A broad-range polymerase chain reaction on a formalin-fixed, paraffin-embedded tissue is a powerful diagnostic tool, but requires cautious interpretation: a case report
Paddy Ssentongo, Tonya Crook, Rezhan Hussein

TL;DR
A case report shows how a diagnostic test on preserved tissue can be misleading and highlights the need for careful interpretation in clinical settings.
Contribution
Demonstrates the potential pitfalls of using broad-range PCR on FFPE tissue for diagnosing infections in a clinical context.
Findings
BRPCR on FFPE tissue detected normal oral flora DNA but missed the actual carcinoma.
The case highlights the risk of misinterpreting BRPCR results in non-sterile FFPE samples.
Proper clinical correlation is essential when using BRPCR in complex diagnostic scenarios.
Abstract
A woman in her mid-50s with Lynch syndrome and a history of malignant neoplasms was found to have a superior vena cava (SVC) thrombus and a necrotic mediastinal mass on surveillance imaging. The initial biopsy yielded necrotic debris, and the procedure was complicated by a mediastinal hematoma. Due to concern for possible infection, the patient was empirically treated with antibiotics while planning further workup. A broad-range 16S polymerase chain reaction (BRPCR) was performed on a formalin-fixed paraffin-embedded (FFPE) tissue, which was negative for fungi and mycobacteria but revealed DNA from normal oral flora. Subsequently, she developed SVC syndrome, raising concern about a mediastinal abscess. A repeated biopsy confirmed the suspected carcinoma with necrosis. This case underscores the importance of proper interpretation of BRPCR results in FFPE (non-sterile) tissue and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
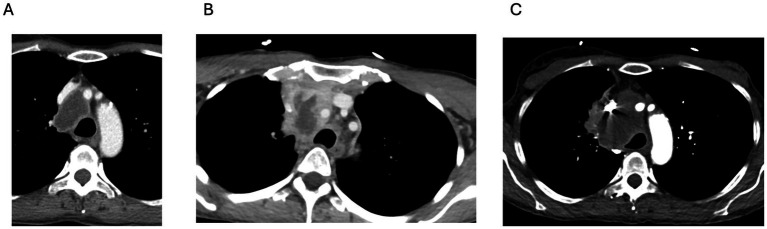 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Otolaryngology and Infectious Diseases · Infective Endocarditis Diagnosis and Management
Highlights
- BRPCR on FFPE tissues is vulnerable to contamination and degradation.
- Clinical correlation and appropriate context are essential when ordering or interpreting BRPCR results.
- Fresh tissue collected in a sterile container during the biopsy procedure is preferred for molecular diagnostics when infection is suspected.
Background
Broad-range 16S polymerase chain reaction (BRPCR) has emerged as a powerful diagnostic tool in culture-negative infections, offering the ability to identify fastidious, slow-growing, or non-viable organisms through amplification of conserved ribosomal gene sequences (1). When used on fresh, sterile tissue, BRPCR can expedite the diagnosis and guide targeted antimicrobial therapy in complex or atypical presentations. Its utility has been documented across a range of clinical scenarios, including prosthetic joint infections, endocarditis, and central nervous system infections, where standard cultures often fail to yield results (2). The technique’s strength lies in its broad scope and sensitivity, allowing the detection of diverse microbial taxa from small or degraded samples, and it has become an increasingly common adjunct in the diagnostic evaluation of suspected infections, particularly when conventional methods are ineffective.
BRPCR amplifies conserved genetic regions, such as the bacterial 16S rRNA gene, the fungal internal transcribed spacer (ITS) regions, and, for acid-fast bacilli, including nontuberculous mycobacteria and the Mycobacterium tuberculosis complex, targets such as the 16S rRNA gene, rpoB, and hsp65 to detect a wide range of organisms directly from clinical specimens without the need for culture (3, 4). Sequencing the amplified product and comparing it with reference databases enables organism identification, including fastidious or nonviable pathogens (4).
However, BRPCR has notable limitations, particularly when applied to formalin-fixed paraffin-embedded (FFPE) tissues (5–8). The fixation and embedding process chemically alters nucleic acids, introducing fragmentation and cross-linking that impair amplification fidelity. In necrotic or non-sterile specimens, background DNA from environmental, commensal, or oral flora may be inadvertently amplified, resulting in misleading or false-positive findings. Contamination introduced during tissue processing, DNA extraction, or polymerase chain reaction (PCR) setup can further confound interpretation. These vulnerabilities are especially relevant when BRPCR is ordered on tissue that was not collected for microbiological evaluation and was not handled sterily. The case presented here illustrates how a BRPCR performed on a necrotic FFPE tissue risked misdirecting attention from a non-infectious etiology—an adenocarcinoma masquerading as a mediastinal infection.
Case presentation
A woman in her mid-50s with Lynch syndrome was found to have a well-circumscribed, 4.0 × 2.4 cm anterior mediastinal mass with central necrosis and peripheral enhancement, which was compressing the proximal superior vena cava (SVC) on routine surveillance computed tomography (CT) of the chest (Figure 1A). She also had an SVC thrombus. Her past medical history included invasive ductal breast carcinoma (diagnosed and treated with mastectomy and adjuvant chemotherapy 9 years prior) and resection of an intestinal neuroendocrine tumor 6 months before presentation. She was anticoagulated and referred to interventional pulmonology for a biopsy and underwent endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA). Biopsy material was collected for cytologic evaluation and routine cultures. Processing into FFPE blocks occurred according to the routine diagnostic protocol. Pathology from the initial biopsy revealed only necrotic debris with no evidence of malignancy. Twelve days after the EBUS procedure, she developed new neck pain and a bulge along the right side of her neck and presented to the emergency room.
Progressive enlargement of an anterior mediastinal mass over time. (A) CT scan of the chest at presentation showing a 4.0 × 2.4 cm centrally necrotic mass in the middle mediastinum with smooth peripheral enhancement and associated SVC involvement and thrombus. (B) CT scan of the chest taken approximately 3 weeks later, demonstrating interval enlargement of the lesion with increased peripheral enhancement and a new extension into the anterior mediastinum, involving the left brachiocephalic vein. (C) CT scan of the chest taken approximately 8 weeks after the initial presentation, showing further progression with an increase in size to 6.3 × 3.7 cm and possible adjacent lung involvement.
Upon admission, she was afebrile and hemodynamically stable. Laboratory tests showed a white blood cell count of 9.8 × 10^9^/L (normal range: 4.0–10.0 × 10^9^/L), hemoglobin level of 12.3 g/dL (normal range: 12–16 g/dL), platelet count of 198 × 10^9^/L (normal range: 150–400 × 10^9^/L), ESR of 32 mm/h (normal range: 0–15 mm/h), and C-reactive protein level of 2.6 mg/dL (normal range: <0.5 mg/dL). A repeat contrast-enhanced chest CT scan revealed an enlarging necrotic mediastinal mass with mass effect on the SVC (Figure 1B) and left brachiocephalic vein (unchanged from prior), and a new complex, low-attenuation fluid collection measuring up to 4.5 cm in the anterior superior mediastinum, thought to be a hematoma given the recent biopsy. The treating team was concerned about a necrotizing infectious process, prompting an infectious diseases (ID) consultation. The ID examination included blood cultures, urine for Histoplasma and Blastomyces antigens, a serum cryptococcal antigen test, a Quantiferon TB-Gold test, an Aspergillus galactomannan antigen test, Bartonella serology, and BRPCR for fungi, mycobacteria, and bacteria (to look for Nocardia species, in particular) was requested to be added to the FFPE specimen as there were no fresh samples to test.
Blood cultures and antigen/serology testing were negative during the hospitalization. However, a computerized tomography Panorex showed a chronic mandibular dental infection, raising concern about the extension of an odontogenic infection via the fascial planes into the mediastinum. The patient was empirically treated with ampicillin-sulbactam IV while hospitalized and discharged on amoxicillin-clavulanate with close outpatient follow-up with pulmonary service. Subsequently, BRPCR was reported to be negative for fungi and mycobacteria but positive for the DNA of Streptococcus mitis, Streptococcus parasanguinis, Veillonella atypica, and Streptococcus raffinosus. Since fungi, mycobacteria and nocardia were not detected, she was continued on amoxicillin-clavulanate and advised to undertake further evaluation and proceed with a planned positron emission tomography (PET) scan.
She returned within 8 weeks to the emergency department with progressive dyspnea and worsening right-sided neck swelling. A repeated chest CT scan revealed enlargement of the mediastinal mass (now 6.3 × 3.7 cm) with SVC and inferior vena cava (IVC) invasion (Figure 1C). Heavily influenced by the BRPCR results, the treating teams consulted the ID service again, expressing concern about a mediastinal abscess.
However, the ID service cautioned against a diagnosis of a mediastinal abscess, noting that the BRPCR results could be misleading. They recommended proceeding with a repeat tissue biopsy to obtain a larger sample. A tissue biopsy obtained by CT guidance showed carcinoma with necrosis. Immunostaining was CK7-positive and GATA3/TTF-1/SOX10-negative, indicating a gastrointestinal origin.
Treatment and follow-up
The patient remained under oncologic care, received chemotherapy, and underwent further evaluation for additional metastatic lesions.
Discussion
BRPCR has emerged as a useful diagnostic tool for identifying pathogens in culture-negative infections. However, its application to formalin-fixed, paraffin-embedded (FFPE) tissues presents several technical and interpretive challenges. DNA extracted from FFPE specimens is often fragmented and chemically modified due to formalin fixation, reducing amplification fidelity and increasing the likelihood of non-specific or background signals. These limitations are particularly problematic in necrotic or non-sterile tissues, where the distinction between true infection and environmental or commensal contamination becomes blurred (5, 6).
In this case, the detection of DNA from the Streptococcus mitis group, Veillonella atypica, and other oral flora in a necrotic mediastinal mass led the treating team to consider diagnosing a mediastinal abscess when the patient presented again to the hospital; however, the ID team cautioned against this conclusion and emphasized the importance of repeating a tissue biopsy due to concerns about malignancy. This highlights how molecular results can disproportionately influence decision-making when they are not interpreted within the full clinical context.
Recent literature has reinforced the challenges associated with molecular diagnostics applied to FFPE samples (9–12). Multiple studies highlight that contamination, nucleic acid degradation, and the inability to quantify microbial load substantially limit the clinical specificity of BRPCR in FFPE tissue. Proposed refinements, such as quantitative PCR, metagenomic sequencing, and multiplex molecular panels, may offer improved resolution, although their performance in necrotic or non-sterile tissue remains uncertain (11, 12). These observations underscore the need to interpret FFPE-derived molecular results with caution and always in conjunction with clinical and radiologic data.
A holistic approach that integrates clinical context, radiologic features, histopathology, and microbiology is essential to avoiding premature or inaccurate conclusions (8). Fresh, unfixed, or frozen samples collected in a sterile container, if possible, are preferred for molecular diagnostics to guide antimicrobial therapy, and we urge the cautious interpretation of BRPCR (especially on fixed tissues) if an infectious etiology is not highly suspected, and the use of the results in the proper context.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sontakke S Cadenas MB Maggi RG Diniz PPV Breitschwerdt EB. Use of broad range 16S r DNA PCR in clinical microbiology. J Microbiol Methods. (2009) 76:217–25. doi: 10.1016/j.mimet.2008.11.002, 19046999 · doi ↗ · pubmed ↗
- 2Akram A Maley M Gosbell I Nguyen T Chavada R. Utility of 16S r RNA PCR performed on clinical specimens in patient management. Int J Infect Dis. (2017) 57:144–9. doi: 10.1016/j.ijid.2017.02.006, 28216180 · doi ↗ · pubmed ↗
- 3Rakeman JL Bui U La Fe K Chen Y-C Honeycutt RJ Cookson BT. Multilocus DNA sequence comparisons rapidly identify pathogenic molds. J Clin Microbiol. (2005) 43:3324–33. doi: 10.1128/JCM.43.7.3324-3333.2005, 16000456 PMC 1169180 · doi ↗ · pubmed ↗
- 4Putnam NE Charles DW Doub JB Johnson JK. Broad-range polymerase chain reaction and sequencing for the diagnosis of infectious diseases. Microbiol Spectr. (2025) 13:e 02505-24. doi: 10.1128/spectrum.02505-24, 40042284 PMC 11960090 · doi ↗ · pubmed ↗
- 5Janda JM Abbott SL. 16S r RNA gene sequencing for bacterial identification in the diagnostic laboratory: pluses, perils, and pitfalls. J Clin Microbiol. (2007) 45:2761–4. doi: 10.1128/JCM.01228-07, 17626177 PMC 2045242 · doi ↗ · pubmed ↗
- 6Rampini SK Bloemberg GV Keller PM Büchler AC Dollenmaier G Speck RF . Broad-range 16S r RNA gene polymerase chain reaction for diagnosis of culture-negative bacterial infections. Clin Infect Dis. (2011) 53:1245–51. doi: 10.1093/cid/cir 692, 21976460 · doi ↗ · pubmed ↗
- 7Corless CE Guiver M Borrow R Edwards-Jones V Kaczmarski EB Fox AJ. Contamination and sensitivity issues with a real-time universal 16S r RNA PCR. J Clin Microbiol. (2000) 38:1747–52. doi: 10.1128/JCM.38.5.1747-1752.2000, 10790092 PMC 86577 · doi ↗ · pubmed ↗
- 8Lehmann U Kreipe H. Real-time PCR analysis of DNA and RNA extracted from formalin-fixed and paraffin-embedded biopsies. Methods. (2001) 25:409–18. doi: 10.1006/meth.2001.1263, 11846610 · doi ↗ · pubmed ↗