Cryptococcid Sweet Syndrome in the Setting of Hydralazine‐Induced ANCA Vasculitis: A Case Report
Jenna Vroman, Pelin Sagut, Kathryn Lynam, Amanda Ederle, Laura Winterfield

TL;DR
A rare case of cryptococcoid Sweet syndrome combined with hydralazine-induced vasculitis is reported, highlighting the importance of accurate diagnosis.
Contribution
This case report documents the rare co-occurrence of cryptococcoid Sweet syndrome and hydralazine-induced ANCA vasculitis.
Findings
Cryptococcoid Sweet syndrome can mimic fungal infection histologically but is non-infectious.
The patient had hydralazine-induced ANCA vasculitis alongside Sweet syndrome, a rare combination.
Accurate diagnosis is crucial to avoid unnecessary antifungal treatment.
Abstract
Acute febrile neutrophilic dermatosis, also known as Sweet syndrome, is an inflammatory skin condition characterized by the rapid onset of painful, erythematous plaques or nodules with neutrophilic infiltrate on histology. Rarely, acellular bodies surrounded by vacuolated spaces have been noted within the neutrophilic infiltrate, mimicking Cryptococcus infection. Despite these histological findings, the cryptococcoid variant of Sweet syndrome is not an infectious process. This delineation is essential for the initiation of proper treatment. Here, we present a patient with cryptococcoid Sweet syndrome with concomitant hydralazine‐induced ANCA vasculitis, which has seldom been reported in the literature.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
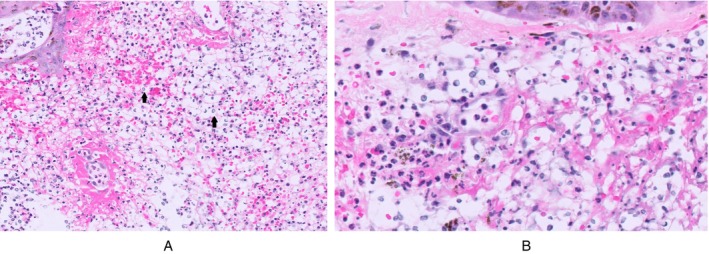 FIGURE 1
FIGURE 1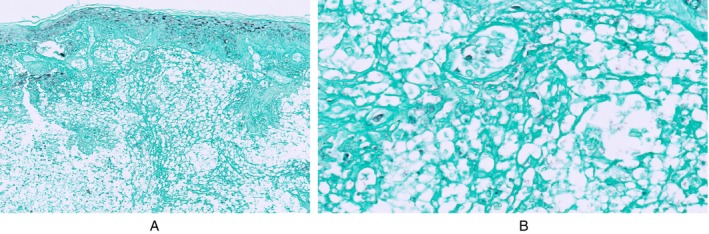 FIGURE 2
FIGURE 2| Major criteria |
| 1. Acute onset of tender erythematous plaques or nodules |
| 2. Dense neutrophilic infiltrate on biopsy |
| Minor criteria |
| 1. Fever, temperature > 38°C |
| 2. Association with an underlying hematologic malignancy, inflammatory disease, or pregnancy, or preceded by an upper respiratory or gastrointestinal tract infection |
| 3. Rapid response to treatment with systemic corticosteroids |
| 4. Abnormal laboratory values at presentation (3 of 4):
Erythrocyte sedimentation rate > 20 mm/h Positive C‐reactive protein Leukocyte count > 10 × 103/μL > 70% neutrophils |
| Reference | Age/sex | Past medical history | Distribution of lesions | Positive serologic autoantibodies | Concomitant vasculitis noted? | Pulmonary and/or neurological involvement? | Medications | Treatment management |
|---|---|---|---|---|---|---|---|---|
| Current case | 67/M | COPD, ESRD, history of GI bleeds | Face, hands, legs, feet | pANCA, MPO, anti‐DNase | Yes, noted on biopsy | Yes. PNA complicated by hypoxic respiratory failure as well as encephalopathy (both |
Hydralazine Acyclovir, doxycycline, vancomycin | Systemic corticosteroids |
| Alshaikh et al. [ | 63/M | None | Scalp, face, trunk, upper extremities | Not reported | Not reported | None reported | None | Systemic corticosteroids |
| Boyd et al. [ | 63/M | ESRD on HD, COPD, CAD, recurrent | Trunk, extremities | Not reported | Not reported | None reported | “Numerous,” recently started Vancomycin | Metronidazole, topical triamcinolone 0.1% cream |
| Byekova et al. [ | 82/F | DM, CKD | Mouth, tongue, trunk, extremities | None | Not reported | PNA complicated by respiratory failure | Not reported | N/A (died before improvement noted) |
| Fletcher et al. [ | 81/M | GI malignancy (neuroendocrine tumor), hypothryoidism, HTN, GERD, an episode of similar cutaenous eruptions 3 years prior | Forehead, cheeks, fingers | Not reported | Not reported | None reported | Not reported | Systemic corticosteroids |
| Fresco et al. [ |
73/F 50/F |
ESRD on HD, DM, CHF ESRD on HD, chronic hepatitis C infection, CAD, cocaine use, one episode of CSS documented 2 months prior |
Face, trunk, upper and lower extremities Lower extremities |
MPO MPO |
Yes, noted on biopsy Yes, noted on biopsy |
Respiratory failure and mental status deterioration Mental status deterioration |
Not reported Not reported |
N/A (died before improvement noted) Systemic corticosteroids |
| Jordan et al. [ |
81/F 87/F |
DM, metastatic breast cancer DM, HTN, CKD |
Feet, face, arms Face, trunk, extremities |
Not reported Not reported |
Not reported Not reported |
None reported None reported |
Not reported Not reported |
N/A (died before improvement noted) Systemic corticosteroids |
| Ko et al. [ |
76/F 84/F 79/F |
AML SLE CLL |
Upper and lower extremities Face, lip Face, back, neck |
ANA “Multiple autoantibodies” Not reported |
LCV noted on biopsy Yes, noted clinically Absent |
None reported PNA None reported |
Piperacillin‐tazobactam, vancomycin. Piperacillin‐tazobactam Not reported |
N/A (died before improvement noted) Systemic corticosteroids Topical metronidazole |
| Lim et al. [ | 68/F | DM, ESRD on HD | Face, hands, toes | ANCA | Absent | None reported | Had antibiotics as she was admitted for infective endocarditis but antibiotics were not specified | Systemic corticosteroids |
| Mazzei et al. [ | 18/F | Pyoderma gangrenosum, Sweet syndrome, ANCA‐positive vasculitis complicated by ESRD on HD | Face, hands | Not reported | History of vasculitis, but not otherwise noted on biopsy. | None reported | Azathioprine, prednisone, losartan, valaciclovir, trimethoprim–sulfamethoxazole | Systemic corticosteroids |
| Sherban et al. [ |
70/F 68/F 70/F |
ESRD, DM, COPD Chronic anemia, HTN, HLD ESRD, DM |
Face, neck, chest, upper extremities Face, eyelids, upper extremities, legs Head, upper extremities, tongue |
pANCA, PR3 pANCA, MPO, equivocal PR3 MPO, anti‐histone |
Absent Yes, noted on biopsy Absent |
PNA complicated by respiratory failure None reported Viral PNA |
Piperacillin/tazobactam Not reported Not reported |
Systemic corticosteroids + dapsone
N/A (died before improvement noted) Prednisone, dapsone, mycophenolate mofetil |
| Skaljic et al. [ | 70/F | HTN, DM, bladder cancer, CKD | Face, arms, legs, mouth | ANA, anti‐histone, anti‐dsDNA, pANCA, MPO | Yes, noted on biopsy | None reported | Hydralazine, amlodipine, clonidine, aspirin, clopidogrel, furosemide, simvastatin, insulin. | Systemic corticosteroids |
| Stauder et al. [ | 57/M | CKD, HTN, BPH, DM, OSA, HLD, psoriasis, substance use (+remote cocaine use) | Head, trunk, hands, extremities, tongue | ANA, pANCA, anti‐histone, MPO, PR3 | Yes, focal vasculitis noted on histology | Hypoxic respiratory failure (prior to skin lesions) | Hydralazine, insulin, amlodipine, aspirin, carvedilol, finasteride, glimepiride, losartan, metoprolol, tamsulosin. | Systemic corticosteroids + dapsone |
| Volonté et al. [ | 57/M | Anemia due to melena of unknown orgin, pauci‐immune p‐ANCA‐associated crescentic glomerulonephritis leading to ESRD on HD, COPD, HTN, gastritis | Head, tongue, lips, nasal mucosa, trunk, extremities | pANCA, MPO | Yes, focal vasculitis noted on histology. |
PNA (prior to skin lesions) Respiratory failure (after skin lesions) |
Oral prednisone, escitalopram, bisoprolol, ramipril, doxazosin. piperacillin‐tazobactam | Systemic corticosteroids |
| Wilson et al. [ |
48/F 55/F |
Anemia, cocaine use Chronic hepatitis C, RA, cocaine use |
Neck Face, trunk, extremities, mouth |
ANA, pANCA, anti‐SSA pANCA |
Absent Absent |
None reported None reported |
Not reported None |
Systemic corticosteroids Systemic corticosteroids |
| Wilson et al. [ | 75/M | HTN, DM, CAD, ESRD | Face, ears, scalp, hands, elbows | ANA, anti‐histone | Absent | PNA (prior to skin lesions) |
Aspirin, atorvastatin, clonidine, hydralazine, insulin, isosorbide mononitrate, lansoprazole, metoprolol. Piperacillin‐tazobactam | Systemic corticosteroids |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders · Cutaneous lymphoproliferative disorders research · Sarcoidosis and Beryllium Toxicity Research
Introduction
1
Acute febrile neutrophilic dermatosis, or Sweet syndrome (SS), is a systemic inflammatory skin condition characterized by fever, leukocytosis, and painful, erythematous plaques and nodules along the face, neck, and upper extremities [1]. Histologically, SS is marked by dense neutrophilic infiltrate and edema in the papillary dermis [1]. A rare histological subtype, cryptococcoid SS (CSS), presents with basophilic, acellular, vacuolated bodies within the neutrophilic infiltrate that bear a resemblance to Cryptococcus. However, staining with Grocott/Gomori methenamine silver (GMS) and periodic acid‐Schiff (PAS) fails to reveal organisms.
We present a patient with recurring hydralazine‐induced ANCA vasculitis (HIAV) and CSS with pulmonary and neurological findings. This constellation of findings is rare and highlights the spectrum of neutrophilic dermatoses and leukocytoclastic vasculitis linking HIAV and CSS.
Case Report
2
A 67‐year‐old man with a history of end‐stage renal disease (ESRD) on hemodialysis, hypertension, chronic obstructive pulmonary disease, and gastrointestinal (GI) bleeds presented to an outside hospital (OSH) due to shortness of breath and hemoptysis. The patient had no known history of immunosuppression, autoimmune diseases, or dermatologic conditions. Serological tests revealed positive p‐ANCA (1:80), anti‐myeloperoxidase (MPO) antibodies, and anti‐DNase antibodies. The elevated p‐ANCA raised concerns for granulomatosis with polyangiitis (GPA). However, imaging studies demonstrated no pulmonary cavities or nodules. Due to the elevated anti‐DNase antibodies suggestive of HIAV, he was switched from 100 mg of hydralazine three times daily to nifedipine and discharged after a course of IV antibiotics.
Shortly thereafter, he was readmitted to an OSH for potential sepsis and skin lesions. Purpuric papules, plaques, and nodules on forehead, head, arms, and feet were noted on physical exam. Initially treated as disseminated herpes zoster with valacyclovir, lumbar puncture and serological workup were negative for VZV, HSV, monkeypox, cryptococcus, syphilis, and HIV. The patient was switched to doxycycline and prednisone. A dermatology follow‐up two months later revealed no active lesions, and a biopsy showed a reparative reaction.
Months later, he was readmitted to an OSH for suspected pneumonia and an active GI bleed. Chest x‐ray revealed bilateral infiltrates consistent with pneumonia. Labs showed a hemoglobin of 30 g/L (Male: 140–170 g/L) [2], which was concerning for an active GI bleed. He was given IV vancomycin and piperacillin‐tazobactam for the pneumonia and transferred to our hospital for management of the GI bleed. Due to limited medical record access from OSH, he was inadvertently restarted on hydralazine. Within 24 h, areas of desquamation from previously healing lesions developed violaceous, edematous bullae on the face and purpuric nodules and plaques on the hands and legs, along with significant facial edema and fever. During this hospitalization, he also developed metabolic encephalopathy, sepsis, and acute hypoxic failure.
A skin biopsy specimen revealed a subepidermal blister, epidermal necrosis, neutrophilic infiltrate, and ovoid structures resembling Cryptococcus (Figure 1). GMS stains (Figure 2) and Diastase Chromic Acid Schiff (DCAS) stains were negative. These histological findings, combined with the patient's clinical history, suggested a diagnosis of CSS in the setting of HIAV. Hydralazine was discontinued, and high‐dose corticosteroids were administered, leading to rapid improvement in his symptoms.
(A and B) Cryptococcoid sweet syndrome. Skin biopsy demonstrating dense infiltration of neutrophils, cellular debris, and numerous basophilic ovoid structures with clear spaces resembling yeast forms (black arrows). (H&E stain, ×20, ×40).
(A, B) Cryptococcoid sweet syndrome. Grocott/Gomori methenamine silver GMS stains of skin biopsy specimen were negative for the ovoid structures at ×10 (2A) and ×40 (2B) magnification.
Discussion
3
Historically, a diagnosis of SS required two major criteria: sudden onset of painful erythematous plaques/nodules and dense neutrophilic infiltrates without evidence of leukocytoclastic vasculitis in histology [1]. However, recent studies propose that vasculitis can occur secondarily to Malone et al. hypothesized that small vessel damage occurs after prolonged exposure to toxic byproducts released by activated neutrophils [3]. Consequently, vasculitic changes on histology should not preclude an SS diagnosis. The specific diagnostic criteria for SS are outlined in Table 1. In addition to both major criteria, the patient was documented to have had at least three of the four minor criteria during his admissions as well (Table 1). Further, the patient had positive p‐ANCA and anti‐MPO antibodies, negative ANA, and rapid deterioration of his vasculitic‐like lesions following hydralazine administration which supports a diagnosis of HIAV. Moreover, the incidence of HIAV is dose dependent [4]. This patient was on 100 mg TID for several years, further strengthening this diagnosis.
TABLE 1: Diagnostic criteria for sweet syndrome a .
Given the unusual histopathologic findings in CSS, an expanded differential diagnosis is necessary to enhance diagnostic accuracy. Infectious mimics such as true cryptococcosis, candidiasis, and Pityrosporum infection should be considered, particularly in immunocompromised patients or those with comorbid conditions [5]. Other neutrophilic dermatoses, such as pyoderma gangrenosum, bowel‐associated dermatosis‐arthritis syndromes, subcorneal pustulosis, and erythema elevatum diutinum must be considered in patients with ambiguous or atypical presentations [6]. Additionally, due to the clinical overlap, vasculitides like eosinophilic granulomatosis with polyangiits and GPA must be considered [7]. In the setting of underlying infection, as seen in this patient, antibiotic‐induced vasculitis, such as erythema multiforme or erythema nodosum could be on the differential as well [8]. A few reports have described dermatologic manifestations of CSS emerging around the time of antibiotic initiation, particularly vancomycin and piperacillin‐tazobactam, both of which were used in this patient [9]. Although these reports could not definitively determine whether their CSS was triggered by systemic inflammation or represented a drug reaction, Volonté et al. noted the temporal association with antibiotic administration [9]. These mimickers reinforce the importance of accurate history taking, correlating clinicopathologic features, and maintaining a broad differential when evaluating atypical dermal neutrophilic infiltrates.
In the absence of infection, the basophilic acellular bodies seen in CSS are hypothesized to be degrading neutrophils undergoing autolysis and apoptosis [10]. The reason why these cryptococcoid structures form remains elusive. However, there are commonalities among reported cases of CSS. In Table 2, we summarize these findings from 22 documented cases of CSS identified through a PubMed search using the keywords “cryptococcoid,” “Sweet syndrome and vasculitis,” and “Sweet syndrome and Cryptococcus.” Notably, most patients with CSS had one or more of the following comorbidities: underlying malignancy, chronic kidney disease, lung disease, and/or active cocaine use. Among the cases that reported serologic testing, all patients had at least one positive autoantibody. Most frequently, multiple autoantibodies were present.
Importantly, not all patients with CSS exhibited concomitant vasculitis. In those who did, vasculitis was frequently found in patients who had a history of taking hydralazine and/or had recently been given piperacillin‐tazobactam and/or vancomycin in the setting of a pneumonia. These patients commonly showed poor response to antibiotics alone, progressing instead to the development of skin lesions and respiratory failure. Timely initiation of systemic corticosteroids was consistently associated with clinical improvement, both in terms of cutaneous findings and respiratory status. Nevertheless, a few patients failed to respond to treatment and died during their hospitalization.
Although previously reported cases of CSS share several clinical features, to our knowledge, this is the first documented case of CSS with concomitant vasculitis demonstrating both SS‐associated pulmonary and neurologic manifestations. Classic pulmonary manifestations of SS include bilateral infiltrates and pleural effusion imitating pneumonia [24], while neurological manifestations (Neuro‐Sweet disease) include encephalitis and meningitis [25]. We hypothesize that this patient's encephalopathy and respiratory failure may have been exacerbated by CSS.
Systemic corticosteroids and termination of hydralazine effectively improved the patient's condition. Hydralazine was added to his allergy list to prevent future exposure.
Future research of CSS should focus on elucidating its etiology and determining if CSS represents a distinct entity or is merely a histopathologic reaction to systemic stressors. Additionally, outcomes should be compared between individuals with histologic findings of classic SS to those with CSS to determine whether one variant is associated with a worse prognosis.
Author Contributions
J.V. was the primary author of the manuscript. P.S., K.L., A.E., and L.W. played instrumental roles in drafting and revising the manuscript.
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. S. Heath and A. G. Ortega‐Loayza , “Insights Into the Pathogenesis of Sweet's Syndrome,” Frontiers in Immunology 10 (2019): 414.30930894 10.3389/fimmu.2019.00414 PMC 6424218 · doi ↗ · pubmed ↗
- 2American College of Physicians , “Laboratory Values,” accessed, April 20, 2024, https://annualmeeting.acponline.org/sites/default/files/shared/documents/for‐meeting‐attendees/normal‐lab‐values.pdf.
- 3J. C. Malone , S. P. Slone , and L. A. Wills‐Frank , “Vascular Inflammation (Vasculitis) in Sweet Syndrome,” Archives of Dermatology 138, no. 3 (2002): 345–349.11902985 10.1001/archderm.138.3.345 · doi ↗ · pubmed ↗
- 4D. Alawneh and A. Edrees , “Hydralazine‐Induced Antineutrophil Cytoplasmic Antibody (ANCA)‐Associated Vasculitis: A Case Report and Literature Review,” Cureus 14, no. 4 (2022): e 24132.35573557 10.7759/cureus.24132 PMC 9106538 · doi ↗ · pubmed ↗
- 5R. Veerappan , L. E. Miller , C. Sosinski , and G. A. Youngberg , “Narrow‐Spectrum Staining Pattern of Pityrosporum,” Journal of Cutaneous Pathology 33, no. 11 (2006): 731–734.17083692 10.1111/j.1600-0560.2006.00537.x · doi ↗ · pubmed ↗
- 6D. Soutou , O. Vignon‐Pennamen , and O. Chosidow , “Les Dermatoses Neutrophiliques,” La Revue de Médecine Interne 32, no. 5 (2011): 306–313.20933309 10.1016/j.revmed.2010.08.023 · doi ↗ · pubmed ↗
- 7E. S. Tabb , L. M. Duncan , and R. M. Nazarian , “Eosinophilic Granulomatosis With Polyangiitis: Cutaneous Clinical and Histopathologic Differential Diagnosis,” Journal of Cutaneous Pathology 48, no. 11 (2021): 1379–1386.34019312 10.1111/cup.14065 · doi ↗ · pubmed ↗
- 8P. N. Arora , “Cutaneous Vasculitis,” Medical Journal, Armed Forces India 50 (1994): 283–290.28790566 10.1016/S 0377-1237(17)31088-2PMC 5533149 · doi ↗ · pubmed ↗