micrograms per liter. The three samples available from patients classified as non-adherent using micrograms per liter were again classified as non-adherent, as two of the samples were below the LLOQ and the second measurement in the third patient was significantly lower compared to the first measurement.
Discussion
This study examined adherence to the ACEi ramipril in children included in the double-blinded placebo-controlled EARLY PRO-TECT Alport trial at two time points. Using an automated liquid chromatography-mass spectrometry as an objective tool for the determination of ramipril in urine, an adherence rate of 96% and 95% was demonstrated at two distinct time points of the trial. In the literature, self-reported adherence in children with CKD ranges from 74% to 96% [28, 38, 39] Objective measures of medication adherence typically reveal lower rates compared to self-reported adherence, with discrepancies reaching up to 69% [40–42].
The high adherence rates observed in our study may be attributed to several factors: Firstly, the simplified dosing regimen, involving once-daily medication intake, likely facilitated participants’ adherence. Secondly, the frequent presence of a positive family history, providing participants with firsthand insight into the disease, may have enhanced their motivation to adhere to the prescribed therapy. Thirdly, the comprehensive education provided about the therapy’s benefits and potential risks within the clinical trial setting likely enhanced participants’ and their families’ understanding of the study medication [28, 43].
In a clinical setting, the LCMS method can provide objective verification of medication intake, serving as a valuable complement to standard clinical monitoring, such as the measurement of albuminuria. While more expensive, the test’s cost can be justified in specific clinical scenarios where a patient’s adherence is unclear and precise information is needed to guide management.
Furthermore, this study might offer additional insights into ACEi therapy in children with CKD. Notably, despite ACEi therapy at the maximum tolerated dose (up to 6 mg/m^2^), no significant blood pressure reduction was observed in the EARLY PRO-TECT Alport trial [21]. Given this study’s high confirmation of medication intake, non-adherence is an unlikely explanation for this lack of blood pressure reduction. This observation is consistent with prior findings suggesting that an increase in RAS blockade has not consistently been shown to lead to a further drop in blood pressure, which indicates that the nephroprotective effects of ACEi are, at least partially, mediated by mechanisms independent of blood pressure lowering [44–46]. In addition, the high medication intake rate observed in this study, along with the EARLY PRO-TECT Alport trial’s established favorable safety profile of ACEi in pediatric CKD, might be interpreted as an indicator of the therapy’s good tolerability [21].
Strengths of this study include the implementation of adherence measurements after the EARLY PRO-TECT Alport trial, thereby ruling out adherence measurement bias by ensuring participants were not prospectively aware of upcoming controls. The blinding of the scientist who analyzed the samples enhanced the objectivity of the measurements. Furthermore, the reliability of the measurement method was demonstrated by the correct identification of all 13 negative controls.
Additionally, the use of data from a randomized controlled trial enables the description of a clinically well-characterized cohort (including family history and well-monitored disease progression). The use of creatinine-normalized concentrations as a sensitivity analysis indicated that potential urine dilution effects did not confound the classification of patient adherence, as all samples retained their original classification.
As a limitation of this study, samples were not available from all children in the EARLY PRO-TECT Alport trial, resulting in a further reduction of the already limited cohort size. Additionally, the high adherence to medication in this study made it impossible to analyze specific risk factors for non-adherence. Furthermore, the study analyzed samples from primarily boys, limiting the generalizability of the findings to female participants. A further study limitation is the lack of information on participants’ ramipril dosing times (morning or evening), which could have influenced ramipril and ramiprilat concentrations and their interpretation. As a result, a detailed analysis correlating specific dose timing with drug concentration was not feasible. Crucially, this study’s adherence definition prioritizes the detection of ramipril and ramiprilat in urine for regular medication intake, aligning with common adherence definitions in the literature, rather than specific concentration levels [47–49]. Hence, it must be acknowledged that the presence of ramipril or ramiprilat in a single urine sample provides evidence of recent medication intake at a specific moment rather than a continuous measure of ongoing medication intake. In addition, it is important to point out that this study was conducted in a controlled clinical trial setting. This structured environment, with its frequent patient contact and close monitoring, likely contributed to higher adherence rates than those seen in routine practice. Consequently, the generalizability of our findings to routine clinical practice is limited.
Another limitation of this study is the absence of comparator measures (e.g., serum levels) to validate this study’s adherence findings. Future studies should explore these comparisons to better determine the sensitivity and specificity of urine-based methods for measuring adherence, especially in pediatric populations. Overall, this study demonstrated that children with CKD, included in a double-blinded, placebo-controlled clinical trial, show high adherence to the study medication. This provides a compelling rationale for the inclusion of children and adolescents with CKD in clinical trials, a population that could derive substantial benefit from innovative, effective therapies, but is often excluded from clinical trials [50].
Conclusion
This study demonstrated that children with chronic kidney disease, when treated with ACEi within a clinical trial, show high adherence to the prescribed medication.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file 1 (DOCX 35.2 KB)Graphical Abstract (PPTX 1.49 MB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burgess E, Muirhead N, de Cotret PR, Chiu A, Pichette V, Tobe S, SMART (Supra Maximal Atacand Renal Trial) Investigators (2009) Supramaximal dose of candesartan in proteinuric renal disease. J Am Soc Nephrol 20:893–900. 10.1681/ASN.200804041610.1681/ASN.2008040416 PMC 266382719211712 · doi ↗ · pubmed ↗