Sarcopenia as a predictor of cage subsidence following stand-alone oblique lumbar interbody fusion in non-osteoporotic patients
Dazhuang Miao, Xianda Gao, Weiqi Zhang, Xiaowei Ma, Di Zhang

TL;DR
This study finds that muscle loss (sarcopenia) increases the risk of cage subsidence after a specific spinal surgery in non-osteoporotic patients.
Contribution
Identifies sarcopenia as a novel predictor of cage subsidence in non-osteoporotic patients undergoing oblique lumbar interbody fusion.
Findings
Cage subsidence occurred in 32.7% of non-osteoporotic patients after SA-OLIF.
Sarcopenia, age over 59.5 years, and low bone mineral density predict cage subsidence.
Patients with sarcopenia had nearly four times higher odds of cage subsidence.
Abstract
This study aimed to identify predictors of cage subsidence following stand-alone oblique interbody fusion (SA-OLIF) in non-osteoporotic patients. A retrospective analysis was performed on 98 patients who underwent SA-OLIF. Cage subsidence was defined to have occured when a cage was subsided into the adjacent endplate by more than 2 mm on the last follow up radiographs. Patients were categorized into subsidence and non-subsidence groups accordingly. Patient characteristics, radiographic parameters, and clinical outcomes were recorded. Sarcopenia was assessed using the L3 skeletal muscle index on axial computed tomography images. Multivariate logistic regression analysis was conducted to identify the predictors of cage subsidence following SA-OLIF. Of the 98 patients who underwent SA-OLIF, subsidence occurred in 32 (32.7%). The subsidence group had a higher mean age (P = 0.005) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
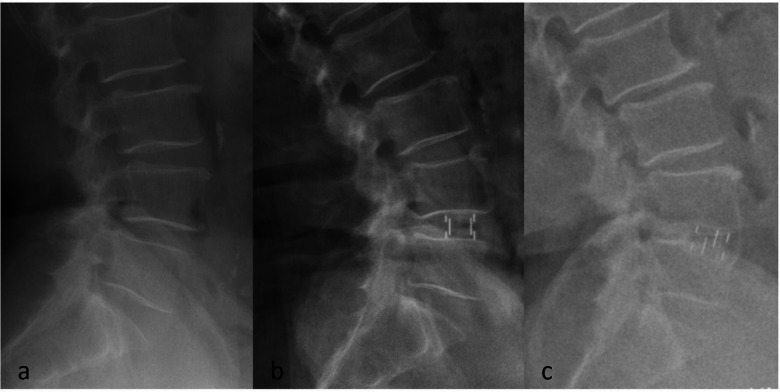 Figure 1
Figure 1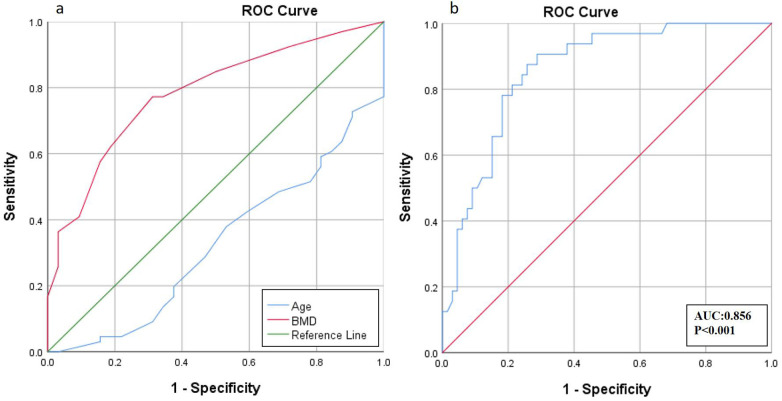 Figure 2
Figure 2| Variable | Subsidence group ( | Non-subsidence group ( |
| |
|---|---|---|---|---|
| Age (years) | 63.28 ± 5.87 | 58.52 ± 7.50 | 2.822 | 0.005 |
| Gender | ||||
| Male | 7 | 10 | 0.679 | 0.410 |
| Female | 25 | 56 | ||
| Body mass index | 23.93 ± 2.54 | 24.72 ± 3.06 | 1.649 | 0.102 |
| BMD ( | −2.05 ± 0.31 | −1.61 ± 0.43 | 4.548 | <0.001 |
| Smoking | 5 | 7 | 0.146 | 0.702 |
| History of symptoms (months) | 11.81 ± 6.95 | 12.62 ± 9.57 | 0.186 | 0.853 |
| Followed up period (months) | 26.69 ± 4.75 | 26.24 ± 4.65 | 0.656 | 0.512 |
| L3-SMI (cm2/m2) | 38.64 ± 6.83 | 43.71 ± 8.35 | 3.189 | 0.001 |
| Sarcopenia | 15 | 12 | 8.889 | 0.003 |
| Surgical segment | ||||
| L2/3 | 3 | 2 | 3.120 | 0.187 |
| L3/4 | 9 | 13 | ||
| L4/5 | 20 | 51 | ||
| Fusion rate% | 90.6% (29/32) | 93.9% (62/66) | 0.032 | 0.858 |
| Revision rate% | 0 | 0 | ||
| Variable | Subsidence group ( | Non-subsidence group ( |
| |
|---|---|---|---|---|
| Intervertebral height (mm) | ||||
| Preoperative | 8.84 ± 1.66 | 9.01 ± 1.73 | 0.468 | 0.641 |
| Postoperative | 12.26 ± 1.25 | 11.71 ± 1.65 | 1.568 | 0.117 |
| Last follow-up | 9.44 ± 1.53 | 10.80 ± 1.63 | 3.913 | <0.001 |
| ΔIH | 2.82 ± 0.71 | 0.91 ± 0.60 | 8.000 | <0.001 |
| Lumbar lordosis | ||||
| Preoperative | 29.66 ± 9.01 | 32.02 ± 11.17 | 1.041 | 0.300 |
| Last follow-up | 35.56 ± 10.24 | 39.20 ± 10.52 | 1.645 | 0.100 |
| Local lordosis Cobb angle | ||||
| Preoperative | 15.13 ± 3.11 | 15.86 ± 4.27 | 1.512 | 0.130 |
| Last follow-up | 16.31 ± 4.21 | 18.71 ± 4.67 | 2.647 | 0.008 |
| Cage height | ||||
| 8 mm | 2 | 3 | 4.284 | 0.115 |
| 10 mm | 11 | 38 | ||
| 12 mm | 18 | 25 | ||
| Cage length | ||||
| 40 mm | 2 | 6 | 3.747 | 0.157 |
| 45 mm | 19 | 49 | ||
| 50 mm | 11 | 11 | ||
| ODI scores | ||||
| Preoperative | 26.38 ± 1.15 | 24.92 ± 0.95 | 0.853 | 0.393 |
| Last follow-up | 15.28 ± 1.51 | 12.35 ± 0.64 | 1.151 | 0.250 |
| Low back pain | 7 | 6 | 2.882 | 0.112 |
| JOA scores | ||||
| Preoperative | 17.16 ± 0.49 | 17.55 ± 0.29 | 0.735 | 0.463 |
| Last follow-up | 21.81 ± 0.62 | 22.74 ± 0.39 | 1.18 | 0.238 |
| Recovery rate% | 38.68 ± 4.65% | 45.74 ± 2.97% | 1.356 | 0.175 |
| Variable | Adjusted odds radio | 95% confidence interval | |
|---|---|---|---|
| Age (years) | 1.113 | 1.025–1.208 | 0.011 |
| BMD | 0.059 | 0.014–0.256 | <0.001 |
| Sarcopenia | 3.881 | 1.231–12.241 | 0.021 |
| Variable | Sensitivity (%) | Specificity (%) | AUC | Cutoff | |
|---|---|---|---|---|---|
| Age (years) | 78.1 | 48.5 | 0.676 | 59.5 | 0.005 |
| BMD | 77.3 | 68.7 | 0.783 | −1.95 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Bone health and osteoporosis research · Cervical and Thoracic Myelopathy
Introduction
The term “sarcopenia” was first proposed by Irwin Rosenberg in 1989 and refers to the progressive loss of muscle mass, strength, and function in the elderly (1, 2). The etiology of sarcopenia is multifactorial, with reduced physical activity, inadequate nutrition, disease triggers, activation of inflammatory pathways, loss of neuromuscular junction integrity, and hormonal changes all contributing (1). Sarcopenia has been associated with adverse outcomes in several conditions, including chronic obstructive pulmonary disease (3), coronary heart disease (4), and cancer (5). Recent studies have also indicated that patients with sarcopenia are more likely to experience poor outcomes following spinal surgery (6). However, the relationship between sarcopenia and cage subsidence following stand-alone oblique lumbar interbody fusion (SA-OLIF) has not yet been investigated.
Oblique lumbar interbody fusion (OLIF), a minimally invasive surgical approach, was first proposed by Mayer in 1997 (7). SA-OLIF and OLIF with instrumentation are two surgical strategies for treating lumbar spine disorders (8–12). SA-OLIF offers several advantages, including shorter operative time, reduced intraoperative bleeding, fewer implant-related complications, lower treatment costs, and shorter hospital stays (10). Nevertheless, cage subsidence remains a common complication following SA-OLIF, making the identification of appropriate surgical indications a critical issue.
Our previous study demonstrated that the most common clinical symptom of cage subsidence was low back pain (13), which was relieved by conservative treatment in most cases. However, severe cage subsidence can induce spinal stenosis and nerve compression, necessitating revision surgery. Osteoporosis [bone mineral density (BMD) T-score < −2.5] has been established as a significant risk factor for cage subsidence, for which instrumentation is recommended (14–16). However, cage subsidence is also frequently observed in for patients with T-score higher than −2.5 following SA-OLIF. Therefore, the present study aimed to identify predictors of cage subsidence following SA-OLIF in non-osteoporotic patients, providing evidence to guide surgical planning in clinical practice.
Materials and methods
Patients
This study was approved by the Clinical Ethics Committee of the Third Affiliated Hospital of Hebei Medical University. In accordance with national legislation and institutional requirements, written informed consent was not required for participation.
A retrospective review was conducted on 98 patients who underwent SA-OLIF between January 2018 and January 2023 at the Third Hospital of Hebei Medical University, China. Inclusion criteria were as follows: (1) patients with symptomatic lumbar degenerative diseases (Grade I lumbar spondylolisthesis, lumbar instability, mild to moderate spinal stenosis, or degenerative lumbar disc disease) who had not improved after at least 3 months of conservative treatment; (2) clinical symptoms consistent with magnetic resonance imaging (MRI) and computed tomography (CT) findings; (3) single-level SA-OLIF; and (4) minimum follow-up of 2 years. Exclusion criteria were as follows: (1) previous spinal fusion surgery; (2) tumors, inflammation, trauma, or other spinal diseases; (3) osteoporosis (T-score < −2.5); (4) incomplete medical records; and (5) extremely high body mass index (BMI) or intraoperative endplate injury.
Surgical procedure
All procedures were performed by the same experienced surgical team. Under general anesthesia, patients were placed in a standard right lateral position and secured with tape. The C-arm X-ray machine was used to mark the center of the target intervertebral disc space, after which a 4-cm incision was made medial to the marked point. The skin, subcutaneous tissue, and external oblique aponeurosis were incised, and blunt dissection was performed to separate the fibers of the external oblique, internal oblique, and transversus abdominis muscles. Access to the disc space was achieved through the retroperitoneal corridor between the psoas major and the great vessel sheath, with careful identification and protection of the genitofemoral nerve, peritoneum, great vessel sheath, ureters, and any segmental vessels. Once the surgical intervertebral space was confirmed, a fixed working channel was installed. The annulus fibrosus was incised, and the nucleus pulposus and cartilaginous endplate tissues above and below the disc were carefully removed, avoiding injury to the bony endplate. A suitable polyetheretherketone cage (6 °Clydesdale; Medtronic Sofamor Danek, Memphis, Tennessee, USA) filled with allogeneic trabecular bone and demineralized bone matrix was implanted under intraoperative C-arm fluoroscopic guidance. On the third postoperative day, patients were encouraged to ambulate with waist support and to perform low back muscle exercises under professional guidance.
Sarcopenia assessment
Sarcopenia was assessed in accordance with the diagnostic criteria recommended by the European Working Group on Sarcopenia in Older People (EWGSOP) (17, 18). The L3 skeletal muscle index (L3-SMI) was measured on axial computed tomography images, although this cannot fully reflect physical performance. The L3-SMI was calculated as the skeletal muscle area at the level of the third lumbar vertebra divided by the square of the patient's height (cm^2^/m^2^). Sarcopenia was defined using an L3-SMI cutoff of 45.4 cm^2^/m^2^ for male patients and 34.4 cm^2^/m^2^ for female patients (18).
Radiological and clinical evaluation
Patients were categorized into subsidence and non-subsidence groups. Preoperative variables including age, sex, BMI, BMD, smoking status, symptom duration, operative level, and fusion rate were recorded. Dual-energy X-ray absorptiometry was used to assess BMD, with values below −2.5 defined as osteoporosis.
Radiological outcomes were evaluated using radiographs, CT, and MRI preoperatively, postoperatively, and at the last follow-up. Lumbar lordosis (LL) was measured as the Cobb angle between the superior endplate of L1 and the inferior endplate of L5. Local lordosis was defined as the Cobb angle between the superior endplate of the upper vertebra and the inferior endplate of the lower vertebra at the surgical segment. Intervertebral height (IH) was calculated as the average of the anterior, middle, and posterior heights between adjacent endplates. ΔIH was defined as the difference between postoperative and last follow-up IH; a ΔIH greater than 2 mm was diagnosed as cage subsidence (Figure 1) (19). All imaging measurements were independently performed by two spinal surgeons, with disagreements resolved by a third senior surgeon. Measurements were obtained using the DICOM-PACS program.
Preoperative (a), postoperative (b), and last follow-up (c) radiographs of SA-OLIF.
Clinical outcomes were assessed using questionnaires administered preoperatively and at the final follow-up visit. Lumbar function and pain intensity were evaluated using the Oswestry Disability Index (ODI; 0–50), with postoperative low back pain defined as a final ODI score exceeding the preoperative score. Neurological function was assessed using the Japanese Orthopaedic Association (JOA) score (0–29), and the recovery rate was calculated as follows: recovery rate (%) = (final JOA score−preoperative JOA score)/(29−preoperative JOA score) × 100%.
Statistical analysis
Data were analyzed using SPSS software (version 27.0; IBM, Armonk, NY, USA), with p-values <0.05 considered statistically significant. The Shapiro–Wilk test was used to assess normality. Quantitative data between groups were compared using the independent-samples t-test or Mann–Whitney U-test, as appropriate. Paired-sample t-tests or Wilcoxon tests were used to compare preoperative and final follow-up values within groups, including LL and local lordosis. Friedman analysis was applied for repeated measures of IH across preoperative, postoperative, and final follow-up assessments; p-values were adjusted to 0.0167 using Bonferroni correction for multiple comparisons. Categorical data were compared using the Chi-square or Fisher's exact test, as appropriate. Univariate logistic regression was used to identify potential predictors (P < 0.100) for inclusion in the multivariate logistic model. Multivariate logistic regression was performed, with results expressed as adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Variables with p < 0.05 were considered significant predictors of cage subsidence following SA-OLIF. The sensitivity, specificity, and optimal cutoff values for each predictor were determined by receiver operating characteristic (ROC) curve analysis, selecting the value corresponding to the maximum Youden index.
Sample size was calculated using PASS 15 (version 15; NCSS LLC, Kaysville, UT, USA). A pilot study including 55 patients meeting the inclusion and exclusion criteria was conducted. Sarcopenia, age, and sex were included in the multivariate logistic regression, yielding an OR of 4.141 for sarcopenia. With an expected effect size of 4.141, a desired statistical power of 0.8, and an alpha of 0.05, the minimum sample size was calculated as 96. Therefore, 98 subjects were included, meeting this threshold.
Results
Among the 98 patients included, 32 (32.7%) met the subsidence criteria and were classified as the subsidence group, while the remaining 66 (67.3%) constituted the non-subsidence group. Patient characteristics are presented in Table 1. In the subsidence group, 15 patients (46.9%) were diagnosed with sarcopenia, with a mean L3-SMI of 38.64 ± 6.83 cm^2^/m^2^. In the non-subsidence group, 12 patients (18.2%) were diagnosed with sarcopenia, with a mean L3-SMI of 43.71 ± 8.35 cm^2^/m^2^, representing a significant difference between groups (P = 0.003 and P = 0.001, respectively). Patients in the subsidence group were significantly older than those in the non-subsidence group (P = 0.005). The subsidence group also had lower BMD compared with the non-subsidence group (−2.05 ± 0.31 vs. −1.61 ± 0.43, P < 0.001). There were no significant differences between groups regarding BMI (23.93 ± 2.54 vs. 24.72 ± 3.06, P = 0.102), smoking status (15.6% vs. 10.6%, P = 0.702), surgical segment (P = 0.187), or fusion rate (90.6% vs. 93.9%, P = 0.858).
The radiological and clinical outcomes are presented in Table 2. In both groups, last follow-up LL and local lordosis Cobb angle were significantly increased compared with preoperative values (P < 0.001). In the non-subsidence group, the last follow-up IH was statistically greater than preoperative IH (10.80 ± 1.63 vs. 9.01 ± 1.73 mm, P < 0.001). In contrast, in the subsidence group, there was no significant difference between last follow-up IH and preoperative IH (9.44 ± 1.53 vs. 8.84 ± 1.66 mm, P = 0.401). There were no significant differences in IH between groups preoperatively or postoperatively. Last follow-up IH in the subsidence group was lower than in the non-subsidence group (10.80 ± 1.63 vs. 9.44 ± 1.53 mm, P < 0.001). ΔIH was 0.91 ± 0.60 mm in the non-subsidence group and 2.82 ± 0.71 mm in the subsidence group, showing a significant difference (P < 0.001). The last follow-up local lordosis Cobb angle in the non-subsidence group was significantly higher than that in the subsidence group, and the difference was statistically significant (P = 0.008). No significant differences were observed in cage height or length between the two groups. Clinical outcomes, assessed using ODI and JOA scores, improved significantly in both groups at the last follow-up. There were no significant differences in JOA or ODI scores between groups preoperatively or postoperatively. Postoperative low back pain was reported in seven patients (21.9%) in the subsidence group and six patients (9.1%) in the non-subsidence group, although this difference was not statistically significant.
Univariate analysis identified age (P = 0.004), BMD (P < 0.001), and sarcopenia (P = 0.004) as potential predictors for inclusion in the multivariate logistic model. Multivariate logistic regression (Table 3) revealed that age (OR = 1.113, 95% CI = 1.025–1.208, P = 0.011), BMD (OR = 0.059, 95% CI = 0.014–0.256, P < 0.001), and sarcopenia (OR = 3.881, 95% CI = 1.231–12.241, P = 0.021) were independent predictors of cage subsidence following SA-OLIF. ROC analysis of the multivariate model yielded an area under the curve (AUC) of 0.856 (P < 0.001) (Figure 2b).
Receiver operating characteristic (ROC) curve analysis. (a) The cutoff values of age and BMD were 59.5 and −1.9 respectively. (b) The area under the curve (AUC) in regard to logistic regression model was 0.856.
ROC analysis was also performed to evaluate the predictive value of age and BMD for cage subsidence in non-osteoporotic patients, with cutoff values determined using the Youden index (Figure 2a, Table 4). The AUC for age was 0.676, with a cutoff of 59.5 years (sensitivity 78.1%, specificity 48.5%). The AUC for BMD was 0.783, with a cutoff of −1.95 (sensitivity 77.3%, specificity 68.7%).
Discussion
Multiple diagnostic approaches for sarcopenia are currently available, including the measurement of muscle mass, assessment of muscle strength, evaluation of physical activity, and analysis of biomarkers (20). Among these, indicators of muscle mass and quality derived from CT are highly effective in assessing sarcopenia (21). The patients in this study were elderly with lumbar degenerative diseases and had limitations in performing functional tests, such as walking assessments, for sarcopenia evaluation. Therefore, although L3-SMI does not fully reflect physical function, it was employed as a simple and objective method to diagnose sarcopenia.
Cage subsidence is one of the most common complications following OLIF (22) and can lead to progressive spinal deformity and nerve compression (23). Currently, no standardized definition of cage subsidence exists, contributing to variability in reported subsidence rates (24). Kim et al. proposed a classification standard, defining cage subsidence as a disc height decrease of more than 2 mm, a criterion widely used in clinical practice (25). In the present study, the incidence of cage subsidence was 32.7%, consistent with previous reports by Hu et al. (26). A fundamental determinant in the occurrence of cage subsidence is the balance between the stress at the cage–vertebral endplate interface and the strength of the support at this interface. This balance is susceptible to various factors (27).
Multivariate logistic analysis in this study identified sarcopenia as an independent predictor of cage subsidence following SA-OLIF. Sarcopenia reflects malnutrition, physical disability, inactivity, increased frailty, and reduced quality of life, and has been associated with poorer surgical outcomes (28). Sun et al. retrospectively reviewed 314 patients aged 60–80 years who underwent single-segment posterior lumbar fusion and found that MRI-based central sarcopenia negatively affected visual analogue scale (VAS) scores for low back pain and ODI scores (29). Similarly, Matsuo et al. analyzed 178 patients with lumbar spinal stenosis (LSS) and reported that patients with LSS and sarcopenia exhibited greater vertebral slippage, lower BMI and BMD, reduced physical function, and more severe low back pain compared with those without sarcopenia (28). Our previous study of 116 patients also demonstrated that sarcopenic patients experienced a greater degree and higher incidence of postoperative low back pain, and the rate of cage subsidence was significantly higher in the sarcopenia group than in the non-sarcopenia group (15).
The findings of the present study support that sarcopenia is a predictor of cage subsidence. Patients with sarcopenia have weakened paraspinal musculature, and muscle dysfunction reduces the protective support of adjacent bone structures, increasing the risk of postoperative cage subsidence. With regard to the relationship between paraspinal muscles and cage subsidence, Kotheeranurak et al. identified multifidus muscle degeneration as a risk factor for cage subsidence following OLIF (22). Singhatanadgige et al. reported that when muscle degeneration occurs, the anterior spinal column, including the OLIF cage, absorbs higher compressive forces and is more prone to endplate violation and subsequent cage subsidence (30). Therefore, patients with preoperative sarcopenia are more prone to experiencing cage subsidence following SA-OLIF.
In the present study, BMD and age were also identified as independent predictors of cage subsidence following SA-OLIF. Our results showed that patients aged over 59.5 years were at higher risk of subsidence, consistent with the findings of Shen et al. (38). However, age showed only a moderate correlation with the extent of cage subsidence (AUC = 0.676). As an independent predictor, the clinical utility of age is limited due to its non-specific nature. Advanced age is often accompanied by declines in musculoskeletal quality and osteoporosis, which may be more directly captured by L3-SMI and BMD (31). Therefore, although age is a predictive factor, its modest predictive value suggests it should not serve as the sole criterion for surgical decision-making.
Previous studies (31, 32) have demonstrated that BMD decreases with age, reducing the load threshold for endplate failure and making it more susceptible to damage. A biomechanical analysis by Palepu et al. (33) found that, regardless of cage type, bone quality was strongly associated with the degree of cage subsidence. Similarly, Jones et al. reported that decreased endplate volumetric BMD was significantly correlated with an increased rate of subsidence (34). However, some reports have suggested that while BMD is the gold standard for assessing bone quality, it may be influenced by confounding factors such as spinal deformities, bowel contents, or aortic atherosclerosis, which can reduce measurement accuracy (35, 36).
In the present study, even in non-osteoporotic patients, BMD remained a significant predictor of cage subsidence following SA-OLIF. Patients with BMD between −1.9 and −2.5 exhibited insufficient vertebral endplate strength, increasing the risk of subsidence. Nonetheless, the predictive value of BMD was moderate (AUC = 0.783), consistent with previous studies. Zou et al. reported that Hounsfield units measured by quantitative computed tomography (qCT) more accurately assess bone quality than BMD (37). However, qCT is costly and exposes patients to higher radiological risks, limiting its use for routine examinations.
Given that cage subsidence is multifactorial, surgeons should consider all relevant factors to optimize outcomes. In this model, patients aged >59.5 years with low BMD (T-score <−1.9) and concomitant sarcopenia represent a high-risk cohort, with a strong correlation to cage subsidence (AUC = 0.856). Therefore, for those patients, instruments should be considered in the surgical plan to decrease the incidence rate of cage subsidence.
This study had several limitations. First, this was a single-center retrospective study with a relatively modest sample size, which may limit statistical power and introduce potential biases in patient selection and data collection. In future studies, a larger sample size might provide more generalizable and robust findings. Second, we only analyzed some common preoperative factors; the factors that may affect the cage subsidence after surgery need to be explored in future research. Third, although multiple methods exist for diagnosing sarcopenia according to EWGSOP guidelines, this study relied solely on L3-SMI and did not incorporate functional muscle assessments.
Conclusion
Cage subsidence following SA-OLIF was a common complication in non-osteoporotic patients, with an incidence rate of 32.7%. Preoperative sarcopenia, age >59.5 years, and a T-score <−1.9 were predictors of cage subsidence following SA-OLIF in non-osteoporotic patients. Patients with sarcopenia had nearly 4-fold increased odds of subsidence. OLIF with instruments may represent an alternative surgical method for patients with predictor factors to decrease the incidence of cage subsidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. (2012) 24(6):623–7. 10.1097/BOR.0b 013e 328358 d 59b 22955023 PMC 4066461 · doi ↗ · pubmed ↗
- 2Derstine BA Holcombe SA Goulson RL Ross BE Wang NC Sullivan JA Quantifying sarcopenia reference values using lumbar and thoracic muscle areas in a healthy population. J Nutr Health Aging. (2017) 21(10):180–5. 10.1007/s 12603-017-0983-329300439 PMC 12880485 · doi ↗ · pubmed ↗
- 3Nan Y Zhou Y Dai Z Yan T Zhong P Zhang F Role of nutrition in patients with coexisting chronic obstructive pulmonary disease and sarcopenia. Front Nutr. (2023) 10:1214684. 10.3389/fnut.2023.121468437614743 PMC 10442553 · doi ↗ · pubmed ↗
- 4Zhang N Zhu WL Liu XH Chen W Zhu ML Kang L Prevalence and prognostic implications of sarcopenia in older patients with coronary heart disease. J Geriatr Cardiol. (2019) 16(10):756–63. 10.11909/j.issn.1671-5411.2019.10.00231700515 PMC 6828602 · doi ↗ · pubmed ↗
- 5Jogiat U Jimoh Z Turner SR Baracos V Eurich D Bédard ELR. Sarcopenia in lung cancer: a narrative review. Nutr Cancer. (2023) 75(7):1485–98. 10.1080/01635581.2023.221242537177914 · doi ↗ · pubmed ↗
- 6Gibbons D Ahern DP Curley AE Kepler CK Butler JS. Impact of sarcopenia on degenerative lumbar spondylosis. Clin Spine Surg. (2021) 34(2):43–50. 10.1097/BSD.000000000000104733633055 · doi ↗ · pubmed ↗
- 7Mayer HM. A new microsurgical technique for minimally invasive anterior lumbar interbody fusion. Spine (Phila Pa 1976). (1997) 22(6):691–9. 10.1097/00007632-199703150-000239089943 · doi ↗ · pubmed ↗
- 8Cai K Luo K Zhu J Zhang K Yu S Ye Y Effect of pedicle-screw rod fixation on oblique lumbar interbody fusion in patients with osteoporosis: a retrospective cohort study. J Orthop Surg Res. (2021) 16(1):429. 10.1186/s 13018-021-02570-834217340 PMC 8254285 · doi ↗ · pubmed ↗