Lorazepam and Survival in Asian Patients with Pancreatic Cancer: A Retrospective Cohort Study
Tae Seung Lee, Jin Ho Choi, In Rae Cho, Jin Woo Park, Sang Hyub Lee, Ji Kon Ryu, Woo Hyun Paik

TL;DR
This study found that high-dose lorazepam use in Asian pancreatic cancer patients undergoing chemotherapy was linked to worse progression-free survival, but not overall survival.
Contribution
The study is the first to report an association between high-dose lorazepam and reduced progression-free survival in Asian pancreatic cancer patients.
Findings
High-dose lorazepam was associated with shorter progression-free survival (median 6 vs. 8 months).
No significant difference in overall survival was observed between high- and low-dose groups.
Higher cumulative lorazepam exposure correlated with worse progression-free survival outcomes.
Abstract
Lorazepam is frequently used in pancreatic cancer patients receiving chemotherapy for its antiemetic properties and to mitigate psychological distress. However, N-unsubstituted benzodiazepines like lorazepam may adversely impact pancreatic cancer progression by stimulating fibrosis and inflammatory signaling. This study aimed to retrospectively compare the survival rates of pancreatic cancer patients exposed to lorazepam with those who were not exposed to real-world clinical practice. Data were retrospectively reviewed from patients aged ≥ 18 years with pathologically confirmed pancreatic cancer who received palliative chemotherapy at Seoul National University Hospital between January 2011 and January 2023. Patients were dichotomized based on lorazepam administration: those who received ≥ 15 mg (equivalent to ≥ 1 tablet daily for 30 days) were classified as the high-dose group, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
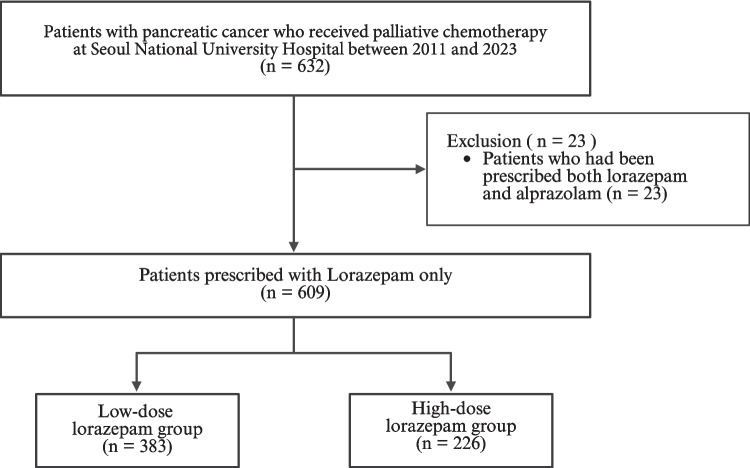 Figure 1
Figure 1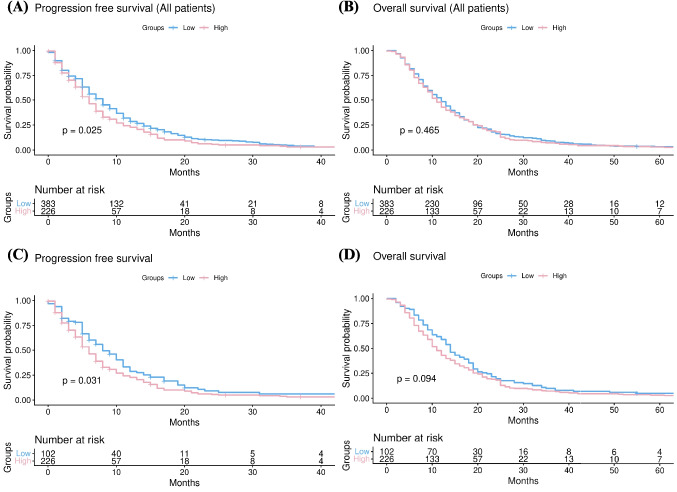 Figure 2
Figure 2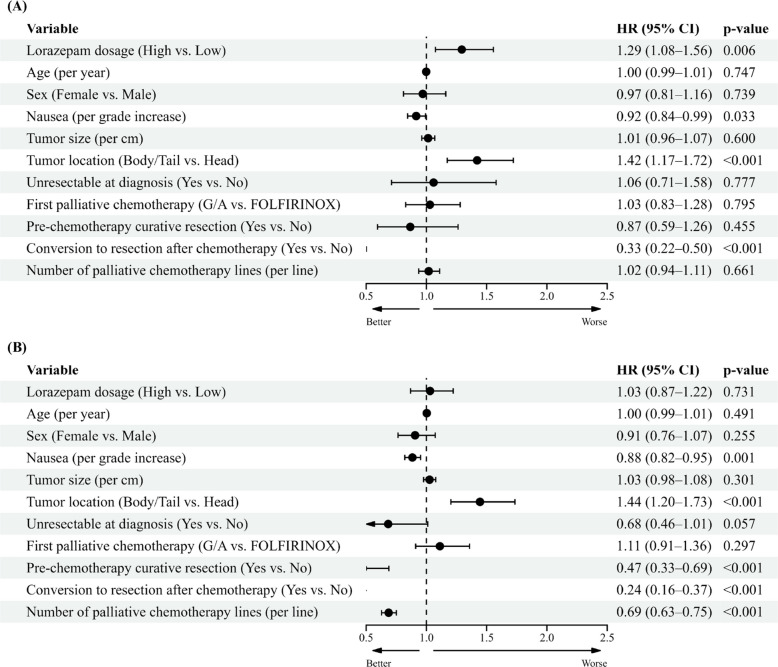 Figure 3
Figure 3- —Seoul National University Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Stress, Anesthesia, and Immune Response · Pain Management and Opioid Use · Nausea and vomiting management
Introduction
Pancreatic cancer is one of the most challenging cancers to treat with poor prognosis. Surgical resection is the only curative method, however, fewer than 20% of patients are eligible for surgery at the time of diagnosis, resulting in a five-year survival rate of about 13% [1]. This low eligibility is due to the aggressive nature of pancreatic cancer, which often progresses locally or metastasizes systemically in its early stages. At the time of diagnosis, about 50%–60% of patients are found to have metastatic disease [2], 25%–30% have locally advanced disease [2], and only 10%–15% are diagnosed with localized disease suitable for surgery [2]. Even after surgery, recurrence is common [2]. Furthermore, the incidence of pancreatic cancer is increasing globally, with an annual rise of 0.5%–1% observed in the United States and South Korea. By 2030, pancreatic cancer is projected to become the second leading cause of cancer-related deaths [3]. Despite advancements in anti-cancer treatments [4–7], pancreatic cancer still has a low five-year survival rate. This grave prognosis is largely attributed to the tumor microenvironment, which is characterized by the presence of cancer-associated fibroblasts (CAFs) [8]. These CAFs contribute to treatment resistance by fostering a desmoplastic and fibrotic environment that diminishes the efficacy of chemotherapy [9, 10].
Given these huddles, recent studies have emphasized the importance of palliative care in pancreatic cancer, highlighting its impact on both treatment management and patient outcomes [11]. Pancreatic cancer’s high recurrence rate leads to significant emotional distress, anxiety, and depression among patients [12–14]. From the perspective of comprehensive cancer care, psychosocial support has become increasingly recognized as an essential aspect of patient management. In particular, anxiety and depression induced by cancer-related symptoms and pain severely affect patients’ quality of life [12]. Additionally, anticipatory anxiety and chemotherapy-induced nausea can reduce treatment compliance, thereby worsening quality of life, and performance status, and treatment outcomes [15].
To cope with these cancer-related effects, patients are often prescribed various palliative care medications, such as selective serotonin reuptake inhibitors, opioids, and benzodiazepines. However, increasing evidence suggests that many of these medications may influence cancer risk, tumor progression [16], and the efficacy of chemotherapy [17], either positively or negatively. Specifically, lorazepam is widely used not only to alleviate psychological distress during chemotherapy but also as an antiemetic to manage anticipatory nausea [18, 19].
Recent study has revealed that N-unsubstituted benzodiazepines, including lorazepam, clonazepam, nordiazepam, and oxazepam, promote the expression of GPR68, a receptor commonly found in the CAFs of pancreatic cancer [11]. This receptor increases IL-6 production in CAFs, which activates fibrotic and inflammatory signaling pathways. These pathways promotes desmoplasia and ischemic necrosis, ultimately correlated with poor progression-free survival (PFS) in pancreatic cancer patients [11]. Conversely, N-substituted benzodiazepines, such as alprazolam, diazepam, and temazepam, do not stimulate GPR68 activation [11].
In addition to these mechanistic findings, a recent clinical study by Tsilimigras et al. [16] evaluated the association between long-term lorazepam use and survival outcomes in patients with pancreatic adenocarcinoma. The authors reported that prolonged lorazepam exposure was associated with worse progression-free survival, while no significant difference in overall survival was observed. Although this study provided important clinical insight, it was conducted predominantly in non-Asian populations and did not specifically evaluate cumulative dose-based stratification.
Nonetheless, clinical data on the impact of lorazepam on the prognosis of pancreatic cancer patients remain limited. Therefore, this study aims to retrospectively evaluate the prognosis of pancreatic cancer patients receiving chemotherapy, comparing outcomes based on lorazepam use, which is prescribed to alleviate psychological distress and manage anticipatory nausea.
Materials & Methods
Study Population
Patients aged ≥ 18 years with pathologically confirmed pancreatic cancer who received palliative chemotherapy at Seoul National University Hospital from January 2011 to January 2023, were enrolled in this study. All included patients were of Asian ethnicity, reflecting the single-race population of this single-center study conducted in Korea. As this is a retrospective study, informed consent was not obtained from the patients. The retrospective review included patients regardless of whether they underwent surgery or radiation therapy. All prescriptions for alprazolam and lorazepam up to the last follow-up date were reviewed, regardless of the cancer diagnosis. Patients who had been prescribed alprazolam, or both lorazepam and alprazolam, even once, were excluded from the study.
Patients were categorized into two groups based on cumulative lorazepam exposure, defined as the total prescribed dose aggregated across multiple prescription periods. In a previous study [16], outcomes were compared between patients exposed to lorazepam for ≥ 30 days and those with shorter exposure. Based on this concept, cumulative lorazepam dose was operationalized using a standard daily dose of 0.5 mg, corresponding to a 30-day exposure (15 mg). Accordingly, patients with a cumulative dose of < 15 mg (as a monthly total dose) were classified as the low-dose group, whereas those with ≥ 15 mg were classified as the high-dose group. Clinical and demographic parameters were retrospectively collected from electronic medical records, including age, sex, date of the initial imaging diagnosis of pancreatic cancer, tumor location and size, date of surgical resection, the initial and final dates of palliative chemotherapy, and the type of chemotherapy administered.
Study Outcomes
The main endpoints were progression-free survival (PFS) and overall survival (OS). Both PFS and OS were measured from the initiation date of first-line palliative chemotherapy. Disease progression was determined by the first radiological identification of a new lesion or recurrence. Death was recorded based on documented evidence, or if unavailable, verified using mortality data. For patients classified as hopeless discharge or lost to follow-up under critical conditions, the last recorded follow-up date was regarded as the date of death.
Statistical Methods
Qualitative variables were compared using the chi-square test or Fisher’s exact test, while quantitative variables underwent a normality assessment via the Shapiro–Wilk test. When analyzing continuous variables, the Student’s t-test was applied for normally distributed data, whereas the Mann–Whitney U-test was used for non-normal distributions. Categorical variables were examined with either the chi-square test or Fisher’s exact test. A p-value of ≤ 0.05 was considered statistically significant. All statistical tests were performed as two-sided tests, and relevant variables were included as covariates in further analyses.
For PFS (progression-free survival) and OS (overall survival), 95% confidence intervals (CIs) were estimated using the Kaplan–Meier method and reported as the median and range. The incidence of adverse events was expressed in percentages, with differences assessed via the chi-square test, applying a 5% significance level. Additionally, a multivariable Cox proportional hazards model was utilized to evaluate factors deemed clinically significant in their influence on PFS and OS.
Statement of Human and Animal Rights
This study was approved by the Institutional Review Board of Seoul National University hospital.
Results
Clinical Characteristics of the study population
Of the 632 patients, 23 who had been prescribed both lorazepam and alprazolam were excluded. The remaining 383 patients who were exposed to less than 15 mg of lorazepam were categorized as the low-dose group, while the 226 patients who were exposed to more than 15 mg of lorazepam were categorized as the high-dose group (Fig. 1).Fig. 1. Flow diagram of the study
In the baseline characteristics, the high-dose group had a statistically significantly higher proportion of younger patients (p = 0.037). However, a significantly greater percentage of patients in the high-dose group presented with unresectable disease at diagnosis compared to the low-dose group (81.9% vs. 89.8%, p = 0.012). Additionally, the low-dose group had a higher proportion of patients who underwent curative resection prior to chemotherapy (22.2% vs. 11.9%, p = 0.002). There were no differences between the two groups in terms of sex, tumor size, tumor location, conversion to resection, number of palliative chemotherapy line, palliative chemotherapy duration, no evidence of disease status, or follow-up duration (Table 1). Detailed information on palliative chemotherapy regimens by treatment line is provided in Supplementary Table 1.Table 1. Baseline characteristics of the study patients^^Low-dose groupHigh-dose groupp-value(N = 383)(N = 226)Sex0.288Male240 (62.7%)131 (58.0%)Female143 (37.3%)95 (42.0%)Age62.0 ± 9.160.2 ± 10.60.037Highest grade of chemotherapy related nausea/vomiting < 0.001No Adverse event40 (10.4%)11 (4.9%)Grade 173 (19.1%)29 (12.8%)Grade 230 (7.8%)9 (4.0%)Grade 3180 (47.0%)119 (52.7%)Grade 460 (15.7%)58 (25.7%)Lorazepam prescription dose (mg)1.8 ± 3.6185.4 ± 487.2 < 0.001Lorazepam prescription days0.9 ± 2.991.2 ± 488.20.006Tumor size (centimeter)3.7 ± 1.73.9 ± 1.90.189Tumor location0.155Head165 (43.1%)82 (36.3%)Body102 (26.6%)75 (33.2%)Tail116 (30.3%)69 (30.5%)Unresectable at diagnosis313 (81.9%)203 (89.8%)0.012Curative resection before chemotherapy85 (22.2%)27 (11.9%)0.002Conversion to resection20 (5.2%)11 (4.9%)0.999Line of palliative chemotherapy2.2 ± 1.02.2 ± 0.90.965Progression323 (84.3%)199 (88.1%)0.251Death372 (97.1%)221 (97.8%)0.818NED^†^ state3 (0.8%)2 (0.9%)1.000Palliative chemotherapy duration (months)12.9 ± 14.711.6 ± 10.70.211Follow up duration (months)15.6 ± 18.114.8 ± 16.20.608^^ Values are presented as mean ± standard deviation. Other values are presented as number (%)^†^NED, No evidence of disease
Primary and Secondary Endpoints
PFS was worse in the high-dose lorazepam group compared to the low-dose group [median, 6 months (5–7) vs. 8 months (7–9), p = 0.025] (Fig. 2A). However, there was no difference in OS between low-dose group and high-dose group [median, 11 months (10–12) vs. 12 months (11–13), p = 0.465] (Fig. 2B). Given the potential heterogeneity introduced by including patients with no lorazepam exposure in the low-dose group, we performed an additional subgroup analysis excluding these patients. This approach allowed us to specifically evaluate the dose–response relationship among patients who received lorazepam. In this subgroup, PFS remained significantly worse in the high-dose lorazepam group compared to the low-dose group [median, 6 months (5–7) vs. 8 months (7–11), p = 0.031] (Fig. 2C). However, there was no difference in OS between low-dose group and high-dose group [median, 11 months (10–12) vs. 14 months (13–17), p = 0.094] (Fig. 2D).Fig. 2. Comparison of (a) progression-free survival and (b) overall survival between high-dose and low-dose lorazepam groups in all patients, and (c) progression-free survival and (d) overall survival among patients treated with lorazepam
Covariate-Adjusted Analysis of PFS and OS Based on Lorazepam Usage
In the univariable Cox regression analysis for PFS, lorazepam dosage and tumor location (head) were associated with a higher hazard ratio (HR), indicating worse outcomes. In contrast, highest nausea/vomiting grade and conversion to curative resection after chemotherapy were associated with a lower HR, suggesting improved outcomes. For OS, older age and female was associated with a higher HR, whereas highest nausea/vomiting grade, whether curative surgery was performed before chemotherapy, conversion to curative resection after chemotherapy, and the number of palliative chemotherapy lines were associated with a lower HR (Table 2).Table 2. Univariable Cox regression analysis for (A) Progression-free survival (B) Overall survivalPFSOSHazard Ratio(95% Cl)p-valueHazard Ratio(95% Cl)p-valueLorazepam dosage(High vs. Low)1.23 (1.03–1.47)0.0231.06 (0.90–1.26)0.462Age (per year)1.00 (1.00–1.01)0.3631.01 (1.00–1.02)0.006Sex(Female vs. Male)0.92 (0.77–1.09)0.3390.84 (0.71–1.00)0.045Highest nausea/vomiting grade(per grade)0.92 (0.86–0.99)0.0300.83 (0.78–0.89) < 0.001Tumor size(Per centimeter)1.01 (0.97–1.06)0.6161.04 (1.00–1.09)0.069Tumor location(Head vs. body/tail)1.24 (1.04–1.48)0.0171.17 (1.00–1.39)0.055Unresectable at diagnosis(Yes vs. No)1.05 (0.83–1.34)0.6611.16 (0.92–1.46)0.205Pre-chemotherapy resection (Yes vs. No)0.95 (0.76–1.18)0.6200.73 (0.59–0.91)0.004Conversion to resection(Yes vs. No)0.33 (0.22–0.50) < 0.0010.24 (0.16–0.37) < 0.001First Line Chemotherapy(Gemcitabine/Nab-Paclitaxel vs. FOLFIRINOX)1.11 (0.92–1.35)0.2711.11 (0.32–1.32)0.245Total line of chemotherapy(Per the number of line)1.01 (0.94–1.09)0.7590.74 (0.69–0.80) < 0.001
A multivariable Cox regression analysis was performed, adjusting for factors such as lorazepam dosage, age, sex, highest nausea/vomiting grade, tumor size, tumor location, unresectable status at diagnosis, first chemotherapy regimen, whether curative surgery was performed before chemotherapy, conversion to surgery after chemotherapy, and the number of palliative chemotherapy lines. High-dose lorazepam was associated with a significantly higher HR for PFS [HR 1.29 (95% CI, 1.08–1.56), p = 0.006]. Also, head location of tumor [HR 1.42 (95% CI, 1.17–1.72), p < 0.001] was associated with a significantly higher HR for PFS. Conversely, the higher nausea grade [HR 0.92 (95% CI, 0.84–0.99), p = 0.033] and conversion to resection [HR 0.33 (95% CI, 0.22–0.50), p < 0.001], PFS was found to have a significantly lower HR (Fig. 3A).For OS, no significant difference was observed based on lorazepam dosage [HR 1.02 (95% CI, 0.86–1.21), p = 0.874]. In cases with head location of tumor [HR 1.45 (95% CI, 1.21–1.74), p < 0.001] was associated with a significantly higher HR for PFS. Conversely, the higher nausea grade [HR 0.88 (95% CI, 0.82–0.95), p = 0.001], whether curative surgery was performed before chemotherapy [HR 0.47 (95% CI, 0.33–0.69), p < 0.001], conversion to resection [HR 0.24 (95% CI, 0.16–0.37), p < 0.001], and the number of palliative chemotherapy [HR 0.69 (95% CI, 0.63–0.75), p < 0.001], OS was found to have a significantly lower HR (Fig. 3B).Fig. 3. Covariate − adjusted analysis of (a) Progression free survival and (b) Overall survival based on Lorazepam dosage
Discussion
Lorazepam is frequently used in clinical practice to manage chemotherapy-related anticipatory nausea and vomiting [18, 19]. Previous studies have demonstrated that lorazepam can promote the progression of pancreatic cancer by inducing IL-6 secretion from CAFs [11]. Additionally, a prior research suggested that long-term use of lorazepam might be associated with a worse prognosis in surgically resected pancreatic cancer patients [16]. However, This study included only 55%–60% of patients who received chemotherapy [16], a lower proportion compared to our study, which specifically compares survival outcomes based on lorazepam use in patients who received palliative chemotherapy.
Although data on ethnic differences in lorazepam metabolism are limited, benzodiazepines as a drug class are metabolized by hepatic enzymes that exhibit genetic polymorphisms [20]. Variations in the frequency of these polymorphic drug-metabolizing enzymes across racial and ethnic groups may lead to differences in drug exposure, duration of action, and clinical effects. In our study, similar to previous reports [11, 16], patients with a relatively higher cumulative dose of lorazepam tended to have shorter PFS compared with those in the lower cumulative dose group. Interestingly, no significant difference in OS was observed. This finding may in part reflect the homogeneous ethnic composition of the study population, as all patients were of Asian ethnicity, in whom differences in drug metabolism could potentially influence clinical outcomes. In addition, among patients receiving palliative chemotherapy, lorazepam might play a supportive role by alleviating anticipatory nausea and reducing psychological stress, which could help maintain chemotherapy adherence and allow prolonged treatment duration. Such effects might partially explain the absence of a significant difference in OS between groups [21].
Our study has several limitations: 1) Since the investigation was conducted retrospectively by reviewing prescription records, it does not fully reflect the actual intake of lorazepam. 2) The number of patients prescribed alprazolam alone was not sufficient for comparison 3) Although all patients received palliative chemotherapy, detailed information on the exact timing of lorazepam initiation relative to chemotherapy was not available, precluding time-dependent analyses. Therefore, the observed association between lorazepam exposure and progression-free survival should not be interpreted as causal, and residual confounding by symptom burden or treatment-related factors cannot be excluded.
In conclusion, higher cumulative lorazepam exposure was associated with shorter progression-free survival in Asian patients with pancreatic ductal adenocarcinoma receiving palliative chemotherapy. Given the retrospective design and lack of time-dependent exposure data, these findings should not be interpreted as causal. Further prospective studies are warranted to clarify the clinical implications of lorazepam use in this population.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 53 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1PD JE. Recent updates in the management of chemotherapy-induced nausea and vomiting. Asian J Pharm Clin Res. 2013;6(Suppl 1):5–10. https://journals.innovareacademics.in/index.php/ajpcr/article/view/323