Transcatheter Left Ventricular Restoration in Ischemic Heart Failure and Dilated Cardiomyopathy
Muhammad Mohid Haroon, Faizan Ahmad, Ramsha Ali, Saqlain Haider, Areehah Zafar Masood, Usama Yaseen, Taha Ahmad Zaka Ur Rehman, Muhammad Abdullah Sardar, Muhammad Umer, Shruthi Aswathappa, Muhammad Salman Sabri, Muhammad Muneeb Murtaza, Rubiya Ali, Sunny Kumar, Sameer Ali

TL;DR
A minimally invasive treatment for heart failure reduces left ventricular volume and improves heart function, but more research is needed to confirm long-term benefits.
Contribution
First meta-analysis synthesizing evidence across transcatheter left ventricular restoration devices for ischemic heart failure.
Findings
TLVR significantly reduced left ventricular end-diastolic volume and improved ejection fraction.
Revivent TC and AccuCinch showed consistent benefits, while Parachute results were variable.
Improvements in NYHA class suggest better symptoms, though KCCQ scores were not consistently significant.
Abstract
Ischemic heart disease is the leading global cause of death and frequently progresses to ischemic heart failure (IHF) after myocardial infarction through adverse left ventricular (LV)remodeling. Surgical LV restoration improves ventricular geometry and function but is limited by invasiveness and inconsistent outcomes. Transcatheter Left Ventricular Restoration (TLVR) has emerged as a minimally invasive alternative,employing devices such as Revivent TC, AccuCinch, and Parachute to reduce LV volume, wall stress, and improve LV ejection fraction (LVEF). While several studies have reported promising results, no prior meta‐analysis has synthesized the evidence across devices. This meta‐analysis followed PRISMA 2020 guidelines. PubMed, Embase, Scopus, and Cochrane Library were searched through July 2025. Eligible studies included adult patients with IHF or dilated cardiomyopathy undergoing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
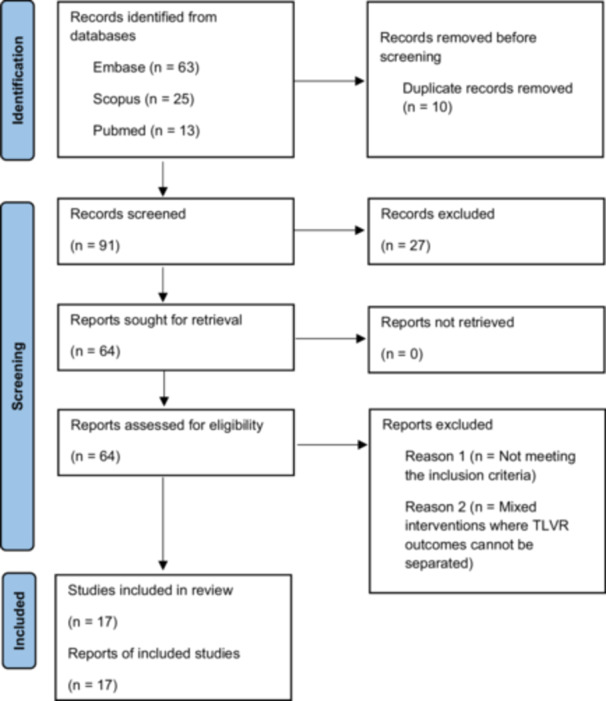 Figure 1
Figure 1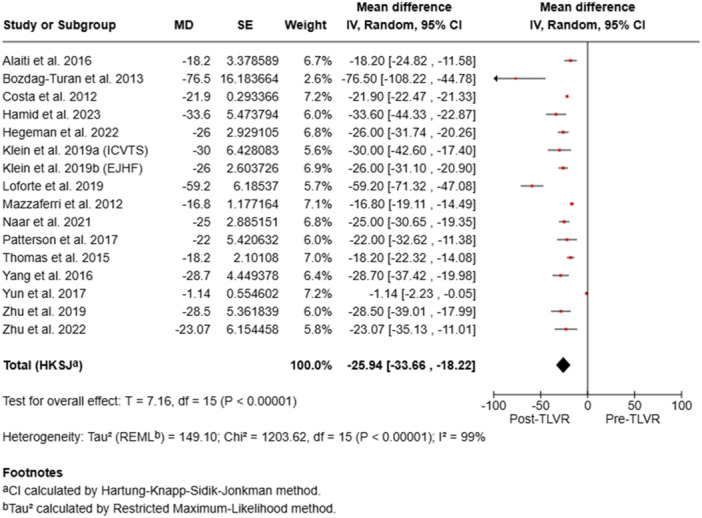 Figure 2
Figure 2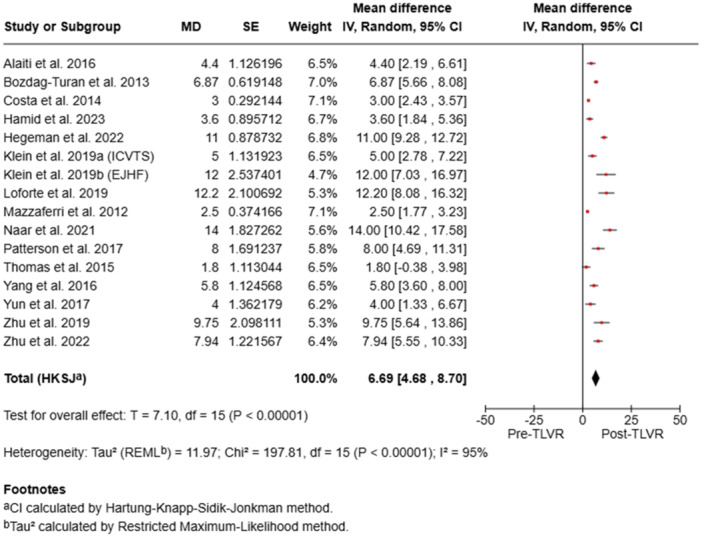 Figure 3
Figure 3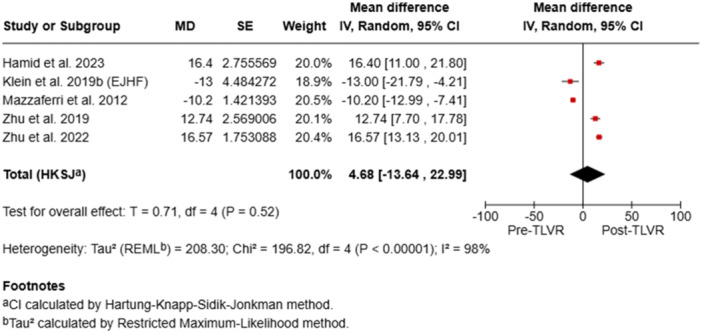 Figure 4
Figure 4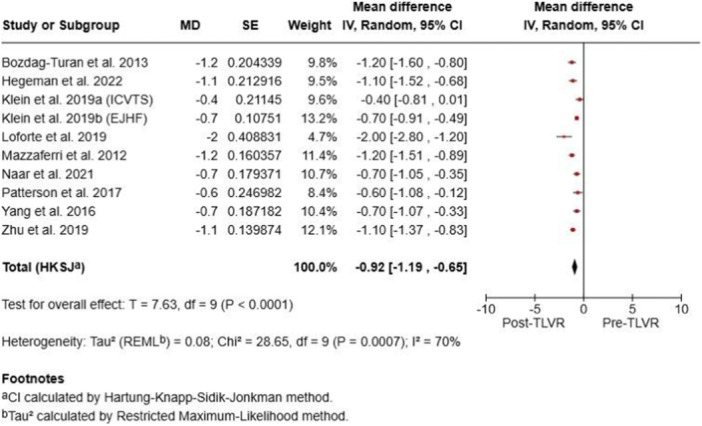 Figure 5
Figure 5| Author name | Year |
| Age (mean ± SD) | % Male | LVEF (%) | LVEDV (mL) | NYHA Class (Mean/% III–IV) | KCCQ score | Ischemic HF % | Device used | Follow‐up (months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alaiti et al. | 2016 | 32 | 59.6 ± 8.0 | 81% | 27.6 ± 6.9 | 122.4 ± 26.9 | 2.7/100% III–IV | N/A | 100% | Parachute® | 6 |
| Bozdag‐Turan et al. (Parachute) | 2013 | 8 | 62 ± 10 | 63% | 32 ± 6 | 122.2 ± 27.8 | 2.8 ± 0.7 | — | 100% | Parachute LVPD | 3 |
| Costa et al. (Parachute FIH) | 2012 | 39 | N/A | N/A | 15–40 | 127.5 | 2.0/N/A | N/A | 100% | Parachute | 36 |
| Costa et al. | 2014 | 39 | 56.4 ± 9.8 | 88% | 27.0 ± 1.1 | 127.7 ± 2.9 | 2.7/100% II–IV | N/A | 100% | Parachute® | 36 |
| Hamid et al. | 2023 | 51 | 56.3 ± 13.1 | 86% | 29.2 | 206 | 46% III–IV | 61.4 | 26% | AccuCinch TLVR | 12 |
| Hegeman et al. | 2022 | 30 | 62 ± 12 | 80.00% | < 40 | 84 ± 32 (index) | 3 ± 1/76% | — | 100% | Revivent TC System | 40.8 (3.4 years) |
| Klein et al. (ICVTS) | 2019 | 9 | 60 ± 8 | 89% | 28 ± 8 | 75 ± 23 (indexed) | 2.7 ± 0.4/Not reported | Not reported | 100% | Revivent TC | Not reported |
| Klein et al. | 2019 | 89 | 60.4 ± 9.9 | 80% | 29 ± 8 | 106 ± 33 (indexed) | 2.6 ± 0.5/59% III | Not reported | 100% | Revivent TC | 12 |
| Loforte et al. | 2019 | 7 | 72 ± 8.9 | 71% | 22.8 ± 8.1 | 137.2 ± 20.1 (indexed) | 3.4 ± 0.6/100% III–IV | Not reported | 100% | Revivent TC | 6.3 (mean) |
| Mazzaferri et al. | 2012 | 39 | 56.4 ± 8.6 | 87% | ≤ 40 | 127.2 ± 4.2 (index) | 3/76% | 38.6 ± 5.1 | 100% | Parachute Device | 12 |
| Naar et al. (Revivent TC) | 2021 | 23 | 59 ± 11 | 65% | 32 ± 7 | 107 ± 27 | 2.3/13% | N/A | 100% | Revivent TC | 61.2 (mean) |
| PARACHUTE III (Thomas et al.) | 2015 | 100 | 62.8 ± 10.4 | 81% | 29.2 ± 7.9 | 117.3 ± 26.3 (indexed) | 2.6 ± 0.5/56% III | Not reported | 100% | Parachute | 12 |
| Patterson et al. (Parachute III) | 2017 | 10 | 61.0 ± 10.4 | 90% | 38 ± 11 | 235 ± 81 | 2.6/40% | N/A | 100% | Parachute | 6 |
| Yang et al. | 2016 | 31 | 57.1 ± 10.4 | 94% | 30 | 110.8 | 6.4% III | — | 100% | Parachute® LVPD | 3 |
| Yun et al. | 2017 | 28 | 58.3 ± 7.2 | 79% | Not reported | Not reported | 20 (71.4% III) | Not reported | 100% | Parachute LVPD | 6 |
| Zhu et al. | 2019 | 16 | 60.9 ± 9.8 | 87.50% | 32.5 | 106.3 | 50% III | — | 100% | Heartech® LVPD | 1.2 (36 days) |
| Zhu et al. | 2022 | 16 | 60.93 ± 9.75 | 88% | 32.75 ± 6.84 | 105.00 (IQR: 90.00–130.00) | 2.7 (71.4% III) | Not reported | 100% | Heartech LVPD | 12 ± 1 |
| Study | Year |
| Pre‐LVEDV mean (SD) | Post‐LVEDV mean (SD) | Mean difference | 95% CI | Weight (%) |
|---|---|---|---|---|---|---|---|
| Alaiti et al. | 2016 | 32 | 122.4 (27.1) | 104.2 (30.3) | −18.2 | −25.1, −11.3 | 100 |
| Bozdag‐Turan | 2013 | 8 | Not reported | Not reported | −76.5 | −116.0 to −36.8 | 100 |
| Costa | 2012 | 31 | 127.7 (2.92) | 105.8 (3.02) | −21.9 | [−22.5, −21.3] | 30 |
| Costa | 2014 | 39 | 127.5 ± N/A | 106.7 ± N/A | −20.8 | N/A | N/A |
| Hamid et al. | 2023 | 51 | 206.0 (55.8) | 172.4 (52.8) | −33.6 | [−44.6, −22.6] | 50 |
| Hegeman | 2022 | 30 | 84 ± 32 | 58 ± 25 | −26 | −32 to −20 | 30 |
| Klein et al. (2018) | 2019 | 9 | 75.0 (23.0) | 45.0 (6.0) | −30 | [−45.2, −14.8] | 10 |
| Klein et al. (2019) | 2019 | 67 | 106.0 (33.4) | 80.0 (26.0) | −26 | [−31.2, −20.8] | 25 |
| Loforte et al. | 2019 | 7 | 137.2 (20.1) | 78.0 (10.2) | −59.2 | [−75.1, −43.3] | 15 |
| Mazzaferri | 2012 | 28 | 127.2 (4.2) | 110.4 (4.6) | −16.8 | [14.2, 19.4] | 33.3 |
| Naar | 2021 | 23 | 107 ± 27 | 82 ± 21 | −25 | −31 to −19 | 19 |
| Patterson | 2015 | 10 | 235 (81) | 100 ± 55 | −22 | −34 to −9 | 20 |
| Thomas et al. | 2017 | 64 | 117.3 (26.3) | 99.1 (27.3) | −18.2 | [−22.4, −14.0] | 20 |
| Yang et al. | 2016 | 31 | 110.8 (26.1) | 82.1 (21.3) | −28.7 | [−37.8, −19.6] | 30 |
| Yun et al. | 2017 | 28 | 97.66 (34.68) | 96.52 (33.04) | −1.14 | [−6.00, 3.72] | 33.3 |
| Zhu et al. | 2019 | 16 | 105.00 (90.00–130.00)* | 76.50 (57.75–120.25)* | −28.5 | [−40.00, −17.00] | 33.3 |
| Zhu et al. | 2022 | 16 | 106.27 (28.01) | 83.20 (16.87) | −23.07 | [−36.27, −9.87] | 20 |
| Study | Year | Sample size ( | Pre‐LVEF mean (SD) | Post‐LVEF mean (SD) | Mean difference | 95% CI | Weight (%) |
|---|---|---|---|---|---|---|---|
| Alaiti et al. | 2016 | 32 | 27.5 (6.9) | 31.9 (8.4) | 4.4 | [2.1, 6.7] | 30 |
| Bozdag‐Turan et al. | 2013 | 8 | 32 ± 6 | 38.87 ± 6.39* | 6.87 | (5.36; 8.39) | — |
| Costa et al. (2012) | 2012 | 39 | Not reported | Not reported | Not reported | Not reported | — |
| Costa et al. (2014) | 2014 | 31 | 27.0 (1.13) | 30.0 (1.17) | 3 | [NR] | NR |
| Hamid et al. (AccuCinch) | 2023 | 51 | 29.2 (4.8) | 32.8 (7.3) | 3.6 | [1.8, 5.4] | 63.8 |
| Hegeman et al. (2022) | 2022 | 30 | 33 ± 8 | 44 ± 10 | 11 | [9.2, 12.8] | 100 |
| Klein et al. (Revivent TC) | 2019 | 64 | 29 (8) | 34 (9) | 5 | [NR] | NR |
| Klein et al. | 2019 | 9 | 28.00 (8.00) | 40.00 (10.00) | 12 | [6.00, 18.00] | 100 |
| Loforte et al. | 2019 | 7 | 22.8 (8.1) | 35.0 (7.2) | 12.2 | [6.8, 17.6] | 15 |
| Mazzaferri et al. (2012) | 2012 | 28 | 26.9 (1.4) | 29.4 (1.4) | 2.5 | [NR] | NR |
| Naar et al. (2021) | 2021 | 23 | 32 ± 7 | 46 ± 15* | 14 | [10.2, 17.8] | 100 |
| Patterson et al. (2017) | 2015 | 10 | 38 ± 11 | 46 ± 14 | 8 | [4.1, 11.9] | 100 |
| Thomas et al. (PARACHUTE III) | 2017 | 97 | 29.2 (7.9) | 31.0 (7.6) | 1.8 | [NR] | NR |
| Yang et al. (2016) | 2016 | 31 | 30.0 ± 5.4 | 35.8 ± 6.8 | 5.8 | [3.5, 8.1] | 100 |
| Yun et al. | 2017 | 28 | 31.00 (10.00) | 35.00 (10.00) | 4 | [1.20, 6.80] | 100 |
| Zhu et al. | 2019 | 16 | 32.75 (6.84) | 42.50 (IQR: 34.75–50.25)* | 9.75 | [5.25, 14.25] | 100 |
| Zhu et al. (Heartech®) | 2022 | 16 | 32.47 (6.98) | 40.41 (6.15) | 7.94 | [5.32, 10.56] | 20 |
| Study (Author) | Year |
| Pre‐NYHA (mean ± SD or % class III–IV) | Post‐NYHA | Mean/proportional change | 95% CI | Weight (%) |
|---|---|---|---|---|---|---|---|
| Alaiti et al. | 2016 | 32 | 50% class III | 45% class I, 55% class II (improved group) | 85% improved/maintained | N/A | N/A |
| Bozdag‐Turan et al. | 2013 | 8 | 2.8 ± 0.7 (100% class II–IV) | 1.6 ± 0.5 | −1.2 | −1.7 to −0.7 | 20 |
| Costa et al. | 2012 | 31 | 100% class II–IV | 52% improved, 33% no change, 15% worsened | 48% improvement in LVEF | N/A | N/A |
| Costa et al. | 2014 | 39 | 2.0 (NYHA class II–IV) | 1.9 (87% symptom improvement) | −0.1 (mean reduction) | N/A | N/A |
| Hamid et al. (AccuCinch®) | 2023 | 51 | 46% class III–IV | 29% class III–IV | 17% reduction in class III–IV | — | — |
| Hegeman et al. | 2022 | 30 | 3 ± 1 (76% class III–IV) | 1.9 ± 0.6 (76% class I–II) | −1.1 (mean reduction) | N/A | N/A |
| Klein (Revivent TC) | 2019 | 77 | 2.6 ± 0.5 | 1.9 ± 0.8 | 26% Change | — | — |
| Klein et al. | 2019 | 9 | 2.7 ± 0.4 (100% class II–IV) | 2.3 ± 0.7 | −0.4 | −0.9 to +0.1 | 15 |
| Loforte et al. | 2019 | 7 | 3.4 ± 0.6 | 1.4 ± 0.9 | 2.0 point reduction | N/A | N/A |
| Mazzaferri et al. (2012) | 2012 | 28 | 2.5 ± 0.6 (median class III) | 1.3 ± 0.6 | Mean reduction: −1.2 classes |
| N/A |
| Naar et al. | 2021 | 23 | 2.3 ± 0.5 | 1.6 ± 0.7 | −0.7 (mean reduction) | N/A | N/A |
| Patterson et al. | 2015 | 10 | 2.5 ± 0.5 (40% class III) | 1.9 ± 0.6 (50% class I–II) | −0.6 (mean reduction) | N/A | N/A |
| Thomas (PARACHUTE III) | 2017 | 97 | 56% class III, 44% class II | 19.6% class I, 46.4% class II, 18.6% class III | 43% improved ≥ 1 class | — | — |
| Yang et al. | 2016 | 31 | 2.3 ± 0.5 (6.4% class III) | 1.6 ± 0.7 (60% class I) | −0.7 (mean reduction) | N/A | N/A |
| Yun et al. (2017) | 2017 | 28 | 71.4% class III | 17.9% class III | 53.5% reduction in class III | N/A | N/A |
| Zhu et al. | 2019 | 16 | 2.7 ± 0.4 (100% class II–IV) | 1.6 ± 0.5 | −1.1 | −1.4 to −0.8 | 25 |
| Zhu et al. (Heartech®) | 2022 | 16 | 50% class III | 0% class III | 50% reduction in class III | — | — |
| Study | Year |
| Pre‐KCCQ mean (SD) | Post‐KCCQ mean (SD) | Mean difference | 95% CI | Weight (%) |
|---|---|---|---|---|---|---|---|
| Alaiti et al. | 2016 | 32 | — | — | — | — | — |
| Bozdag‐Turan et al. | 2013 | 8 | — | — | — | — | — |
| Costa | 2012 | 39 | Not reported | Not reported | Not reported | N/A | N/A |
| Costa et al. | 2014 | 31 | Not reported | Not reported | Not reported | N/A | N/A |
| Hamid et al. | 2023 | 47 | 61.4 (26.0) | 77.7 (19.0) | 16.4 (18.7) | [10.9, 22.0] | — |
| Hegeman et al. | 2022 | 30 | Not reported | Not reported | Not reported | N/A | N/A |
| Klein | 2019 | 9 | Not reported | Not reported | Not reported | — | — |
| Klein | 2019 | 46 | 39 ± 21 | 26 ± 22 | −13 | — | — |
| Loforte | 2019 | 7 | Not reported | Not reported | Not reported | N/A | N/A |
| Mazzaferri et al. | 2012 | 28 | 38.6 (6.1) | 28.4 (4.4) | −10.2 | N/A | N/A |
| Naar et al. | 2021 | 23 | Not reported | Not reported | Not reported | — | — |
| Patterson et al. | 2015 | 10 | Not reported | Not reported | Not reported | — | — |
| Thomas | 2017 | 100 | Not reported | Not reported | Not reported | — | — |
| Yang et al. | 2016 | 31 | Not reported | Not reported | Not reported | — | — |
| Yun et al. | 2017 | 28 | — | — | — | — | — |
| Zhu et al. | 2019 | 15 | 65.93 (11.25) | 78.67 (8.35) | 12.74 | [10.9, 22.0] | — |
| Zhu et al. | 2022 | 16 | 65.93 (11.25) | 82.50 (5.44) | 16.57 | [12.81, 20.33] | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac Fibrosis and Remodeling · Mechanical Circulatory Support Devices
Introduction
1
Ischemic heart disease (IHD) is the leading cause of death worldwide and, if not treated or diagnosed, can develop into ischemic heart failure (IHF) [1]. Following acute myocardial infarction (AMI), adverse left ventricular (LV) remodeling often occurs, with increased LV volumes and reduced ejection fraction (LVEF) due to increased wall tension, loss of orientation of the myocardial fibers, and scarring.
Evidence shows that both pharmacologic and non‐pharmacologic therapies such as cardiac resynchronization therapy can improve survival in patients with LV systolic dysfunction by reducing LV volumes, either ESV or EDV, with bigger reductions associated with better survival outcomes [2]. Where medical treatment is insufficient, surgical interventions are available to correct the form, size, and function of the LV [3].
Surgical restoration of the LV has been used to remodel the dilated failing ventricle and improve chamber architecture and performance. Its use is limited, however, by the invasiveness of the procedure and heterogeneity of outcomes across studies [4].
Transcatheter Left Ventricular Restoration (TLVR) is an alternative, less invasive method attempting to reduce LV volume, wall stress, and improve EF by plicating fibrotic scar tissue [1]. AccuCinch system, BioVentrix LIVE system, Parachute device, and Revivent TC system are examples of the systems investigated in this patient population.
While individual studies have reported promising improvement in EF and quality of life following TLVR, no meta‐analysis to our knowledge has synthesized the evidence collectively or compared device results. This study aims to address this gap by systematically reviewing the literature on TLVR and performing a comparative analysis of device‐specific outcomes.
Methods
2
Study Design and Protocol Registration
2.1
This systematic review and meta‐analysis was conducted in line with the updated 2020 guidelines of the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA). The review protocol was prospectively registered in PROSPERO (Registration ID: CRD420251231767). The protocol was developed a priori following the PICO framework to ensure methodological rigor and transparency. The review protocol was developed a priori in accordance with the PICO framework.
Eligibility Criteria
2.2
Studies were included if they met the following criteria:
Population (P)
2.2.1
Adult patients with ischemic heart failure (IHF) or dilated cardiomyopathy undergoing transcatheter left ventricular restoration (TLVR).
Intervention (I)
2.2.2
TLVR performed using devices such as Revivent TC, AccuCinch, Heartech LV Partitioning Device, Parachute device, or similar technologies.
Comparator (C)
2.2.3
Only single‐arm designs were included, and no direct comparator arm was required. This restriction was applied because comparative data for TLVR remain limited, and most published studies report single‐arm outcomes.
Outcomes (O)
2.2.4
At least one of the following outcomes reported: left ventricular ejection fraction (LVEF), left ventricular end‐diastolic volume (LVEDV), New York Heart Association (NYHA) functional class, Kansas City Cardiomyopathy Questionnaire (KCCQ) scores.
We included prospective and retrospective observational studies, non‐randomized clinical trials, and randomized controlled trials reporting single‐arm TLVR outcomes.
Exclusion Criteria
2.2.5
Case reports, review articles, editorials, conference abstracts without full data, animal studies, and studies without extractable outcome measures were excluded.
Search Strategy and Databases
2.3
A comprehensive literature search was conducted in PubMed/MEDLINE, Embase, Scopus, and the Cochrane Library covering studies from inception to July 2025. The search strategy combined controlled vocabulary (e.g., MeSH terms) and relevant keywords, including “transcatheter left ventricular restoration,” “Parachute device,” “Revivent TC,” “AccuCinch,” and “ventricular partitioning.” Boolean operators AND and OR were used to combine search terms.
All retrieved articles were imported into Rayyan AI for initial screening. Title and abstract screening was performed first, followed by removal of duplicates within Rayyan. Four reviewers independently performed full‐text screening of potentially eligible studies, with disagreements resolved through consensus or, when necessary, adjudicated by a senior reviewer.
Study Selection
2.4
A total of 101 records were retrieved from electronic databases. Ten duplicate records were removed within Rayyan AI, leaving 91 records for title and abstract screening by six independent reviewers. During this stage, 27 records were excluded, and the remaining 63 reports were sought for retrieval. Two reports could not be retrieved, resulting in 61 full‐text articles assessed for eligibility. Four reviewers then conducted detailed full‐text screening, after which 17 studies met the inclusion criteria and were included in the final review. Any disagreements at any stage were resolved through discussion or consultation with a senior reviewer (PRISMA flow diagram, Figure 1).
PRISMA flow diagram for transcatheter left ventricular restoration systematic review. [Color figure can be viewed at wileyonlinelibrary.com]
Data Extraction
2.5
Four independent reviewers used a standardized data extraction sheet in Microsoft Excel to document all relevant information. The following data were collected:
Study profile: Study ID, first author, year of publication, country, study design, sample size, follow‐up duration.
Baseline Characteristics
2.6
Mean age, percentage of male patients, baseline LVEF, baseline LVEDV, NYHA class distribution, comorbidities, and medication use.
Intervention Details
2.6.1
Device type, procedural technique, and peri‐procedural protocols.
Outcomes
2.6.2
Baseline and follow‐up values for LVEF, LVEDV, LV end‐systolic volume (LVESV), NYHA class, KCCQ scores.
Quality Assessment
2.7
The methodological quality of included studies was assessed using an adapted case–control version of the Newcastle–Ottawa Scale (NOS). The NOS evaluates three key domains: Selection, including the adequacy of case definitions, representativeness of cases, selection of controls, and definition of controls; Comparability, assessing whether cases and controls are comparable based on key confounding variables; and Exposure, which examines the ascertainment of exposure, consistency of exposure assessment across groups, and the extent of non‐response. Detailed NOS scoring for all included studies is presented in the Supporting information Table 1.
Statistical Analysis
2.8
All statistical analyses were performed using Revman web software. Continuous outcomes were pooled as mean difference (MD) with standard error (SE) were calculated using a random‐effects model. The Hartung–Knapp–Sidik–Jonkman (HKSJ) method was applied to compute 95% confidence intervals (CIs). Between‐study variance (τ²) was estimated using the Restricted Maximum Likelihood (REML) method. Heterogeneity was assessed using the Cochran's Q test (χ²) and quantified with the I² statistic, with p < 0.10 indicating significant heterogeneity. A test for the overall effect was conducted using a t‐statistic, and results with p < 0.05 were considered statistically significant. Publication bias was evaluated using funnel plot asymmetry and Egger's regression test. Sensitivity analyses were conducted by sequentially excluding each study to assess the robustness of pooled estimates.
Results
3
Study Selection
3.1
The initial database search identified 101 records. After removing 10 duplicates, 91 unique articles were screened by title and abstract. Of these, 27 were excluded for not meeting the inclusion criteria. The remaining 64 underwent full‐text screening, and 17 studies met the eligibility criteria for inclusion (Figure 1).
Study Characteristics
3.2
Seventeen studies (Table 1) evaluating transcatheter left ventricular restoration (TLVR) in patients with heart failure were included in the pooled analysis. Across studies, the study population comprised predominantly older adults (mean age 58–62 years) and males (65%–94%), reflecting the typical TLVR demographic. Baseline left ventricular ejection fraction (LVEF) ranged from 22.8% to 38%, indicating severe systolic dysfunction. Left ventricular end‐diastolic volume (LVEDV) varied widely (75–235 mL), with the largest volumes observed in Parachute device cohorts, reflecting greater ventricular dilation in these populations.
Most patients were New York Heart Association (NYHA) Class II–IV at baseline, with advanced symptoms (Class III–IV) more frequent in Revivent TC studies (59%–76%) than in Parachute trials (e.g., 6.4% Class III in Yang et al.). Ischemic cardiomyopathy was the predominant etiology in nearly all studies except Hamid et al., where 26% of patients had non‐ischemic heart failure. Follow‐up durations ranged from 1.2 months (Zhu et al.) to 5 years (Naar et al.) (Table 1).
LVEDV Outcomes
3.3
All studies demonstrated post‐procedural LVEDV reduction, ranging from –76.5 mL to –1.14 mL, with the most pronounced decreases reported by Loforte et al. (–59.2 mL) and Hamid et al. (–33.6 mL). These findings indicate consistent reverse remodeling following TLVR (Table 2).
LVEF Outcomes
3.4
Baseline LVEF ranged from 22.8% to 38%. Post‐intervention improvements varied between +1.8% (Thomas et al., 2017) and +14% (Naar et al., 2021), with the largest relative gain observed in Klein et al. Notably, larger trials such as Hamid et al. (n = 51) and Thomas et al. (n = 97) also demonstrated clinically meaningful improvements (Table 3).
NYHA Functional Class
3.5
Functional capacity improved in all studies, with marked reductions in the prevalence of advanced heart failure. For example, in Yun et al., Class III/IV patients decreased from 71% to 18%, and in Zhu et al., from 50% to 0%. Costa et al. (2012) reported worsening in 15% of patients (Table 4).
KCCQ Scores
3.6
Kansas City Cardiomyopathy Questionnaire (KCCQ) scores improved in most studies, reflecting enhanced quality of life and symptom relief. Significant mean increases were reported by Hamid et al. (+16.4) and Zhu et al. (+12.7 to +16.6), whereas Klein et al. and Mazzaferri et al. observed declines. Incomplete paired KCCQ data precluded formal meta‐analysis (Table 5). Overall pooled KCCQ results were not statistically significant (MD + 4.68; 95% CI –13.64 to 22.99; p = 0.52), likely due to incomplete reporting and heterogeneity.
Pooled Outcomes
3.7
Pooled analyses demonstrated statistically significant improvements in LVEDV (mean difference [MD] –25.94 mL; 95% confidence interval [CI] –33.66 to –18.22; p < 0.00001), LVEF (MD + 6.69%; 95% CI 4.68–8.70; p < 0.00001), and NYHA class (MD –0.73; 95% CI –1.29 to –0.18; p = 0.02), with no significant change in KCCQ scores (MD + 4.68; 95% CI –13.64 to 22.99; p = 0.52). Substantial heterogeneity (I² > 90%) was observed across all analyses (Figure 2). Overall, TLVR was associated with favorable ventricular remodeling, improved systolic performance, and better functional capacity in patients with ischemic heart failure, despite considerable between‐study variability.
Pooled analysis of studies. [Color figure can be viewed at wileyonlinelibrary.com]
To minimize repetition, forest plots of pooled outcomes (LVEF, LVEDV, and NYHA class) were generated (Figures 2, 3, 4, 5), providing concise visualization of consistent post‐TLVR improvements across studies.
Pooled analysis of studies. [Color figure can be viewed at wileyonlinelibrary.com]
Pooled analysis of studies. [Color figure can be viewed at wileyonlinelibrary.com]
Pooled analysis of studies. [Color figure can be viewed at wileyonlinelibrary.com]
Discussion
4
To our knowledge, this is the first systematic review to evaluate the efficacy and safety of various transcatheter left ventricular restoration (TLVR) using the Revivent TC, Parachute HeartTech LVPD, or AccuCinch devices.
TLVR is designed to reduce LV volumes and restore physiologic geometry in patients with ischemic cardiomyopathy [4]. While huge research has been conducted on surgical reconstruction of the left ventricle, evidence remains variable, and the procedure is usually reserved for selected patients at centers of excellence [5]. The STICH trial, which compared CABG alone to CABG plus surgical LV aneurysmectomy, failed to demonstrate a survival benefit [6].
In contrast, TLVR represents a percutaneous alternative to surgical ventricular reconstruction (SVR), such as that studied in the STICH and RESTORE trials. Unlike SVR, which requires cardiopulmonary bypass and ventriculotomy, TLVR aims to achieve comparable geometric restoration and reduction in wall stress through a catheter‐based approach, potentially lowering procedural morbidity and recovery time.
TLVR was seen as a minimally invasive choice, particularly for patients with anteroapical aneurysm or akinetic scar after myocardial infarction, who might benefit from reducing the volume of the left ventricle [5]. Early outcomes from studies investigating TLVR show encouraging gains [7]. Klein et al recently published substantial decreases in LV volumes, improvement in ejection fraction, and symptomatic benefit at 12 months using the Revivent anchoring system. In this study, patients with a lower LVESVI demonstrated the greatest response [8]. Similarly, Wang et al recently showed significant benefits with Revivent TC in terms of LV volume, ejection fraction, 6‐min walk test and NYHA heart failure class, 9 months after the operation [9].
Comparison With Prior Studies
4.1
Our meta‐analysis reinforces these observations seen in other studies and show consistent benefit with TLVR throughout the trials. While baseline LV volumes were heterogeneous between the studies, TLVR was uniformly linked with significant reverse remodeling of the ventricle and functional improvement. Our meta‐analysis showed a mean reduction of LVEDV of –25.94 mL (95% CI: –33.66 to –18.22; p < 0.00001) and improvement of LVEF by +6.69% (95% CI: 4.68–8.70; p < 0.00001). Functional outcomes mirrored these structural gains, with mean NYHA class reduction of –0.73 (95% CI: –1.29 to –0.18; p = 0.02). Quality of life, as defined by KCCQ, was slightly better but not significant (MD + 4.68; 95% CI: –13.64 to 22.99; p = 0.52).
Heterogeneity and Patient Selection
4.2
Heterogeneity among studies likely reflects differences in device design (e.g., apical vs. basal remodeling mechanisms), patient selection (extent and location of scar, baseline LV size), and procedural learning curve. For instance, apically applied systems such as the Parachute device may favor patients with anteroapical dyskinesis, whereas Revivent and AccuCinch systems address broader LV geometry and wall stress reduction.
All devices reduced LVEDV and improved LVEF, with Revivent and AccuCinch showing the greatest benefit. Parachute showed the greatest variability amongst studies with excellent results seen in some and slight benefit seen in others. This variability underscores the importance of patient‐device matching and highlights a key source of heterogeneity in reported outcomes. Variability across studies can be attributed to heterogeneity in patient populations, differences in device deployment techniques, and inclusion of patients unlikely to derive benefit from TLVR.
Clinical Implications
4.3
The observed improvements in LV geometry and function suggest that TLVR may serve as an adjunctive or bridging option in the heart failure management algorithm—potentially fitting between guideline‐directed medical therapy (GDMT) and advanced interventions such as cardiac resynchronization therapy (CRT) or left ventricular assist device (LVAD) implantation. By targeting structural remodeling rather than solely hemodynamic optimization, TLVR offers a mechanistic complement to existing therapies.
In current heart failure management, transcatheter left ventricular restoration (TLVR) represents a minimally invasive option for patients with ischemic cardiomyopathy who remain symptomatic despite guideline‐directed therapy and are not candidates for surgical reconstruction or durable LVAD implantation. By restoring ventricular geometry and reducing end‐diastolic volume, TLVR can enhance systolic function and functional capacity while avoiding the morbidity of open surgery or long‐term mechanical support. As evidence and experience expand, TLVR may assume an intermediate role within existing heart failure algorithms, complementing CRT and bridging the gap between medical therapy and advanced mechanical interventions (4, 8, 9). Future heart failure guidelines may consider TLVR as a bridge or adjunct to CRT or LVAD in carefully selected patients with ischemic cardiomyopathy.
Limitations
4.4
Our findings in the meta‐analysis are limited by heterogeneity of study design, small sample size, and heterogeneous follow‐up. Results long‐term, particularly regarding survival and rates of hospitalization, are understudied.
Publication bias may also be present given the predominance of early feasibility and single‐arm studies. Additionally, the lack of randomized controlled trials and absence of standardized endpoints restrict generalizability. Long‐term data regarding mortality, rehospitalization, and device durability remain limited.
High statistical heterogeneity (I² > 90%) reflects variability in patient characteristics, device mechanisms, and procedural experience, warranting cautious interpretation. Finally, selective reporting and absence of unpublished negative data could have further influenced pooled estimates.
Conclusion
5
In conclusion, TLVR is emerging as a promising, minimally invasive therapy for ischemic cardiomyopathy, consistently achieving meaningful reverse remodeling and symptomatic improvement throughout all studies. Large multicenter randomized studies need to determine the long‐term durability of these effects and improve patient selection criteria for these devices. Future work should explore its integration within multidisciplinary heart failure management pathways, determine long‐term survival and hospitalization impacts, and refine patient selection based on anatomical and functional criteria.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Figure 1 Supplementary Table: Quality Assessment Using Newcastle‐Ottawa Scale (NOS).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. R. M. J. J. Hegeman , M. J. Swaans , J. P. van Kuijk , and P. Klein , “State‐of‐the‐Art Review: Technical and Imaging Considerations in Hybrid Transcatheter and Minimally Invasive Left Ventricular Reconstruction for Ischemic Heart Failure,” Journal of Clinical Medicine 11, no. 16 (2022): 4831.36013071 10.3390/jcm 11164831 PMC 9409787 · doi ↗ · pubmed ↗
- 2M. Biffi , A. Loforte , G. Folesani , et al., “Hybrid Transcatheter Left Ventricular Reconstruction for the Treatment of Ischemic Cardiomyopathy,” Cardiovascular Diagnosis and Therapy 11, no. 1 (2021): 183–192.33708491 10.21037/cdt-20-265PMC 7944202 · doi ↗ · pubmed ↗
- 3R. R. M. J. J. Hegeman , M. J. Swaans , J. P. Van Kuijk , and P. Klein , “Midterm Outcome of Hybrid Transcatheter and Minimally Invasive Left Ventricular Reconstruction for the Treatment of Ischemic Heart Failure,” Structural Heart 6, no. 5 (2022): 100081.37288056 10.1016/j.shj.2022.100081 PMC 10242554 · doi ↗ · pubmed ↗
- 4N. Hamid , U. P. Jorde , M. Reisman , et al., “Transcatheter Left Ventricular Restoration in Patients With Heart Failure,” Journal of Cardiac Failure 29, no. 7 (2023): 1046–1055.36958391 10.1016/j.cardfail.2023.03.003 · doi ↗ · pubmed ↗
- 5C. Brinza , M. Cinteza , I. V. Popa , and A. Burlacu , “Safety and Efficacy of Less‐Invasive Ventricular Enhancement Procedure With the Transcatheter Revivent TC(TM) System in Patients With Left Ventricular Aneurysm: A Systematic Review,” Reviews in Cardiovascular Medicine 22, no. 2 (2021): 445–452.34258911 10.31083/j.rcm 2202050 · doi ↗ · pubmed ↗
- 6R. H. Jones , E. J. Velazquez , R. E. Michler , et al., “Coronary Bypass Surgery With or Without Surgical Ventricular Reconstruction,” New England Journal of Medicine 360, no. 17 (2009): 1705–1717.19329820 10.1056/NEJ Moa 0900559 PMC 3265934 · doi ↗ · pubmed ↗
- 7J. Naar , I. Skalský , A. Krűger , et al., “Long‐Term Results of Hybrid Left Ventricular Reconstruction in the Treatment of Ischemic Cardiomyopathy,” Journal of Cardiovascular Translational Research 14, no. 6 (2021): 1043–1050.33974231 10.1007/s 12265-021-10133-9PMC 8651588 · doi ↗ · pubmed ↗
- 8P. Klein , S. D. Anker , A. Wechsler , et al., “Less Invasive Ventricular Reconstruction for Ischaemic Heart Failure,” European Journal of Heart Failure 21, no. 12 (2019): 1638–1650.31797492 10.1002/ejhf.1669 · doi ↗ · pubmed ↗