Comparison of catheter-related bloodstream infection between peripherally inserted central catheters and tunneled central venous catheters in patients receiving home parenteral nutrition: a meta-analysis
Yu-Li Zheng, Ying Wang, Shu-Ping Qi, Wei Zhang, Pei-Yan Lin

TL;DR
This study compares infection risks between two types of catheters used for home nutrition and finds one type has a lower infection risk, though the evidence is weak.
Contribution
A meta-analysis comparing CRBSI rates between PICCs and tunneled CVCs in home parenteral nutrition patients.
Findings
PICCs had a lower CRBSI rate (0.77 per 1,000 days) compared to tunneled CVCs (1.01 per 1,000 days).
The pooled analysis showed PICCs significantly reduced CRBSI risk (RR: 0.40, 95% CI: 0.33–0.49).
Subgroup analyses confirmed consistent results, but evidence quality was very low.
Abstract
Catheter-related bloodstream infection (CRBSI) remains one of the most severe complications in patients receiving home parenteral nutrition. Tunneled central venous catheters (CVCs) and peripherally inserted central catheters (PICCs) are the most commonly used devices for home parenteral nutrition. However, the relative risks of CRBSI from these devices remain controversial. This meta-analysis aimed to compare the incidence of CRBSI between PICCs and tunneled CVCs in patients receiving home parenteral nutrition. A systematic search of PubMed, Embase, and the Cochrane Library databases was conducted from database inception to 3 June 2025 to identify studies comparing the incidence of CRBSI between PICCs and tunneled CVCs in patients receiving home parenteral nutrition. Pooled risk ratios (RRs) with 95% confidence intervals (CIs) were calculated to assess the relative risk of CRBSI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
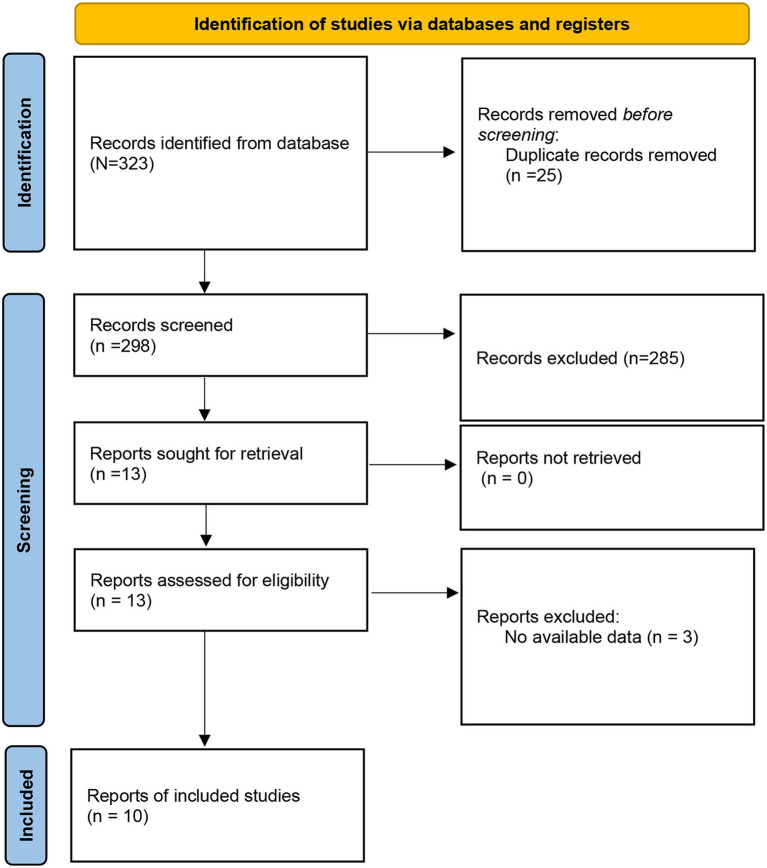 Figure 1
Figure 1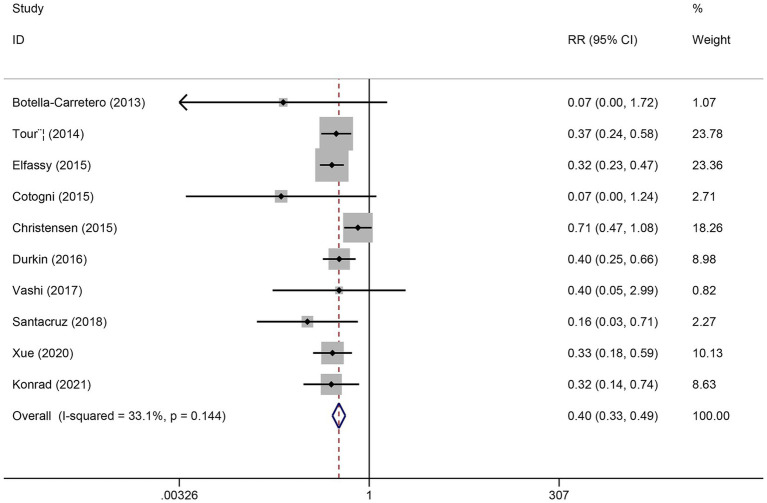 Figure 2
Figure 2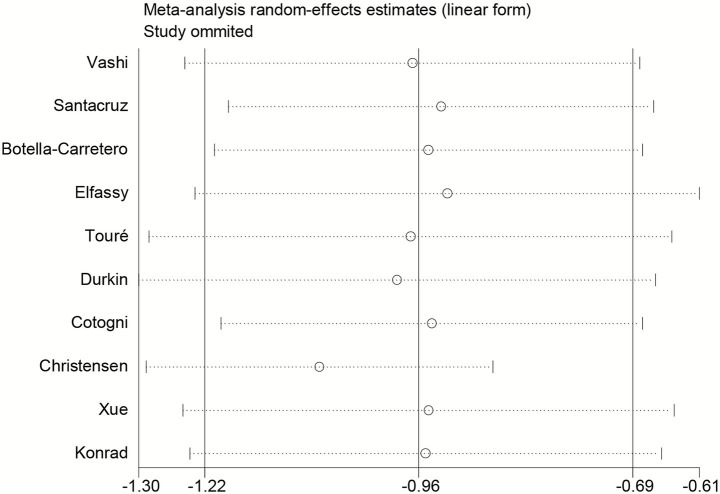 Figure 3
Figure 3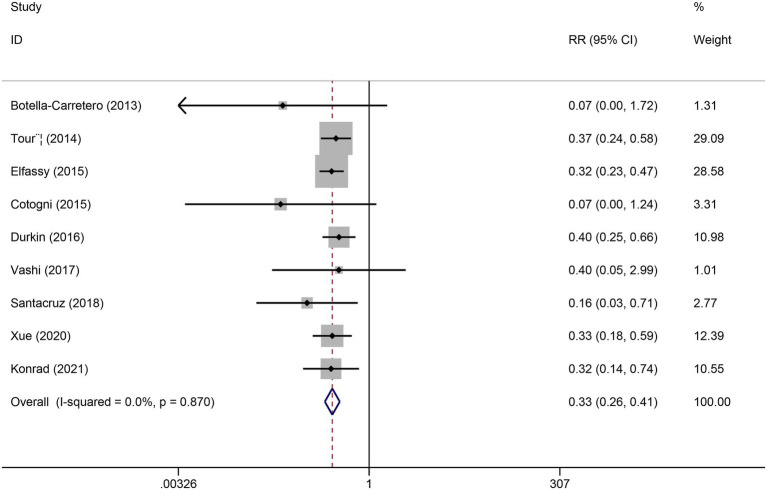 Figure 4
Figure 4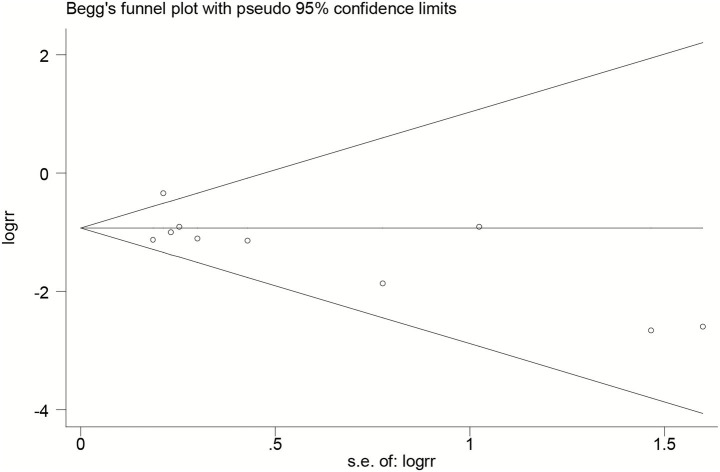 Figure 5
Figure 5| First author | Year | Country | Study design | Mean age | Patient population | CRBSI definition | Method for CRBSI diagnosis | Catheter type | Catheter lumens | Lock solutions | Catheter-days | CRBSI per catheter-days | CRBSI events | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PICC | CVC | PICC | CVC | PICC | CVC | |||||||||||||
| Yes | No | Yes | No | |||||||||||||||
| Vashi | 2017 | USA | Retrospective cohort study | 53.7 | Cancer | IDSA | Blood cultures | PICC, Tunneled | NR | 2% chlorhexidine | – | – | – | – | 7 | 184 | 1 | 10 |
| Santacruz | 2018 | Spain | Prospective cohort study | 58 | Cancer and non-cancer | CDC | Catheter lumen and the blood peripherally cultures | PICC, tunneled | SL:110 | NR | 20,495 | 4,176 | 0.15 | 0.72 | 3 | 113 | 3 | 15 |
| Botella-carretero | 2013 | Spain | Prospective cohort study | 58.46 | Cancer and non-cancer | CDC | Catheter lumen and the blood peripherally cultures | PICC, Hickman | SL:42 | NR | 1,291 | 985 | 0 | 1.02 | 0 | 48 | 1 | 9 |
| Elfassy | 2015 | Canada | Retrospective cohort study | 49.2 | Cancer and non-cancer | No standard criteria | Blood cultures | PICC, Hickman | NR | NR | 18,907 | 18,191 | 1.96 | 1.93 | 37 | 165 | 35 | 27 |
| Touré | 2014 | France | Prospective cohort study | 55.6 | Cancer and non-cancer | CDC | Blood cultures | PICC, Tunneled | NR | NR | 12,322 | 36,812 | 1.38 | 1.82 | 17 | 66 | 67 | 54 |
| Durkin | 2016 | USA | Prospective cohort study | 54 | Cancer and non-cancer | CDC | Blood cultures | PICC, Hickman | NR | NR | – | – | – | – | 20 | 56 | 13 | 7 |
| Cotogni | 2015 | Italy | Prospective cohort study | 67 | Cancer | IDSA | Catheter lumen and the blood peripherally cultures | PICC, Tunneled | All SL | 2% chlorhexidine | 11,504 | 7,835 | 0 | 0.65 | 0 | 65 | 5 | 45 |
| Christensen | 2015 | Denmark | Retrospective cohort study | 64.5 | Cancer and non-cancer | No standard criteria | Blood cultures | PICC, Hickman | NR | NR | 15,974 | 54,912 | 1.63 | 0.56 | 26 | 100 | 49 | 120 |
| Xue | 2020 | USA | Prospective cohort study | 54 | Cancer and non-cancer | CDC | Catheter lumen and the blood peripherally cultures | PICC, Tunneled | SL:18 | NR | – | – | – | – | 14 | 68 | 16 | 15 |
| Konrad | 2021 | Poland | Prospective cohort study | 63.5 | Cancer and non-cancer | No standard criteria | Blood cultures | PICC, Tunneled | All SL | 2% chlorhexidine | 23,045 | 43,789 | 0.3 | 0.41 | 7 | 143 | 18 | 105 |
| First author | Year | Microbiological confirmation |
|---|---|---|
| Vashi | 2017 | |
| Santacruz | 2018 | |
| Botella-Carretero | 2013 | Coagulase-negative |
| Elfassy | 2015 | |
| Touré | 2014 | Coagulase-negative |
| Durkin | 2016 | |
| Cotogni | 2015 | |
| Christensen | 2015 | |
| Xue | 2020 | NR |
| Konrad | 2021 | NR |
| Subgroup | Group | No. studies | Fixed-effects model | Random-effects model | ||
|---|---|---|---|---|---|---|
| RR (95% CI) | RR (95% CI) | |||||
| Country | USA | 3 | 0.37 (0.25, 0.54) | 0.001 | 0.37 (0.26, 0.54) | 0.001 |
| Spain | 2 | 0.13 (0.03, 0.51) | 0.003 | 0.14 (0.03, 0.53) | 0.004 | |
| Canada | 1 | 0.32 (0.23, 0.47) | 0.001 | 0.32 (0.23, 0.47) | 0.001 | |
| France | 1 | 0.37 (0.24, 0.58) | 0.001 | 0.37 (0.24, 0.58) | 0.001 | |
| Italy | 1 | 0.07 (0.00, 1.24) | 0.070 | 0.07 (0.00, 1.24) | 0.070 | |
| Denmark | 1 | 0.71 (0.47, 1.08) | 0.109 | 0.71 (0.47, 1.08) | 0.109 | |
| Poland | 1 | 0.32 (0.14, 0.74) | 0.008 | 0.32 (0.14, 0.74) | 0.008 | |
| Design | Prospective cohort | 7 | 0.33 (0.25, 0.44) | 0.001 | 0.47 (0.24, 0.93) | 0.030 |
| Retrospective cohort | 3 | 0.49 (0.38, 0.65) | 0.001 | 0.35 (0.27, 0.45) | 0.001 | |
| Population | Cancer | 2 | 0.15 (0.03, 0.81) | 0.028 | 0.21 (0.03, 1.37) | 0.105 |
| Non-cancer | 8 | 0.41 (0.34, 0.50) | 0.001 | 0.39 (0.30, 0.51) | 0.001 | |
| CRBSI definition | IDSA | 2 | 0.15 (0.03, 0.81) | 0.028 | 0.22 (0.03, 1.38) | 0.105 |
| CDC | 5 | 0.35 (0.26, 0.47) | 0.001 | 0.36 (0.27, 0.47) | 0.001 | |
| No standard criteria | 3 | 0.46 (0.36, 0.60) | 0.001 | 0.43 (0.24, 0.78) | 0.001 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Clinical Nutrition and Gastroenterology · Dialysis and Renal Disease Management
Introduction
Home parenteral nutrition is a life-sustaining therapy for patients with chronic intestinal failure or severe diseases who are unable to maintain adequate nutritional intake via oral or enteral routes (1, 2). Central venous access is indispensable for home parenteral nutrition, as it enables the long-term administration of nutrient solutions (3, 4). However, catheter-related bloodstream infection (CRBSI) remains the most frequent and serious complication associated with central venous access (5). CRBSI not only increases morbidity and hospital readmission rates but also imposes a substantial economic burden on patients and healthcare systems (6, 7).
In recent years, peripherally inserted central catheters (PICCs) have been increasingly adopted because of their relative ease of insertion, cost-effectiveness, and suitability for long-term use (8). Nevertheless, the risk of CRBSI associated with PICCs compared with conventional central venous catheters (CVCs) remains controversial (9, 10). Some observational studies have suggested that PICCs may be associated with similar or even higher infection rates than tunneled CVCs, while other studies have reported a lower risk of CRBSI with PICCs than with tunneled CVCs (11–14). These inconsistencies highlight the need for a systematic evaluation to clarify the relative risk between PICCs and tunneled CVCs in patients receiving home parenteral nutrition. Therefore, this study aimed to conduct a comprehensive meta-analysis to compare the incidence of CRBSI between PICCs and tunneled CVCs in patients receiving home parenteral nutrition. By synthesizing the available evidence, we aimed to generate more reliable data to inform clinical practice.
Methods
Literature search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was used to conduct this systematic review and meta-analysis (15). The study protocol was registered on INPLASY (Registration number: INPLASY2025120072). A systematic literature search was conducted in PubMed, Embase, and the Cochrane Library databases from their inception to 3 June 2025. The search terms included combinations of the following keywords and Medical Subject Headings (MeSH): “peripherally inserted central catheter,” “PICCs,” “central venous catheter,” “CVCs,” and “home parenteral nutrition.” The detailed search strategy was described in Supplementary Table S1. The search was restricted to studies published in English. Reference lists of relevant articles and reviews were also manually screened to identify additional eligible studies.
Inclusion and exclusion criteria
Studies that met the following criteria according to the PICOS guidelines were included: Patients: adult patients (≥18 years) receiving home parenteral nutrition; Intervention and comparison: peripherally inserted central catheters versus tunneled central venous catheters; Outcomes: the incidence of CRBSI; and Study design: cohort or case–control studies. Articles were excluded if they lacked eligible data or were case reports, reviews, or conference abstracts.
Data extraction and quality assessment
All eligible data were independently extracted by two investigators using a standardized data extraction form. Any discrepancies were resolved through discussion, and if consensus could not be reached, a third investigator was consulted. Data extracted included the first author, year of publication, country, study design, treatment regimen, outcome measures, and definition of CRBSI. The methodological quality of the included studies was independently assessed by two reviewers using the Newcastle–Ottawa Scale (NOS) (16). Studies with an accumulated score of ≥6 points were considered high quality. The certainty of evidence and strength of recommendations were evaluated using the GRADE approach (17), which rates confidence in summary effect estimates across four levels: very low, low, moderate, and high.
Statistical analysis
Stata 12.0 (STATA Corp, College Station, TX, USA) was used for the meta-analysis. Pooled risk ratios (RRs) with 95% confidence intervals (CIs) were calculated to estimate the incidence of CRBSI using either the fixed-effects model or random-effects model, depending on the degree of heterogeneity. Heterogeneity was assessed using Cochran’s Q test and quantified with the I^2^ statistic, with I^2^ > 50% considered substantial. Sensitivity analysis was conducted by sequentially removing individual studies to assess the robustness of the results. Subgroup analyses were conducted based on available variables. Publication bias was evaluated using funnel plots, Egger’s regression test, and Begg’s test.
Results
Literature selection
A total of 323 studies were initially retrieved from the databases. After removal of duplicates and screening titles and abstracts, 13 articles were retained for full-text review. Of these, three studies were excluded due to unavailable or insufficient data. Finally, 10 studies (11–15, 18–22) met the inclusion criteria for the meta-analysis. The study selection process is presented in the PRISMA flow diagram (Figure 1). The included 10 studies, published between 2013 and 2021, involved a total of 1,139 patients receiving PICCs, with sample sizes ranging from 48 to 202 participants. The studies were conducted between 2013 and 2021 across multiple countries, including the USA, Spain, Canada, France, Italy, Denmark, and Poland. Both prospective and retrospective cohort designs were represented, with patient populations including both cancer and non-cancer patients. CRBSI definitions varied among studies: the Infectious Diseases Society of America (IDSA) criteria were used in two studies, the CDC criteria in five studies, and no standard criteria were reported in three studies. CRBSI was generally diagnosed based on blood cultures or catheter lumen cultures, with slight differences depending on the study protocol. Catheter types included PICCs and tunneled CVCs. The number of lumens, catheter-days, and CRBSI rates per 1,000 catheter-days were reported when available (Table 1). The microorganisms responsible for catheter-associated infections are primarily Gram-positive bacteria, Gram-negative pathogens, and fungi (Table 2). The quality of the included literature was scored 6–7 (Supplementary Table 2).
Flow diagram of literature search.
Meta-analysis of CRBSI
Ten studies reported the effects of PICCs and tunneled CVCs on the incidence of CRBSI based on per-patient risk. Moderate heterogeneity was observed among the included studies (I^2^ = 33.1%, p = 0.14). Therefore, both fixed-effects and random-effects models were applied. Under both models, PICC use was associated with a significantly lower risk of CRBSI compared with tunneled CVCs (fixed-effects model: RR = 0.40, 95% CI 0.33–0.49; random-effects model: RR = 0.38, 95% CI 0.29–0.50; both p < 0.001) (Figure 2). According to GRADE, the quality of evidence was very low (Supplementary Table 3). In addition, seven studies reported CRBSI incidence based on per 1,000 catheter-days. The mean CRBSI rate was 0.77 per 1,000 PICC-days (range: 0.00–1.96 per 1,000 PICC-days) and 1.01 per 1,000 tunneled CVC-days (range: 0.41–1.93 per 1,000 tunneled CVC-days), indicating a consistently lower incidence associated with PICCs.
Forest plot for the incidence of CRBSI between PICCs and tunneled CVCs groups.
Subgroup analysis by country showed consistent results across most regions, including the USA, Spain, Canada, France, and Denmark, with no significant differences between PICCs and tunneled CVCs. In contrast, Italy and Poland did not demonstrate a statistically significant difference between the two catheter types. Subgroup analyses stratified by study design demonstrated that both prospective cohort and retrospective cohort studies found a significant difference between PICCs and tunneled CVCs, with PICC use being associated with a lower risk of CRBSI. When stratified by patient population, the association between catheter type and CRBSI risk remained consistent in both cancer and non-cancer populations. Moreover, subgroup analyses stratified by CRBSI definition demonstrated that studies using IDSA criteria, CDC criteria, and those applying non-standard clinical definitions all showed a statistically significant difference between PICCs and tunneled CVCs, with PICC use consistently associated with a lower risk of CRBSI (Table 3).
Sensitivity analysis
Sensitivity analysis was performed by sequentially excluding each study (Figure 3). After excluding the study by Christensen et al., heterogeneity was eliminated (I^2^ decreased from 33.1 to 0%). The pooled effect estimate remained stable, with PICCs still associated with a significantly lower risk of CRBSI compared with tunneled CVCs (RR = 0.33, 95% CI 0.26–0.41), indicating the robustness of the overall findings (Figure 4).
Sensitivity analysis for CRBSI risk.
Forest plot of the incidence of CRBSI comparing PICCs and tunneled CVCs after removal of one study.
Publication bias
Publication bias was evaluated using funnel plots and Begg’s test. Visual inspection of the funnel plot revealed no significant asymmetry (Figure 5). Both Egger’s test (p = 0.138) and Begg’s test (p = 0.421) indicated no significant publication bias.
Begg’s funnel plot for publication bias.
Discussion
The choice between PICCs and tunneled CVCs for home parenteral nutrition remains a subject of an important clinical debate. This controversy arises from differences in complication risks, patient comfort, and cost-effectiveness. Therefore, determining which catheter insertion method provides superior outcomes is of critical importance. In this meta-analysis, we found that PICCs may be associated with a lower risk of CRBSI compared with tunneled CVCs in patients receiving home parenteral nutrition.
The observed lower risk of CRBSI associated with PICCs may be explained by several plausible reasons. First, peripheral insertion may reduce the risk of procedural contamination because the puncture site is more accessible and easier to maintain aseptically (23, 24). Second, PICC placement is generally less invasive and often performed at the bedside using ultrasound guidance, which has been associated with fewer insertion-related complications and shorter procedure times—factors that may reduce infection risk (25, 26). In addition, catheter design characteristics may contribute to differences in CRBSI risk. PICCs used for home parenteral nutrition are more frequently single lumen and of smaller diameter, features that have been associated with lower rates of intraluminal colonization (27, 28). However, tunneled CVCs are more frequently selected for patients with greater disease severity, poor peripheral venous access, or anticipated prolonged or complex therapy (29, 30). As a majority of the included studies were observational and lacked adjustment for illness severity, catheter indication, and functional status, residual confounding cannot be excluded.
Our findings are largely consistent with previous observational studies reporting a lower incidence of CRBSI with PICCs than with tunneled CVCs, particularly in home-based care or long-term use scenarios (11, 13, 21). Multiple prospective cohort studies have shown that PICCs are associated with fewer infectious complications, shorter catheter dwell-related morbidity, and lower hospitalization rates (14, 18, 19, 22). In contrast, studies conducted in hospital settings sometimes reported minimal differences, suggesting that contextual factors, such as infection prevention training, institutional protocols, and healthcare personnel expertise, may influence the observed outcomes (31). These comparisons underscore that, while catheter selection is important, strict adherence to infection control measures remains essential. Notably, the diagnosis of CRBSI varied across the included studies. CRBSI is defined according to established criteria, such as those proposed by the Centers for Disease Control and Prevention (CDC) (32) or the Infectious Diseases Society of America (IDSA) (33). However, several studies relied on less stringent definitions, such as positive blood cultures without standardized confirmation methods (18, 19, 21). This inconsistency in diagnostic criteria may have contributed to heterogeneity in the pooled estimates and should be considered when interpreting the results.
Despite the important insights provided by our study, several limitations should be considered. First, a majority of the included studies were observational, introducing the potential for selection bias and residual confounding. Second, substantial heterogeneity existed across studies in CRBSI definitions, diagnostic criteria, and surveillance methods, which may have influenced the pooled estimates. Third, the majority of studies lacked detailed reporting of catheter-related variables, including catheter dwell time, the number of lumens, comorbidities, or concurrent medications, all of which can affect infection risk. Finally, the lack of high-quality randomized controlled trials limits the generalizability of our conclusions, particularly across diverse healthcare settings and populations with different home care practices. Importantly, when assessed using the GRADE framework, the overall certainty of evidence for the CRBSI was very low, due to the risk of bias, inconsistency, and imprecision.
Although the results of this meta-analysis indicate that PICCs may be associated with a lower risk of CRBSI compared with tunneled CVCs in patients receiving home parenteral nutrition, the available studies are observational, carrying a substantial risk of bias and residual confounding, which led to a very low certainty of evidence. High-quality, well-designed randomized controlled trials with standardized CRBSI definitions and comprehensive reporting of catheter-related variables are urgently needed to confirm these findings and to inform optimal vascular access strategies in home parenteral nutrition care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bering J Di Baise JK. Home parenteral and enteral nutrition. Nutrients. (2022) 14:2558. doi: 10.3390/nu 14132558, 35807740 PMC 9268549 · doi ↗ · pubmed ↗
- 2Pironi L Boeykens K Bozzetti F Joly F Klek S Lal S . ESPEN guideline on home parenteral nutrition. Clin Nutr. (2020) 39:1645–66. doi: 10.1016/j.clnu.2020.03.005, 32359933 · doi ↗ · pubmed ↗
- 3Kovacevich DS Corrigan M Ross VM Mc Keever L Hall AM Braunschweig C. American society for parenteral and enteral nutrition guidelines for the selection and care of central venous access devices for adult home parenteral nutrition administration. JPEN J Parenter Enteral Nutr. (2019) 43:15–31. doi: 10.1002/jpen.1455, 30339287 · doi ↗ · pubmed ↗
- 4Salonen BR Bonnes SL Mundi MS Lal S. Repair of central venous catheters in home parenteral nutrition patients. Nutr Clin Pract. (2019) 34:210–5. doi: 10.1002/ncp.1026230729597 · doi ↗ · pubmed ↗
- 5Wong LP. Practical strategies for prevention of catheter-related bloodstream infections (CRBSI) in United States hemodialysis facilities. Hemodial Int. (2025) 30:10–17. doi: 10.1111/hdi.70005, 40582986 · doi ↗ · pubmed ↗
- 6Iorga A Velezis MJ Marinac-Dabic D Lario RF Huff SM Gore B . Venous access: national guideline and registry development (VANGUARD): advancing patient-centered venous access care through the development of a national coordinated registry network. J Med Internet Res. (2023) 25:e 43658. doi: 10.2196/43658, 37999957 PMC 10709786 · doi ↗ · pubmed ↗
- 7Scaglione G Colaneri M Offer M Galli L Borgonovo F Genovese C . Epidemiology and clinical insights of catheter-related Candidemia in non-ICU patients with vascular access devices. Microorganisms. (2024) 12:1597. doi: 10.3390/microorganisms 12081597, 39203438 PMC 11356456 · doi ↗ · pubmed ↗
- 8Frondizi F Dolcetti L Pittiruti M Calabrese M Fantoni M Biasucci DG . Complications associated with the use of peripherally inserted central catheters and midline catheters in COVID-19 patients: an observational prospective study. Am J Infect Control. (2023) 51:1208–12. doi: 10.1016/j.ajic.2023.05.002, 37160191 PMC 10164288 · doi ↗ · pubmed ↗