Emergency cancer diagnosis in older adults: patterns, subgroups, and implications for health-care quality metrics
Sarah E Soppe, Sharon Peacock Hinton, Ellis C Dillon, Sandi L Pruitt, Georgios Lyratzopoulos, Matthew E Barclay, Megan A Mullins, Allison W Kurian, Nicholas Pettit, Matthew Thompson, Caroline A Thompson

TL;DR
This study examines how older adults in the US are diagnosed with cancer in emergency settings and identifies patterns that suggest barriers to timely care.
Contribution
The study introduces a novel classification of emergency cancer diagnoses based on hospitalization status to better understand care barriers.
Findings
38% of older cancer patients were diagnosed through emergency presentations, with 80% requiring hospitalization.
Outpatient emergency presentations were more common in younger, rural patients with localized cancers.
Emergency presentations had less nonemergency care for symptoms and more prediagnostic emergency care.
Abstract
Cancer diagnosis originating in emergency departments (emergency presentation) contributes to poorer cancer survival and reflects aggressive disease and limited access to routine health care. This study characterized emergency presentations for a range of cancers and subclassified by whether patients were hospitalized after the emergency encounter, with the hypothesis that, compared with those hospitalized, patients not requiring hospitalization more specifically represent barriers to timely and adequate care. We analyzed Surveillance, Epidemiology, and End Results–Medicare data for patients aged 66 years and older diagnosed with 14 cancer types (2008-2017; n = 614 885). We described emergency presentation overall and demographic and clinical characteristics across subgroups using linear regression and assessed differences in health-care utilization before the emergency presentation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
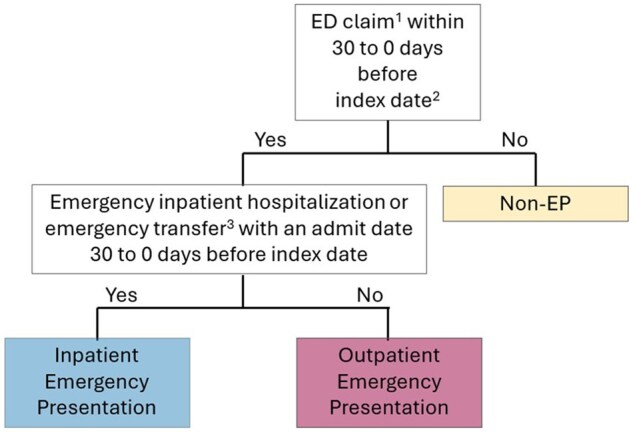 Figure 1
Figure 1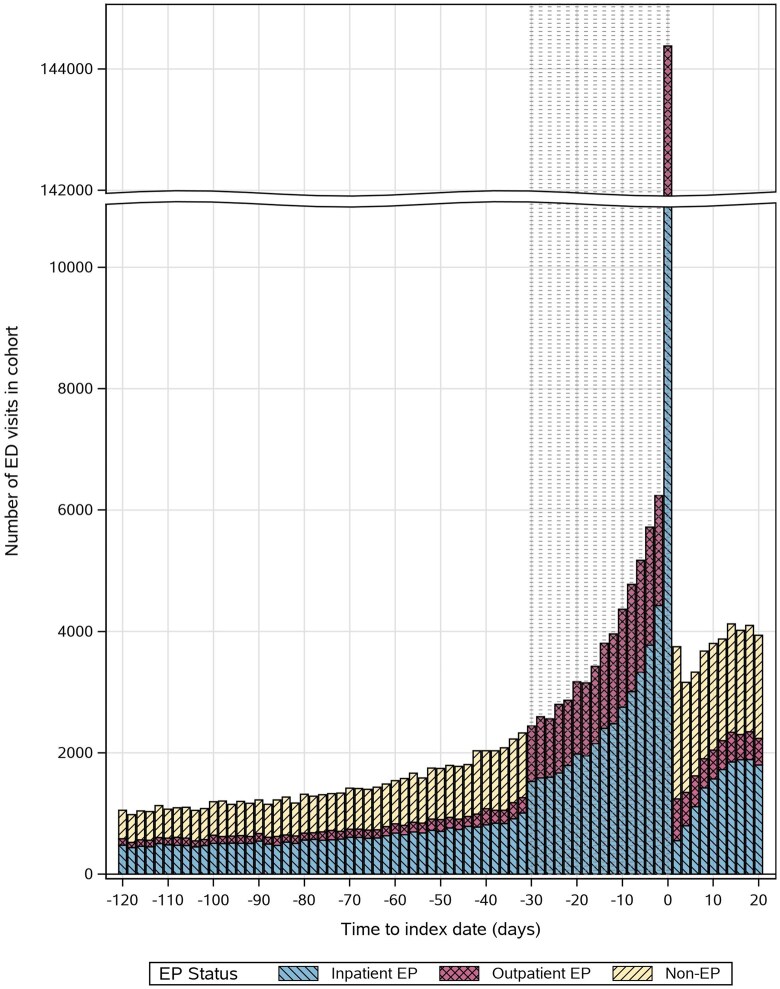 Figure 2
Figure 2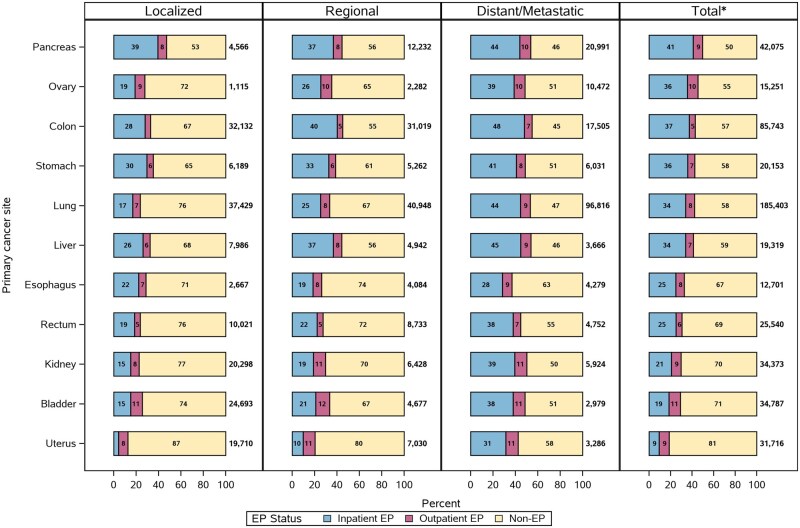 Figure 3
Figure 3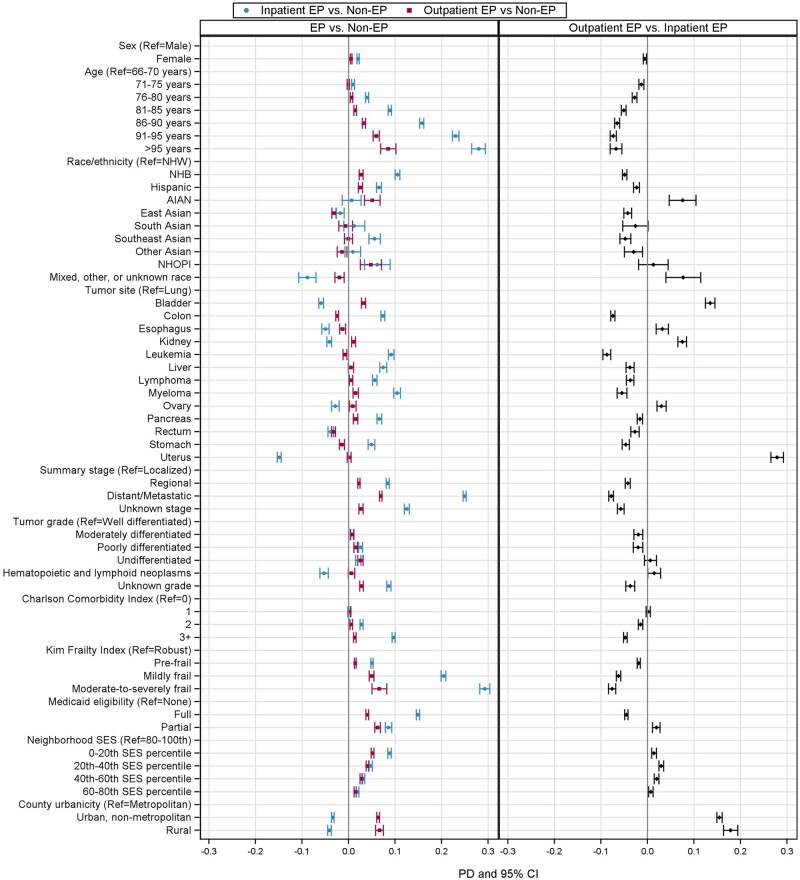 Figure 4
Figure 4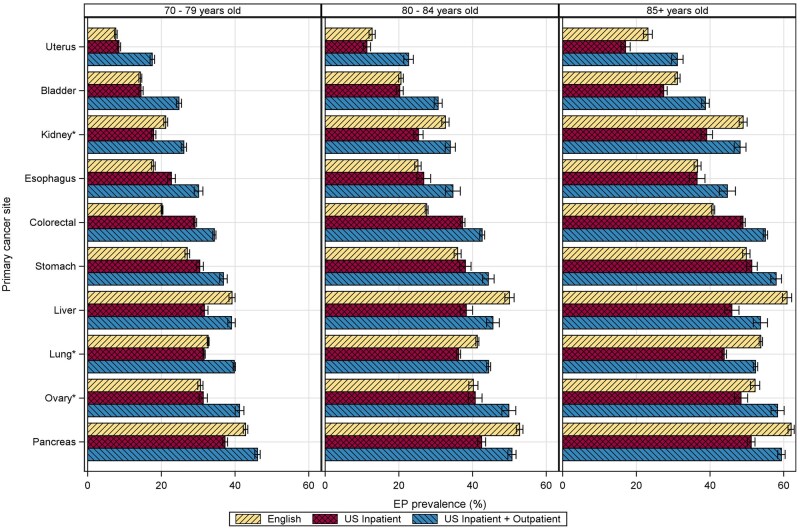 Figure 5
Figure 5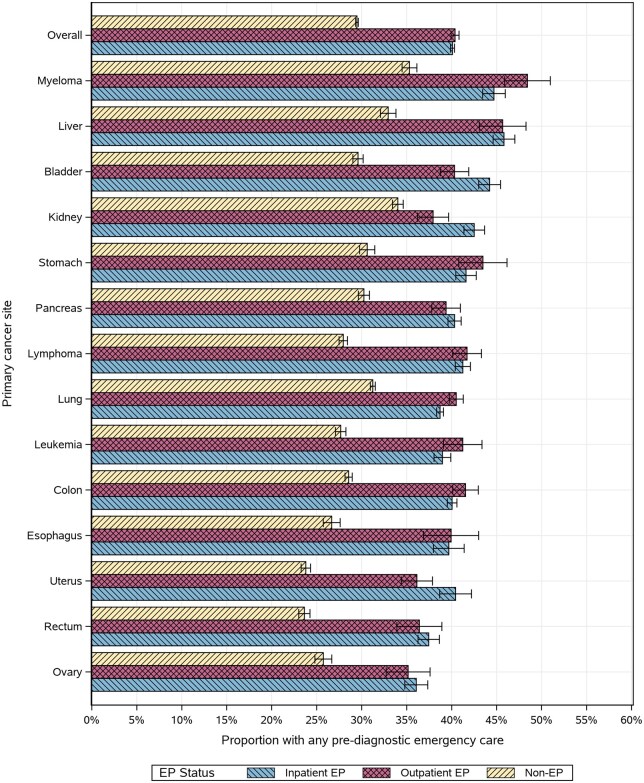 Figure 6
Figure 6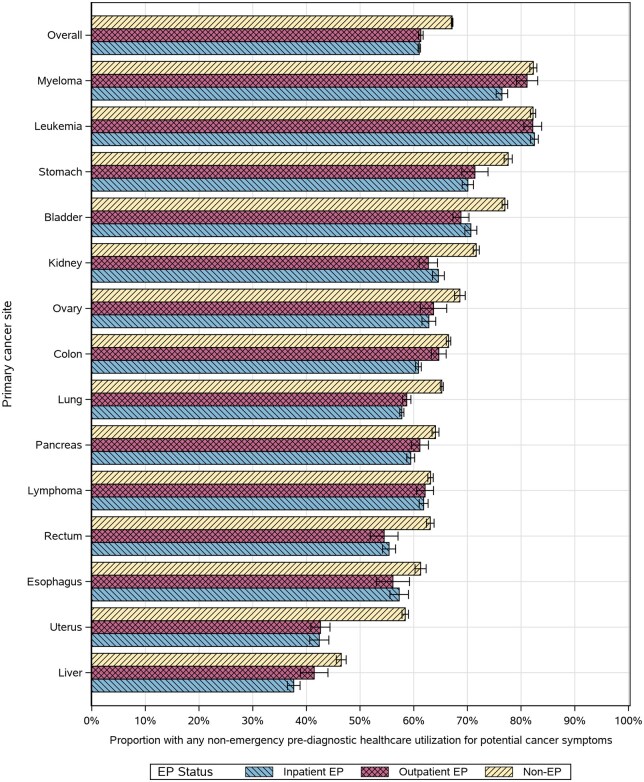 Figure 7
Figure 7| Characteristics | All patients ( | Non-EP ( | Inpatient EP ( | Outpatient EP ( |
|---|---|---|---|---|
| No. (col %) | No. (col %) [row %] | No. (col %) [row %] | No. (col %) [row %] | |
| Sex | ||||
| Male | 295 575 (48) | 186 285 (49) [63] | 86 953 (46) [29] | 22 337 (47) [8] |
| Female | 319 310 (52) | 193 994 (51) [61] | 100 486 (54) [32] | 24 830 (53) [8] |
| Age, y | ||||
| 66–70 | 144 613 (24) | 97 850 (26) [68] | 35 600 (19) [25] | 11 163 (24) [8] |
| 71–75 | 142 925 (23) | 94 796 (25) [66] | 37 388 (20) [26] | 10 741 (23) [8] |
| 76–80 | 128 586 (21) | 80 914 (21) [63] | 37 872 (20) [30] | 9800 (21) [8] |
| 81–85 | 105 595 (17) | 61 343 (16) [58] | 36 291 (19) [34] | 7961 (17) [8] |
| 86–90 | 64 865 (11) | 33 217 (9) [51] | 26 532 (14) [41] | 5116 (11) [8] |
| 91–95 | 23 704 (4) | 10 370 (3) [44] | 11 363 (6) [48] | 1971 (4) [8] |
| Older than 95 | 4597 (<1) | 1789 (<1) [39] | 2393 (1) [52] | 415 (<1) [9] |
| Race and ethnicity | ||||
| Non-Hispanic White | 502 455 (82) | 317 309 (83 [63] | 146 526 (78) [29] | 38 620 (82) [8] |
| Non-Hispanic Black | 45 053 (7) | 22 946 (6) [51] | 18 529 (10) [41] | 3578 (8) [8] |
| Hispanic | 34 139 (6) | 19 010 (5) [57] | 12 278 (7) [36] | 2851 (6) [8] |
| American Indian or Alaska Native | 2404 (<1) | 1465 (<1) [61] | 664 (<1) [28] | 275 (<1) [11] |
| East Asian American | 14 394 (2) | 9247 (2) [64] | 4422 (2) [31] | 725 (2) [5] |
| South Asian American | 1877 (<1) | 1210 (<1) [65] | 541 (<1) [29] | 126 (<1) [7] |
| Southeast Asian American | 6980 (1) | 3946 (1) [57] | 2572 (1) [37] | 462 (1) [7] |
| Other Asian American | 3362 (<1) | 2142 (<1) [64] | 1013 (<1) [30] | 207 (<1) [6] |
| Native Hawaiian or other Pacific Islander | 1437 (<1) | 795 (<1) [55] | 495 (<1) [34] | 147 (<1) [10] |
| Mixed race, another race, or unknown race | 2784 (<1) | 2209 (<1) [56] | 399 (<1) [36] | 176 (<1) [8] |
| Tumor site | ||||
| Bladder | 34 787 (6) | 24 628 (7) [71] | 6461 (3) [19] | 3698 (8) [11] |
| Colon | 85 743 (14) | 48 969 (13) [57] | 32 133 (17) [38] | 4641 (10) [5] |
| Esophagus | 12 701 (2) | 8542 (2) [67] | 3170 (2) [25] | 989 (2) [8] |
| Kidney | 34 373 (6) | 24 169 (6) [70] | 7149 (4) [21] | 3055 (7) [9] |
| Leukemia | 35 495 (6) | 22 889 (6) [65] | 10 564 (6) [30] | 2042 (4) [6] |
| Liver | 19 319 (3) | 11 352 (3) [59] | 6546 (4) [34] | 1421 (3) [7] |
| Lung | 185 403 (30) | 107 124 (28 [58] | 62 918 (34) [34] | 15 361 (33) [8] |
| Lymphoma (non-Hodgkin) | 51 892 (8) | 35 033 (9) [68] | 13 222 (7) [26] | 3637 (8) [7] |
| Myeloma | 20 437 (3) | 12 953 (3) [63] | 5991 (3) [29] | 1493 (3) [7] |
| Ovary | 15 251 (3) | 8330 (2) [55] | 5445 (3) [36] | 1476 (3) [10] |
| Pancreas | 42 075 (7) | 21 166 (6) [50] | 17 265 (9) [41] | 3644 (8) [9] |
| Rectum | 25 540 (4) | 17 733 (5) [69] | 6379 (3) [25] | 1428 (3) [6] |
| Stomach | 20 153 (3) | 11 599 (3) [58] | 7236 (4) [36] | 1318 (3) [7] |
| Uterus | 31 716 (5) | 25 792 (7) [81] | 2960 (2) [9] | 2964 (6) [10] |
| Summary stage | ||||
| Solid tumors | ||||
| Localized | 166 806 (27) | 123 547 (33) [74] | 31 294 (17) [19] | 11 965 (25) [7] |
| Regional | 127 637 (21) | 81 059 (21) [64] | 37 060 (20) [29] | 9518 (20) [8] |
| Distant, metastatic | 176 701 (29) | 84 653 (22) [48] | 76 336 (41) [43] | 15 712 (33) [9] |
| Unknown stage | 35 917 (6) | 20 145 (5) [56] | 12 972 (7) [36] | 2800 (6) [8] |
| Nonsolid tumors | 107 824 (18) | 70 875 (19) [66] | 29 777 (16) [28] | 7172 (15) [7] |
| Tumor grade | ||||
| Well differentiated | 35 113 (6) | 26 574 (7) [76] | 6 263 (3) [18] | 2276 (5) [7] |
| Moderately differentiated | 126 748 (21) | 85 193 (22) [67] | 33 382 (18) [26] | 8173 (17) [6] |
| Poorly differentiated | 99 840 (16) | 62 800 (17) [63] | 29 066 (16) [29] | 7974 (17) [8] |
| Undifferentiated | 36 442 (6) | 24 656 (7) [68] | 8027 (4) [22] | 3759 (8) [10] |
| Hemopoietic and lymphoid neoplasms | 85 506 (14) | 58 418 (15) [68] | 21 339 (11) [25] | 5749 (12) [7] |
| Unknown | 231 236 (38) | 122 638 (32) [53] | 89 362 (48) [39] | 19 236 (41) [8] |
| Charlson Comorbidity Index (excluding 90 days prior to index) | ||||
| 0 | 208 069 (34) | 136 571 (36) [66] | 55 562 (30) [27] | 15 936 (34) [8] |
| 1 | 145 230 (24) | 93 744 (25) [65] | 40 109 (21) [28] | 11 377 (24) [8] |
| 2 | 99 765 (16) | 61 261 (16) [61] | 30 732 (16) [31] | 7772 (17) [8] |
| ≥3 | 161 821 (26) | 88 703 (23) [55] | 61 036 (33) [38] | 12 082 (26) [8] |
| Kim Frailty Index (excluding 90 days prior to index) | ||||
| Robust | 312 123 (51) | 208 012 (55) [67] | 80 924 (43) [26] | 23 187 (49) [7] |
| Pre-frail | 256 595 (42) | 152 787 (40) [60) | 83 458 (45) [33] | 20 350 (43) [8] |
| Mildly frail | 40 901 (7) | 17 708 (5) [43] | 19 934 (11) [49] | 3259 (7) [8] |
| Moderate-to-severely frail | 5266 (1) | 1772 (<1) [34] | 3123 (2) [59] | 371 (1) [7] |
| Medicaid eligibility (any vs none) | ||||
| Full | 88 394 (14) | 43 003 (11) [49] | 38 145 (20) [43] | 7246 (15) [8] |
| Partial | 21 906 (4) | 11 784 (3) [54] | 7743 (4) [35] | 2379 (5) [11] |
| None | 504 585 (82) | 325 492 (86 [65] | 141 551 (76) [65] | 37 542 (80) [7] |
| Neighborhood socioeconomic status, percentile | ||||
| 0-20th | 95 983 (16) | 53 254 (14) [56] | 34 119 (18) [36] | 8610 (18) [9] |
| 20th-40th | 120 831 (20) | 72 108 (19) [60] | 38 161 (20) [32] | 10 562 (22) [9] |
| 40th-60th | 124 942 (20) | 77 073 (20) [62] | 37 964 (20) [30] | 9905 (21) [8] |
| 60th-80th | 125 855 (21) | 80 152 (21) [64] | 36 853 (20) [29] | 8850 (19) [7] |
| 80th-100th | 124 393 (20) | 83 587 (22) [67] | 33 194 (18) [27] | 7612 (16) [6] |
| Unknown | 22 881 (4) | 14 105 (4) [62] | 7148 (4) [31] | 1628 (4) [7] |
| County urbanicity | ||||
| Metropolitan | 523 317 (85) | 322 843 (85 [62] | >164 835 (>88) [32] | >35 632 (>76) [7] |
| Urban, nonmetropolitan | 81 433 (13) | 50 966 (13) [63] | 20 253 (11) [25] | 10 214 (22) [13] |
| Rural | 10 073 (2) | 6423 (2) [64] | 2340 (1) [23] | 1310 (3) [13] |
| Unknown | 62 (<1) | 47 (<1) [76] | < 11 (<1) [<24] | < 11 (<1) [<24] |
- —National Cancer Institute at the National Institutes of Health10.13039/100000054
- —Cancer Research United Kingdom
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmergency and Acute Care Studies · Global Cancer Incidence and Screening · COVID-19 and healthcare impacts
Introduction
Diagnostic delays worsen outcomes for cancer patients worldwide and may reflect missed opportunities to diagnose cancer through earlier ambulatory care.1^,^2 To pinpoint missed opportunities for diagnosis in administrative health-care data, diagnosis of cancer through care originating in the emergency department (ED) was recently proposed as a health-care quality metric.2 This measure of emergency presentation has been extensively examined outside the United States (US), often defined as cancer diagnosis following emergency hospital admission.3^,^4 Multiple studies identified emergency presentation as a predictor of poor survival independent of cancer stage.3^,^4 Yet, US estimates of emergency presentation prevalence and factors driving emergency presentation remain unreported for many cancer types.
Emergency presentations can be caused by a variety of circumstances, from rapid cancer progression with sudden severe symptoms to health-care access barriers resulting in reliance on the ED for primary care.2^,^5-10 Such barriers include extensive wait times in nonemergency settings, difficulty navigating the health-care system, poor care quality resulting in diagnostic errors, and other psychosocial and socioeconomic factors like lack of time and transportation for care.11^,^12 These factors are particularly relevant to the United States where the ED is frequently attended by patients with no regular health-care provider.13 Unlike aggressive cancer biology, barriers to care may be a more readily intervenable cause of emergency presentation. Better understanding of patients affected by emergency presentations, especially those that are avoidable, can translate to improved outcomes.
We previously reported the prevalence of emergency presentation of 4 common cancer types noting many patients had ED contact within 4 weeks before diagnosis.5 Here we report prevalence of emergency presentation across 14 cancer types examining subgroups of emergency presentation not previously presented. Many international studies define emergency presentation as emergency hospitalization before cancer diagnosis, often within the prior month,3^,^4 whereas most US studies consider any emergency care in the 30 days before diagnosis, combining patients hospitalized and discharged after emergency care.2^,^5-7 Here, we separate emergency presentations into patients diagnosed during or following an emergency hospitalization (“inpatient emergency presentations,” admission from the ED, or hospitalization of an emergency admission “type”), and patients diagnosed following discharge from the ED without hospitalization (“outpatient emergency presentations”). Because outpatient emergency presentations are able to be discharged, we hypothesized they would be less likely to have suddenly presented with severe symptoms indicative of unavoidable emergency presentation. We suspected this group may instead consist of patients presenting to the ED because of barriers to care related to socioeconomic disadvantage or access. To evaluate this hypothesis, we assessed whether outpatient emergency presentation patients have lower income or reside in rural neighborhoods with fewer prior nonemergency encounters for symptoms and higher overall ED use before cancer diagnosis. For additional international context, we contrasted emergency presentation prevalence among US older adults with similar metrics from England. To our knowledge, this is the first conceptualization of emergency presentations in this manner and the first United States-to-international comparison of emergency presentation prevalence.
Methods
Data source and study population
We used data from the Surveillance, Epidemiology, and End Results (SEER)–Medicare database.14 Patients were diagnosed from 2008 to 2017 with cancers of the colon, rectum, esophagus, stomach, liver and intrahepatic bile duct, pancreas, lung and bronchus, kidney and renal pelvis, urinary bladder, uterus, ovary, leukemia, non-Hodgkin lymphoma, and multiple myeloma. Breast and prostate cancers were excluded because of common detection through screening and low ED involvement.5 Because Medicare coverage typically begins at age 65 years and a year of fee-for-service claims was needed to classify prediagnostic care, we included patients aged 66 years and older with continuous Medicare Parts A and B and no Medicare Advantage enrollment in the year before diagnosis. We also excluded patients with prior cancers or diagnoses by autopsy or death certificate only.
Classification of emergency presentation subgroups
Using a published algorithm,15^,^16 we derived the date of the earliest cancer-specific International Classification of Diseases (ICD) code in the SEER month of diagnosis (+/- 1 month) as the “index date” (Table S1). All patients with an emergency-associated claim in the 30 days before this date were classified as emergency presentations based on ED revenue codes (0450-0459) or hospitalizations with an emergency admission type, while all others were considered nonemergency presentations (see Figure 1). To explore adequacy of the 30-day lookback, we plotted the frequency of ED visits 120 days before the index date color-coded by emergency presentation status (see Figure 2). We subclassified emergency presentations based on their ED discharge disposition: inpatient emergency presentation if ED contact resulted in emergency hospitalization (see Figure 1) and outpatient emergency presentation if not.
Algorithm for classifying inpatient and outpatient emergency presentation vs nonemergency presentation. 1ED-associated revenue code (0450-0459) OR a short-term acute care hospitalization (Medicare Provider Analysis and Review file) with an emergency admission type. 2Index date: Date of the earliest cancer-specific International Classification of Diseases code appearing on a claim in the Surveillance, Epidemiology, and End Results month of diagnosis (+/− 1 month). 3Emergency inpatient hospitalization or emergency transfer: The short-term acute care inpatient stay (Medicare Provider Analysis and Review file) has an ED-associated revenue code (0450-0459) OR the inpatient stay has an admission type of ED OR ED revenue code within 3 days before hospital admission. Abbreviations: ED = emergency department; EP = emergency presentation.
Frequency of all ED visits in the study cohort up to 120 days prediagnosis and 20 days postdiagnosis relative to the index date, colored by emergency presentation status. The lookback window for EP is shown in gray tick marks. Abbreviations: ED = emergency department; EP = emergency presentation.
Patient sociodemographic and clinical characteristics
We obtained sociodemographic variables from SEER, including age, sex, race and ethnicity (Table S2), neighborhood-level socioeconomic status (SES),17 and county urbanicity based on US Department of Agriculture Rural Urban Continuum Codes.18 We also examined clinical characteristics, including tumor site, SEER summary stage, the Charlson Comorbidity Index,19 the Kim frailty index with preestablished cut points, and Medicaid dual eligibility from the Medicare files.20^,^21 To reflect clinical characteristics before cancer diagnosis, comorbidity and frailty indices were calculated using claims 90 to 365 days before the index date.
English emergency presentation estimates
We used publicly available age-stratified National Health Service (NHS) summary statistics on routes to diagnosis, which use an algorithmic classification for different prediagnostic care scenarios.3 NHS emergency presentations include patients diagnosed via accident and emergency, emergency general practitioner referral, emergency transfer, or emergency admission or attendance, with most emergency presentations including hospitalization.3^,^22 We calculated the English emergency presentation proportion as the number of patients diagnosed via emergency presentation divided by the number of total cancer patients diagnosed during the years under study, comparing with both the US inpatient emergency presentation and total emergency presentation proportions.23 To improve comparability with our cohort, we excluded patients aged younger than 70 years and those with leukemia, lymphoma, and myeloma, for which NHS data were not publicly available, and collapsed the colon and rectum cancer groups. Differences in emergency presentation prevalence were assessed using tests of proportions (Table S3).
Prediagnostic health-care utilization
We defined the prediagnostic period as the year before the index date, excluding the 30-day window used to classify emergency presentations. We quantified prediagnostic care including ED visits and non-ED visits for potential cancer symptoms by emergency presentation status. For the latter, we reviewed studies of symptoms for each cancer type (eg, abdominal bloating for colorectal cancer, chronic cough for lung cancer)24-28 (Table S4) and flagged claims with these ICD-9 and ICD-10 codes. To avoid mixing ED utilization with symptom-related care, we ignored symptom ICD codes on the same day as an ED visit.
Statistical analysis
We reported the proportion of inpatient emergency presentations, outpatient emergency presentations, and nonemergency presentations overall and by stage and tumor site. We estimated prevalence differences for demographic and clinical characteristics described above using separate linear regression models with nonemergency presentations as the reference group,29^,^30 adjusting for age (modeled using 5-year age categories), SEER summary stage, sex, and tumor type. We also estimated prevalence differences for outpatient vs inpatient emergency presentations (excluding nonemergency presentations) using the same adjustment set. All statistical analyses were conducted in SAS v9.4 (SAS Institute, Cary, NC, USA).
Results
Of 614 885 included beneficiaries, 234 606 (38%) were diagnosed as emergency presentations, among whom 187 439 (80%) were hospitalized following emergency care (inpatient emergency presentations) (Table 1). Across the study population, the greatest frequency of ED visits occurred on the index date marking diagnosis. Increases in ED visits were observed as early as 70 days before diagnosis, with steeper increases during the 30-day lookback window defining emergency presentation (Figure 2). Emergency presentation prevalence was greatest for patients with cancers of the pancreas (50%), ovary (45%), and colon (43%) and lowest for those with kidney (30%), bladder (29%), and uterine cancer (19%) (Figure 3). Inpatient emergency presentations were more prevalent among those with later stage cancer (43% of metastatic vs 19% of localized), yet outpatient emergency presentations did not vary substantially by cancer type or stage (9% of metastatic vs 7% of localized).
*The proportion of cancers diagnosed as an inpatient and outpatient emergency presentation (EP) overall and by cancer site and stage across the 11 solid tumor sites, including from left to right inpatient EPs, outpatient EPs, and non-EPs. Total includes unstaged cancers.
Relative to nonemergency presentations, adjusted prevalence differences for inpatient emergency presentation were higher for patients who were older (prevalence difference = 28%, 95% confidence interval [CI] = 26% to 29%, for ages 95 years and older vs ages 66-70 years), frailer (prevalence difference = 29%, 95% CI = 28% to 30%, for moderate-to-severely frail vs robust), and more comorbid (prevalence difference = 10%, 95% CI = 9% to 10%, for Charlson Comorbidity Index ≥ 3 vs Charlson Comorbidity Index = 0) (Figure 4). Many of these factors were also associated with outpatient emergency presentations compared with nonemergency presentations, though with weaker prevalence differences. For example, outpatient emergency presentations were also more common among older patients (prevalence difference = 9%, 95% CI = 7% to 10%, for ages 95 years and older vs ages 66-70 years) and the highly frail (prevalence difference = 7%, 95% CI = 5% to 8%, for moderate-to-severely frail vs robust). Demographics associated with inpatient emergency presentation vs nonemergency presentation included specific race and ethnic groups (all vs non-Hispanic White): non-Hispanic Black (prevalence difference = 11%, 95% CI = 10% to 11%), Hispanic (prevalence difference = 7%, 95% CI = 6% to 7%), Southeast Asian (prevalence difference = 6%, 95% CI = 4% to 7%), Native Hawaiian or other Pacific Islander (prevalence difference = 6%, 95% CI = 3% to 9%); Medicaid eligibility (prevalence difference = 15%, 95% CI = 15% to 16%, for fully vs not eligible); and living in lower SES neighborhoods (prevalence difference = 9%, 95% CI = 8% to 9%, lowest vs highest quintile) (Figure 4). Non-Hispanic Black, Hispanic, and Native Hawaiian or other Pacific Islander race and ethnicity, dual eligibility, and lower neighborhood-level SES were also related to increased prevalence of outpatient emergency presentations (vs nonemergency presentations) but with associations equal to or less than those of inpatient emergency presentations. Only one race and ethnic group, American Indian or Alaska Native, was associated with outpatient emergency presentations (prevalence difference = 5%, 95% CI = 3% to 7%) and not inpatient emergency presentations. Relative to inpatient emergency presentations, outpatient emergency presentations were 8% (95% CI = 5% to 10%) higher among American Indian or Alaska Native (vs non-Hispanic White) individuals. Outpatient emergency presentations were also more common in nonmetropolitan counties compared with nonemergency presentations (prevalence difference = 6%, 95% CI = 6% to 7%, for nonmetropolitan urban, and prevalence difference = 7%, 95% CI =6% to 7%, for rural vs metropolitan counties). In models restricted to emergency presentations, these differences were substantial; rural emergency presentations had an 18% higher adjusted prevalence of outpatient emergency presentation (vs inpatient emergency presentation) compared with patients in metropolitan counties.
Adjusted prevalence differences of inpatient and outpatient emergency presentation (EP) (vs non-EP) and outpatient vs inpatient EP. Prevalence differences were generated using separate models for each characteristic additionally adjusted for age, sex, tumor site, and summary stage at diagnosis. Abbreviations: AIAN = American Indian or Alaska Native; CI = confidence interval; EP = emergency presentation; NHB = non-Hispanic Black; NHOPI = Native Hawaiian or other Pacific Islander; NWH = non-Hispanic White; PD = prevalence difference; ref = referent; SES = socioeconomic status.
In the population of those aged 70 years and older with the 10 included cancer sites, US inpatient emergency presentations exceeded English emergency presentations for esophageal, colorectal, and stomach cancer, while English emergency presentations exceeded US inpatient emergency presentations for kidney, liver, lung, and pancreatic cancers (Figure 5). English emergency presentation proportions were similar to the US inpatient emergency presentation proportions for uterus, bladder, and ovarian cancer, aside from the oldest age group (85 years and older), among which English emergency presentations were greater. English emergency presentations exceeded the total US emergency presentation estimate of inpatient and outpatient emergency presentations for liver and pancreatic cancer.
*Proportion of emergency presentations in SEER-Medicare data compared with English estimates from National Health Service CancerData stratified by age group. Included age groups and cancer sites reflect the NHS data available.Kidney cancers included renal pelvis in the SEER-Medicare data but not in the NHS data. Ovarian cancers included fallopian tube or primary peritoneal carcinomas, and lung cancers included tracheal cancers in the NHS data but not in the SEER-Medicare data. Abbreviations: EP = emergency presentation; NHS = National Health Service; SEER = Surveillance, Epidemiology, and End Results.
Fewer nonemergency presentations had prediagnostic ED visits (30%, 95% CI = 29% to 30%), but this proportion did not vary overall between inpatient (40%, 95% CI = 40% to 40%) and outpatient (40%, 95% CI = 40% to 41%) emergency presentations (Figure 6). Stratified by cancer type, more patients had prediagnostic ED utilization among inpatient emergency presentations than outpatient emergency presentations for uterine, kidney, and bladder cancer. Alternatively, more outpatient emergency presentation patients had prediagnostic ED visits than inpatient emergency presentations for those with lung cancer and myeloma.
Proportion of patients with any emergency care in the prediagnostic period before the emergency presentation (EP) window (ie, excluding the 30 days before the index), stratified by cancer site and EP status.
Patients with nonemergency prediagnostic care for potential cancer symptoms before the emergency presentation lookback window were slightly more prevalent among nonemergency presentations (67%, 95% CI = 67% to 67%) compared with emergency presentations, also with little variation between inpatient (61%, 95% CI = 61% to 61%) and outpatient (61%, 95% CI = 61% to 62%) emergency presentations (Figure 7). By cancer site, this care was slightly more common for outpatient vs inpatient emergency presentations among patients with myeloma, colon, or liver cancer; no cancer type had a statistically greater prevalence of nonemergency care among inpatient emergency presentations than outpatient emergency presentations (Figure 7).
Proportion of patients with any nonemergency health-care utilization for site-specific potential cancer symptoms in the prediagnostic period before the emergency presentation (EP) window (ie, excluding the 30 days before the index), stratified by cancer site and EP status.
Discussion
We report emergency presentation prevalence across a range of cancer types, including many not previously reported in US populations, among Medicare beneficiaries reflecting most US adults aged older than 65 years. More than 1 in 3 patients with pancreatic, ovarian, colon, stomach, myeloma, lymphoma, lung, liver, and esophageal cancers were diagnosed through an emergency presentation route. These cancer sites have poor survival and may be overrepresented among emergency presentations because of aggressive disease or broad, nonspecific symptom profiles complicating timely diagnosis in routine care.24^,^31 In contrast, sites with lower emergency presentation prevalence in our study (eg, uterus and bladder) tend to have more specific and alarming symptoms, such as postmenopausal bleeding or hematuria, which may prompt more straightforward diagnostic evaluation.24^,^32^,^33 Emergency presentation prevalence in this study was nearly double that of recent US estimates for colorectal and lung cancer using electronic health records.2^,^6 This may reflect the older age of our cohort and more complete capture of emergency care in Medicare claims compared with electronic health records, which often miss care outside a given health-care system.34 Consistent with prior findings,10 emergency presentation was more prevalent among patients with poor underlying health and advanced cancer, as well as barriers to care including lower neighborhood SES and geographic isolation.
Unlike prior studies, we examined emergency presentations stratified by care pathway following ED evaluation. Patients diagnosed as outpatient emergency presentations were a distinct group with less clinical acuity and more rurality than inpatient emergency presentations. Although existing emergency presentation literature primarily emphasizes factors driving unavoidable emergency care, such as older age, greater comorbidity, and frailty, and more advanced stage, we observed that these associations were substantially weaker for outpatient emergency presentations. Even in this insured population, outpatient emergency presentations were also more likely than nonemergency presentations to live in disadvantaged neighborhoods and rural counties, areas often affected by provider shortages and limited health-care access.35 Although inpatient emergency presentations also appeared driven partly by access barriers, outpatient emergency presentations did not share the same associations with later stage or poorer clinical condition as inpatient emergency presentations, indicating outpatient emergency presentations may more specifically reflect lack of access to a usual source of quality care rather than clinical acuity. Combining US inpatient and outpatient emergency presentations may obscure important heterogeneity in the drivers of emergency presentation. Specifically examining outpatient emergency presentations may help identify modifiable missed opportunities for earlier diagnosis, as these may more strongly reflect barriers to care rather than severe disease.
Although the English emergency presentation estimates were produced by a different algorithm than used here, reflecting different data sources and underlying health-care systems, they may conceptually be most comparable to US inpatient emergency presentations because most English emergency presentations include a hospital admission.22 The English algorithm uses a 28-day prediagnostic window rather than 30 days as used here and in most US studies, though this has been shown to minimally impact results.3^,^4 The proportion of patients diagnosed through emergency presentation in England was similar to our estimates for many cancer sites, though with some variability for gastrointestinal cancers. Variation in emergency presentation estimates across countries may generate hypotheses about how differences in earlier care could influence emergency presentation. For instance, the greater prevalence of US inpatient emergency presentation for colorectal cancers relative to England may reflect differences in screening uptake and frequency.36 However, dissimilarities in data sources, algorithms, and health-care systems should be kept in mind; many English emergency presentations are classified based on emergency general practitioner referrals not explicitly quantified here,22 while the lack of a usual source of primary care may not contribute to English emergency presentation as substantially.
As previously reported,5^,^9^,^10 our findings indicate several racial and ethnic groups are disproportionately affected by emergency presentations. We report for the first time that non-Hispanic Black, Hispanic, Southeast Asian, and Native Hawaiian or other Pacific Islander patients had stronger associations with inpatient emergency presentation than outpatient emergency presentation, which may reflect greater comorbidity or cancer aggressiveness resulting from the accumulation of systemic health barriers.37 Interestingly, American Indian or Alaska Native patients did not follow this pattern, with higher prevalence of outpatient emergency presentations than other groups even after adjusting for age, sex, stage, and cancer site. Some American Indian or Alaska Native patients may receive emergency services through the Indian Health Service, which lacks specialized cancer care and may be more likely to reside on rural reservation lands, factors that could contribute to outpatient-only ED care.38 These patterns and subsequent consequences of outpatient emergency presentations on outcomes in these populations warrant further investigation.
Patients diagnosed as emergency presentations were more likely to have ED visits in the year before diagnosis, suggesting greater reliance on the ED as a usual source of care. We hypothesized prediagnostic ED use would be even higher among patients diagnosed through outpatient emergency presentations than inpatient emergency presentations; yet, aside from a few site-specific exceptions, both groups were equally likely to have prediagnostic emergency care. As an older, frailer, and more comorbid group, inpatient emergency presentations may have greater need for emergency care, resulting in high ED utilization regardless of access barriers. Although the proportion receiving prediagnostic care for potential cancer symptoms outside the ED was somewhat lower for emergency presentations than nonemergency presentations, this difference was less than 5 percentage points, challenging the notion that emergency presentation patients simply did not seek other care for symptoms before presenting to the ED. We also hypothesized outpatient emergency presentations would have less prediagnostic care for cancer symptoms than inpatient emergency presentations, though the proportions were ultimately similar across both groups. Nonetheless, we could not assess whether quality of prediagnostic care differed between subgroups, which could partly explain the reliance of patients with outpatient emergency presentation on the ED, even in the absence of disease severity requiring hospitalization.
Our findings assume emergency care in the 30 days before the index date (a convention used in many prior studies) was related to the soon-to-be diagnosed cancer rather than unrelated conditions.2^,^4-7 To assess the reliability of this window, we examined the density of ED visits over time, which increased as early as 70 days before the index. This suggests some earlier ED visits may relate to cancer symptoms; the best lookback window for measuring emergency presentation should be evaluated further. Strengths of this study included use of Medicare data well-suited for identifying emergency presentations because of continuity of coverage after enrollment and inclusion of care across different hospital systems. Although some emergency care may have been billed to secondary insurance and not captured here, we expect this was minimal. Importantly, our findings are less generalizable to younger patients and individuals without continuous health insurance, who may have more access barriers and rely more heavily on the ED for routine care needs. Additionally, our study underrepresents Medicare Advantage beneficiaries, an increasingly large segment of the Medicare population who may have better access to primary care and care coordination services.39 Future work should assess whether emergency presentation patterns differ in these groups and examine how differences in care continuity affect emergency presentations and missed diagnostic opportunities.
Our results provide comprehensive estimates of emergency presentation among US older adults with previously understudied cancer types and suggest the presence of meaningful subgroups within emergency presentation, revealing important heterogeneity that may be obscured when these subgroups are combined. Stratifying emergency presentations by whether patients were hospitalized after emergency care may help pinpoint drivers of avoidable emergency presentations, with outpatient emergency presentations serving as more specific indicators of care quality less affected by unmodifiable factors like underlying health status and cancer aggressiveness.2^,^40 Targeted efforts are needed to strengthen primary care access, care continuity, and early diagnostic evaluation, particularly in rural and underserved areas. Future studies should examine quality and timeliness of prediagnostic care in these subgroups and develop strategies to reduce missed diagnostic opportunities, with a particular focus on outpatient emergency presentations.
Supplementary Material
pkag008_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hanna TP , King WD, Thibodeau S, et al Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020;371:m 4087. 10.1136/bmj.m 408733148535 PMC 7610021 · doi ↗ · pubmed ↗
- 2Kapadia P , Zimolzak AJ, Upadhyay DK, et al Development and implementation of a digital quality measure of emergency cancer diagnosis. J Clin Oncol. 2024;42:2506-2515. 10.1200/JCO.23.0152338718321 PMC 11268555 · doi ↗ · pubmed ↗
- 3Elliss-Brookes L , Mc Phail S, Ives A, et al Routes to diagnosis for cancer–determining the patient journey using multiple routine data sets. Br J Cancer. 2012;107:1220-1226. 10.1038/bjc.2012.40822996611 PMC 3494426 · doi ↗ · pubmed ↗
- 4Mc Phail S , Swann R, Johnson SA, et al; ICBP Module 9 Emergency Presentations Working Group. Risk factors and prognostic implications of diagnosis of cancer within 30 days after an emergency hospital admission (emergency presentation): an International Cancer Benchmarking Partnership (ICBP) population-based study. Lancet Oncol. 2022;23:587-600. 10.1016/S 1470-2045(22)00127-935397210 PMC 9046095 · doi ↗ · pubmed ↗
- 5Thompson CA , Sheridan P, Metwally E, et al Emergency department involvement in the diagnosis of cancer among older adults: a SEER-Medicare study. JNCI Cancer Spectrum. 2024;8:pkae 039. 10.1093/jncics/pkae 03938796687 PMC 11193434 · doi ↗ · pubmed ↗
- 6Zimolzak AJ , Khan SP, Singh H, Davila JA. Application of a digital quality measure for cancer diagnosis in Epic Cosmos. J Am Med Inform Assoc. 2025;32:227-229. 10.1093/jamia/ocae 25339394724 PMC 11648705 · doi ↗ · pubmed ↗
- 7Sikka V , Ornato JP. Cancer diagnosis and outcomes in Michigan E Ds vs other settings. Am J Emerg Med. 2012;30:283-292. 10.1016/j.ajem.2010.11.02921247723 · doi ↗ · pubmed ↗
- 8Pettit NR , Noriega A, Missen MRV. Retrospective review of patients with lung cancer presenting emergently. Am J Emerg Med. 2023;71:129-133. 10.1016/j.ajem.2023.06.02737392511 · doi ↗ · pubmed ↗