Reframing Food is Medicine as syndemic care: a multidimensional approach to food insecurity
Caroline Elizabeth Owens, David Himmelgreen

TL;DR
This paper suggests using a syndemic approach to address food insecurity and chronic disease by integrating food-based interventions into healthcare.
Contribution
The paper introduces syndemic theory as a novel framework for understanding and addressing food insecurity and chronic disease.
Findings
FIM programs can improve food security and glycemic control.
Mental health may also benefit from these interventions.
Policy changes threaten the effectiveness of syndemic care.
Abstract
Food insecurity and chronic disease are interlinked through systemic disparities in the United States. Building on anthropological and public health scholarship, we argue that syndemic theory offers a valuable framework for analyzing these entangled conditions. A syndemic lens highlights overlapping biological, behavioral, and social mechanisms. Such as chronic stress, inflammation, and coping strategies, that exacerbate disease outcomes in populations experiencing food insecurity, while also pointing toward testable pathways for intervention. In this essay, we explore the potential promise of Food is Medicine (FIM), which includes clinically embedded approaches like medically tailored meals and produce prescriptions, as a form of syndemic care, targeting the co-occurrence of social and health vulnerabilities and risks. Emerging evidence suggests that FIM programs can improve food…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
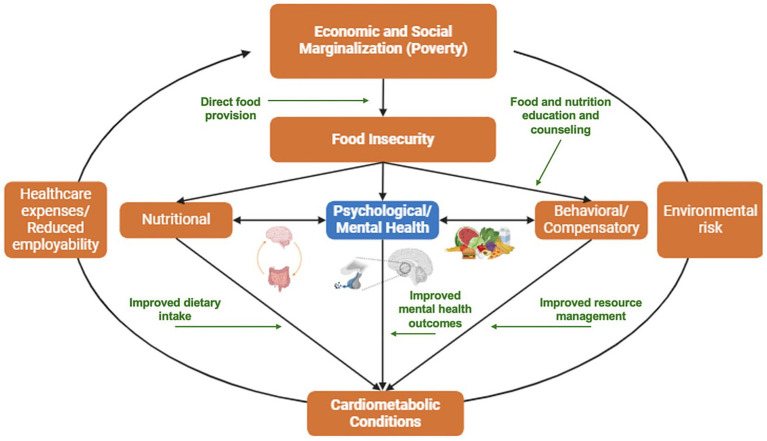 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFood Security and Health in Diverse Populations · Obesity and Health Practices · Child Nutrition and Water Access
Introduction
Over 75% of all adults in the United States live with one or more chronic conditions, many of which are diet-sensitive chronic diseases or conditions. Co- and multimorbidity have become increasingly prevalent, with one in two adults managing multiple, overlapping chronic health conditions (1). These clustered health conditions are patterned by structural and social factors, including county-level economic status (2), systemic discrimination (3, 4), and insecurity related to basic resources like housing, healthcare, and food (5, 6). As a result, food insecurity contributes to the disproportionate prevalence of diet-sensitive diseases among Black or African American, Hispanic/Latinx, American Indian and Alaska Native communities (7), as well as among individuals with lower incomes (8). The recent rise of food insecurity in the United States (9), coupled with policy changes introduced by the One Big Beautiful Bill Act (H.R.1-119th Congress), including cuts to Medicaid and food assistance programs, threatens to deepen existing health disparities, worsen the burden of diet-sensitive chronic disease, and lead to 16,000 extra deaths annually (10).
Food insecurity has wide-ranging consequences for health and wellbeing (5). One well-documented example is its relationship to type 2 diabetes. Compared to people with food security, those experiencing food insecurity are two to three times more likely to have type 2 diabetes and significantly more likely to have poor glycemic control, lower diabetes-specific self-efficacy, and diabetes distress (11–13). In addition to its effects on physical health, food insecurity is robustly associated with adverse mental health conditions, including depression and anxiety (14), which are common comorbidities of diet-related cardiometabolic conditions like type 2 diabetes (15).
Syndemics: the interplay of disease and social disparities
The frequently overlapping constellation of social and economic marginalization, food insecurity, and diet-related chronic diseases has led some scholars to conceptualize these conditions as syndemic phenomena (16, 17). Anthropologist Merrill Singer developed the concept of syndemics, which broadly describes the clustering and synergistic interactions of diseases or health conditions shaped by and exacerbating existing social inequalities (18). Importantly, not all comorbidities meet the criteria for syndemics. Emily Mendenhall identifies three defining features: (1) the co-occurrence of two or more diseases within a specific population; (2) social and contextual factors that are co-constructed and contribute to this co-occurrence; and (3) interactions between diseases that intensify their impact, thereby compounding impacts among affected populations (19).
Building on this framework, Himmelgreen and colleagues argue that food insecurity and diet-related chronic disease constitute a syndemic (17). Himmelgreen et al. suggest that dietary intake, coping strategies, and the biological effects of chronic stress—including dysregulation in cortisol, increased inflammation and the accumulation of visceral fat—interact with the effects of poverty to perpetuate this syndemic. Supporting these proposed biological mechanisms, food insecurity has been associated with biomarkers of inflammation in the US adult population (20). Moreover, both C-reactive protein, an inflammatory biomarker, and cortisol, a stress hormone, have been shown to partially mediate the relationship between household food insecurity and insulin resistance among Latinos with type 2 diabetes (21).
Beyond biological mechanisms, individuals experiencing food insecurity also report coping strategies, such as disordered eating and medication scrimping and non-adherence, that can worsen metabolic outcomes and contribute to emotional distress (22). These findings point to intersecting biological, behavioral, and social pathways, as illustrated in Figure 1, and suggest that interventions grounded in a syndemic framework may be uniquely positioned to disrupt vicious cycles of food insecurity and poor health. However, as Berkowitz, Seligman, and Mozaffarian caution (23), strategies that improve income or food security may enhance certain aspects of health without necessarily improving dietary quality or nutrition security. Similarly, effort focused narrowly on food security or diet may fail to address the broader, systemic drivers of resource insecurity. These considerations underscore the need for holistic, multi-level interventions that address structural drivers of the proposed syndemic.
Proposed syndemic of food insecurity, mental health, and cardiometabolic outcomes, and pathways of Food is Medicine (FIM) impact in green.
Syndemic care: from theory to practice
While syndemic theory has gained traction in public health research as a framework for understanding the interaction of health conditions and structural inequities, its translation into equity-oriented clinical and public health interventions remains nascent. Nonetheless, syndemic thinking offers a promising lens for reimagining care delivery, particularly by emphasizing how chronic stress and systemic disadvantage shape health outcomes and engagement with treatment.
As conceptualized by Dixon and Mendenhall, “syndemic care” applies this framework to clinical practice and policy by emphasizing treatment approaches that addresses co-occurring conditions holistically rather than in isolation (24). Syndemic care expands on integrative or holistic models of medicine by addressing not only shared biological etiologies of disease but the social contexts by which they manifest. This approach moves beyond personal health optimization to encompass the social and environmental dimensions of health. In practice, this means designing interventions that are integrated, contextually aware, and responsive to disadvantage, marginalization, and disenfranchisement. Syndemic care thus requires care teams to understand the lived experiences of patients. In doing so, syndemic care offers a deeper response to the root causes of health than models primarily focused on individual agency or behavior. Existing social determinants of health screening and referral processes are a vital initial step toward moving beyond biomedical reductionism. Realizing the full potential of syndemic care requires clinical systems to connect patients with coordinated, holistic resources—including interventions that address food insecurity and nutrition as central components of health.
Food is Medicine: a model for syndemic care
Bridging the gap between social determinants of health and clinical practice, Food is Medicine (FIM) interventions offer a promising model for operationalizing syndemic care for prevention and treatment. FIM initiatives—a spectrum of food-based, healthcare-integrated interventions that often provide specific types of food and nutrition education and counseling—have gained traction as viable mechanisms for simultaneously improving food security and health outcomes (25). With flexible service options, including medically tailored meals, medically tailored groceries, and produce prescriptions, FIM supports individuals across the lifecourse, from prenatal programs to those for older adults with diet-related conditions, offering a continuum of care that spans prevention through treatment. In addition to addressing food insecurity, FIM interventions are increasingly recognized for their potential to advance health equity, with emerging evidence of positive effects on mental health and overall wellbeing. Systematic reviews and meta-analyses indicate that FIM interventions can improve food security, dietary patterns, and physical health outcomes for patients with diverse chronic conditions, including type 2 diabetes, cardiovascular diseases, HIV, and cancer (25, 26). Focusing on proximate mechanisms, Dixon and Mendenhall identify stress-mediation as a core component of interventions adopting a syndemic care lens (24).
Despite promising early results, many FIM studies have focused on short-term physical health outcomes such as body mass index, HbA1c, and blood pressure. Far fewer have examined effects on mental health or psychosocial stress—key elements of the syndemic framework. However, a growing number of mixed method and qualitative studies of FIM participants have documented changes in psychosocial stress, anxiety, depression, and loneliness (27–30). For example, a randomized trial involving 191 patients with HIV, participants who received 6 months of medically tailored meals had 68% lower odds of experiencing depressive symptoms compared to controls (31). Thus, current evidence demonstrates the significant and multifaceted health consequences of food and nutrition insecurity, positions mental health and psychosocial stress as part of a pathway underlying insecurity and chronic cardiometabolic conditions and shows the promise of FIM as a therapeutic tool for improving wellbeing.
Building on the syndemic framework, FIM interventions may act as critical stress-mediating strategies, aligned with Dixon and Mendenhall’s proposal of syndemic care. Current evidence suggests that FIM interventions can alleviate food and nutrition insecurity, concurrently reducing stressors by improving access to healthy foods, fostering social support, and enhancing self-efficacy in disease management. Biologically, these interventions may disrupt the interconnected physiological pathways whereby chronic stress triggers cortisol dysregulation and systemic inflammation, which in turn exacerbates cardiometabolic disease progression and management.
Figure 1 illustrates the intersecting biological, behavioral, and structural pathways through which food insecurity contributes to syndemic disease—and how interventions like FIM can disrupt these feedback loops. As depicted in Figure 1, FIM can break biological-social linkages by addressing social determinants like economic hardship and limited food access that “get under the skin” to influence mental and physical health. By targeting these intersecting biological and social pathways, FIM serves not only to improve diet and health outcomes but also to potentially disrupt the bidirectional feedback loops that perpetuate syndemic cycles of disadvantage and ill health. Yet, documented experiences of patients receiving FIM often reveal co-occurring social determinants of health, such as housing instability, unreliable transportation, and economic burdens that limit the long-term impact of FIM interventions alone (32). This underscores the importance of considering the broader social and structural conditions in which FIM efforts are embedded.
Reconsidering the social and structural conditions
As promising evidence grows for FIM as a strategy aligned with syndemic care, it becomes increasingly important to situate these interventions within the structural and policy contexts that shape their implementation, effectiveness, and long-term potential. Current funding for FIM initiatives is heterogeneous, encompassing state-specific Medicaid demonstration programs, in lieu of services benefits, select Medicare Advantage plans, and philanthropic support for both research and implementation (33). To date, most interventions are time-limited, ranging from a few weeks to a year or more, but offer demonstrated short-term benefits for health (25). These benefits may also include reduced economic burden of food purchasing, enabling household resources to be saved or spent on other resources. In addition, interventions that provide nutrition and/or culinary education in tandem with provision of food may foster skills related to resource budgeting that may be sustained post-intervention.
Growing evidence from clinical trials and simulation studies suggests that FIM interventions may also be cost-effective for healthcare by reducing utilization and healthcare expenditures. For example, a recent simulation study estimated that medically tailored meal programs could save up to $13.6 billion annually in healthcare costs and prevent 1.6 million hospitalizations among Medicare and Medicaid beneficiaries (34). These findings suggest that the upfront investment in FIM may be offset by downstream savings in healthcare.
However, the sustainability of these improvements may be challenged by persistent economic and environmental barriers, as highlighted in select post-intervention studies, and with shifts in federal and state-level policies related to healthcare and food access (35). While FIM focuses on proximal factors, such as immediate access to nutritious foods, it often does not address the root causes—disparities in income, food environments, discrimination, and opportunity—that drive food insecurity and many health disparities (7, 36). This underscores the opportunity to explore how FIM interventions might be complemented by policies and structural strategies that target these ultimate, root causes. As enthusiasm for FIM grows, it is critical to examine the broader economic, structural, and policy conditions that shape its implementation and sustainability. Without such context, even promising interventions may fall short of achieving their full impact.
Gaps remain in understanding the long-term impacts and sustainability of FIM, especially across diverse and structurally disadvantaged communities. Advancing this work could involve integrating FIM into longer-term health and social care models, aligning with upstream initiatives to improve food environments and economic security. As the field evolves, attention to the contextual conditions that support or hinder the durability of FIM’s impact will be essential to fully realizing its potential as part of a more equitable approach to healthcare.
Critically, efforts to expand reach and impact of FIM risk being undermined by proposed federal policy changes that directly impact foundational funding and access mechanisms supporting FIM. For example, the proposed One Big Beautiful Bill Act includes provisions that would significantly reduce coverage under Medicaid and the Supplemental Nutrition Assistance Program (SNAP). Proposed Medicaid reductions are estimated to result in the loss of health coverage for millions of Americans. These cuts are further compounded by stringent work requirements and more restrictive eligibility criteria, which will make it more challenging to enroll in, and maintain, Medicaid coverage. Given that many FIM initiatives are reimbursed or piloted through Medicaid Section 1115 waivers or managed care organizations, diminished enrollment may translate to reduced program reach and weaker integration between screening and referral within clinical workflows.
In parallel, proposed changes to SNAP coverage, including tightened eligibility thresholds and procedural barriers, are likely to reduce participation. These reductions in access may increase food insecurity and threaten a fundamental food safety-net that currently supports over 40 million people. These policy shifts jeopardize not only the future of FIM, but also the broader landscape of syndemic care models across the United States.
Syndemic solutions: implications for practice and policy
Syndemic theory has the potential to illuminate the ways in which human health is affected by structural and proximate factors that shape our environments and lived experiences, including those with food. As FIM interventions expand, integrating a syndemic lens could enhance efforts to address nutrition and the underlying structural and social contexts in which health inequities develop and persist. Ultimately, addressing syndemics requires collaboration among diverse sectors, including housing, social services, education, urban planning, and food system stakeholders whose policies collectively shape social determinants of health. In the context of shifting federal policies and funding, FIM practitioners may pursue pragmatic, locally grounded strategies that remain viable in the absence federal policy levers. For example, clinics and FIM practitioners might prioritize adapting existing technological infrastructure, such as electronic health records and data sharing systems, to strengthen shared referral platforms and improve care coordination with wraparound services. Technology can also support more holistic lifestyle-based approaches in FIM, as demonstrated by efforts to develop AI-driven smartphone applications (37). Aligning FIM programming with local food access and public health initiatives may enhance program stability by leveraging community-based resources, with braided funding streams serving as a mechanism to meet programmatic needs across sectors. Such integration can incorporate pre-existing efforts such as community gardens, nutrition education, and counseling. Integrated models that link clinical care with social interventions and community development hold promise for disrupting entrenched cycles of disadvantage and poor health. Likewise, engaging youth and younger adults can strengthen efforts toward disease prevention alongside management and treatment. Given nutrition’s profound influence on both biological processes and social determinants, centering food and nutrition security within syndemic-informed interventions is essential to advancing health equity and transforming the root conditions that sustain chronic disease burdens.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Watson KB Wiltz JL Nhim K Kaufmann RB Thomas CW Greenlund KJ. Trends in multiple chronic conditions among US adults, by life stage, behavioral risk factor surveillance system, 2013–2023. Prev Chronic Dis. (2025) 22:22. doi: 10.5888/pcd 22.240539, 40245168 PMC 12007472 · doi ↗ · pubmed ↗
- 2Shaw KM Theis KA Self-Brown S Roblin DW Barker L. Chronic disease disparities by county economic status and metropolitan classification, behavioral risk factor surveillance system, 2013. Prev Chronic Dis. (2016) 13:160088. doi: 10.5888/pcd 13.160088, 27584875 PMC 5008860 · doi ↗ · pubmed ↗
- 3Satia JA. Diet-related disparities: understanding the problem and accelerating solutions. J Am Diet Assoc. (2009) 109:610–5. doi: 10.1016/j.jada.2008.12.019, 19328255 PMC 2729116 · doi ↗ · pubmed ↗
- 4Bailey ZD Krieger N Agénor M Graves J Linos N Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet. (2017) 389:1453–63. doi: 10.1016/S 0140-6736(17)30569-X, 28402827 · doi ↗ · pubmed ↗
- 5Gundersen C Ziliak JP. Food insecurity and health outcomes. Health Aff. (2015) 34:1830–9. doi: 10.1377/hlthaff.2015.0645, 26526240 · doi ↗ · pubmed ↗
- 6Parekh T Xue H Cheskin LJ Cuellar AE. Food insecurity and housing instability as determinants of cardiovascular health outcomes: a systematic review. Nutr Metab Cardiovasc Dis. (2022) 32:1590–608. doi: 10.1016/j.numecd.2022.03.025, 35487828 · doi ↗ · pubmed ↗
- 7Odoms-Young A Bruce MA. Examining the impact of structural racism on food insecurity implications for addressing racial/ethnic disparities. Fam Community Health. (2018) 41:S 3–6. doi: 10.1097/FCH.0000000000000183, 29461310 PMC 5823283 · doi ↗ · pubmed ↗
- 8Rabbitt MP Reed-Jones M Hales LJ Suttles S Burke MP. Household food security in the United States in 2024 (2025). Available online at: www.ers.usda.gov (accessed December 22, 2025).