Salvage Mini-Open Achilles Tendon Repair Using the Percutaneous Achilles Repair System (PARS): A Technical Tip
Sarah Oyadomari, Andrew R Hsu, Naudereh Noori

TL;DR
This paper describes a salvage technique for repairing Achilles tendon ruptures when minimally invasive methods fail.
Contribution
A novel salvage mini-open technique is introduced to avoid full open surgery in complex Achilles tendon cases.
Findings
Percutaneous methods sometimes fail to capture the proximal tendon stump effectively.
The proposed salvage technique uses mini-open incisions to repair complex tears without full open surgery.
Abstract
Minimally invasive surgical repair options for mid-substance Achilles tendon ruptures may pose some limitations in regard to complex tear patterns or poor overall tendon quality. We have encountered cases where percutaneously passed sutures with the help of a targeting device fail to adequately capture the proximal tendon stump. In this technical report, we report a salvage technique for such cases that prevents the need for conversion to an extensile open approach, relying on smaller mini-open incisions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
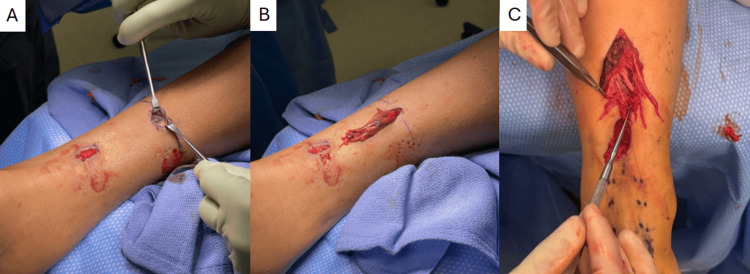 Figure 1
Figure 1 Figure 2
Figure 2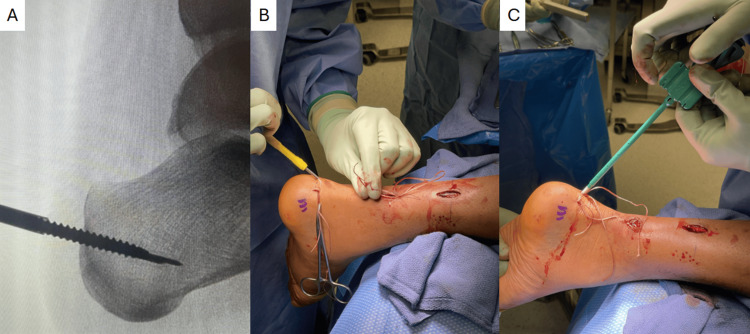 Figure 3
Figure 3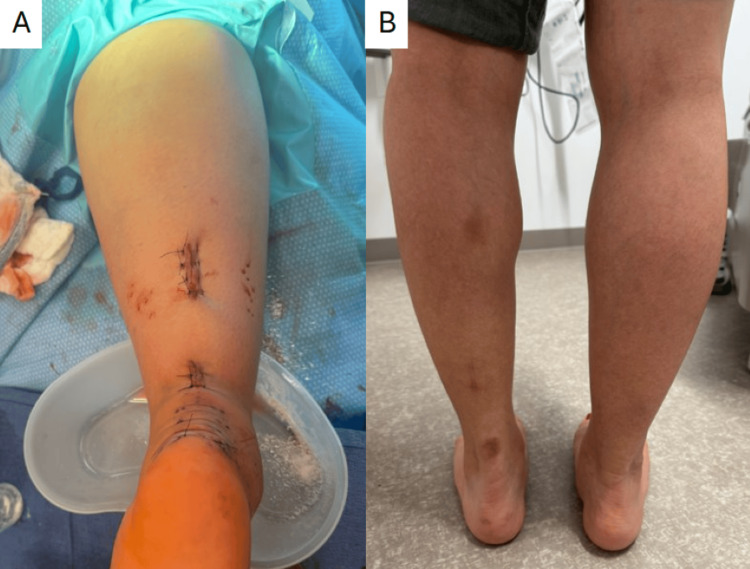 Figure 4
Figure 4| Postoperative Time | Activity Restriction |
| Weeks 0-2 | Non-weight-bearing in plantarflexion splint |
| Weeks 2-4 | Non-weightbearing in CAM boot with heel lifts, dorsiflexion to neutral |
| Weeks 4-6 | Progressive weightbearing and removal of lifts in the CAM boot, isometric calf exercises |
| Weeks 6-8 | Weightbearing as tolerated in CAM boot, no dorsiflexion past neutral, graduated resistance exercises |
| Weeks 8-12 | Wean into regular shoes, bilateral calf raises while seated, passive stretching, and continue with no dorsiflexion past neutral |
| Weeks 12-16 | Plyometric training, single-leg raises, jogging, full range of motion without restriction |
| Months 6-8 | Consider full running, agility, jumping with progressive return to sport |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTendon Structure and Treatment · Shoulder Injury and Treatment · Foot and Ankle Surgery
Introduction
Achilles tendon ruptures are a common athletic injury occurring in 2.1 per 100,000 person-years, with a growing incidence in active older individuals [1,2]. Minimally invasive surgical options have evolved to mitigate the complications from traditional open surgical repairs, which disrupt local biology and carry the risk of greater wound complications [3,4]. The Percutaneous Achilles Repair System (PARS, Arthrex Inc., Naples, FL, USA) is one example of a commonly used minimally invasive technique to repair mid-substance Achilles tendon ruptures [5]. However, if the proximal tendon stump has complex multiplanar tears or poor tendon quality, the repair sutures passed with the PARS jig may have insufficient purchase and pull through. In these situations, conversion to an extensile open approach is often performed to visualize and capture a greater extent of the damaged tendon; however, the authors have successfully devised an alternative, less invasive mini-open salvage technique detailed here.
Technical report
The patient is positioned prone on the operating table. A thigh tourniquet is used, and an approximately 2 cm incision is planned at the palpable defect. A longitudinal or transverse incision can be used. The PARS jig is used as described [5] to pass the repair sutures, which, when cycled, may pull through the tendon. This may be due to improper positioning of the jig, so it is advised to try multiple attempts. With persistent pull-through of the sutures, poor proximal tendon quality or complex tearing is likely the cause.
A mini-open 2-3 cm longitudinal counter incision is made proximal to the initial incision, leaving at least a 3 cm skin bridge (Figure 1). Of note, the summation of the counter incision and initial incision is smaller than the extensile extension needed to allow access to the same area of the proximal tendon. In some instances, the paratenon is ruptured at this region; in cases where it is not, an incision is made through the paratenon to access the tendon. The proximal tendon stump is then tunneled retrograde from the distal incision out of the proximal one (Figure 1). Figure 1 shows two examples of poor tendon quality with a coronal delamination and fraying with multiple longitudinal splits, both of which can account for the inability of the PARS jig to capture the tendon fully.
Counter incision (proximal) with intact paratenon exposed (A). Proximal tendon stump tunneled through showing evidence of delamination (B) and extensive fraying with longitudinal tears (C).
A four-strand repair is completed with 1.3 mm SutureTape (Arthrex Inc., Naples, FL, USA) using a core weave (Figure 2) or Krackow repair technique. All sutures are cycled 10 times to remove creep and ensure tendon purchase. The suture ends and the proximal tendon stump are tunneled anterograde through the distal incision, preserving any remaining paratenon.
Four-strand repair with suture tape using a core weave pattern with good purchase.
The remainder of the case can be completed using a PARS-to-PARS (suture-to-suture) repair or a PARS-SpeedBridge (suture to calcaneal suture anchor; Arthrex Inc., Naples, FL, USA) repair, using the four-strand repair suture limbs in place of the ones passed with the PARS jig. It is our preference to use a PARS-SpeedBridge approach, especially in cases of poor tendon quality, in order to obtain direct tendon-to-bone fixation, bypassing suture knots and bulk in the area of the primary rupture. Anchors are drilled and tapped along the insertion of the Achilles tendon under fluoroscopic guidance before passing the suture through the distal stump and seating the anchors with the ankle in maximal plantarflexion (Figure 3). The paratenon is carefully closed in both the proximal and distal incisions to assist with vascular restoration and tendon healing. The postoperative course is the same as that of other patients at our institution undergoing PARS-SpeedBridge Achilles tendon repair (Table 1), with no additional restrictions. An example of the intraoperative closure and subsequent healed incisions for our technique is shown in Figure 4.
Appropriate positioning of calcaneal anchors confirmed on fluoroscopy (A), followed by tunneling through the distal stump (B) and insertion of anchors (C).
Intraoperative closure (A) and healed incisions one-year postoperatively (B).
Discussion
This mini-open conversion technique is ideal for salvaging cases of Achilles tendon rupture in which the PARS jig fails due to suture pull-out through poor-quality tendon. Many patients have pre-existing Achilles tendinosis, resulting in more fibrotic and scarred tissue that is not as robust and may lead to more shredding upon injury. One study found that up to 77% of patients showed evidence of preceding Achilles tendinosis at the rupture site [6].
Other contributors to suture pull-out include more complex tear morphology. In one study’s cohort, most mid-substance ruptures were found to be transverse; however, 10% of cases were found to have a more involved pattern, including coronal splits resulting in double-layers or Z-shaped ruptures [7]. The PARS jig is difficult to apply to tendons with these non-transverse rupture patterns, as the prongs may slip through the multiple layers, and passing needles may push aside rather than pierce the tissue.
The core weave stitch reduces the bulk of suture material on the tendon surface and has no significant difference in load to failure when compared with a Krackow stitch [8]. We have had success with both stitch techniques.
Conclusions
Overall, minimally invasive Achilles repair techniques such as PARS-to-PARS and PARS-Speedbridge offer several advantages, such as decreased wound complications and faster return to baseline activities compared with traditional open techniques. However, not all Achilles ruptures are amenable to the use of the PARS technique. The conversion technique described here has been performed in multiple cases where previously unrealized poor-quality tendon has been encountered, preventing the need for conversion to an extensile open repair.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Achilles tendinopathy Stat Pearls [Internet] Medina Pabón MA Naqvi U Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 538149/30844176 · pubmed ↗
- 2Achilles tendon injuries Curr Rev Musculoskelet Med Egger AC Berkowitz MJ 72801020172819463810.1007/s 12178-017-9386-7PMC 5344857 · doi ↗ · pubmed ↗
- 3Outcomes and complications of open versus minimally invasive repair of acute Achilles tendon ruptures: a systematic review and meta-analysis of randomized controlled trials Am J Sports Med Attia AK Mahmoud K d'Hooghe P Bariteau J Labib SA Myerson MS 8258365120233490849910.1177/03635465211053619 · doi ↗ · pubmed ↗
- 4Clinical outcomes and complications of percutaneous Achilles repair system versus open technique for acute Achilles tendon ruptures Foot Ankle Int Hsu AR Jones CP Cohen BE Davis WH Ellington JK Anderson RB 127912863620152605525910.1177/1071100715589632 · doi ↗ · pubmed ↗
- 5Minimally invasive mid-substance Achilles tendon repair using the percutaneous Achilles repair system (PARS)JBJS Essent Surg Tech Martin KD Crouser NJ Khan IA 012202210.2106/JBJS.ST.21.00050 PMC 993103736816527 · doi ↗ · pubmed ↗
- 6Achilles tendinosis does not always precede Achilles tendon rupture Knee Surg Sports Traumatol Arthrosc Park YH Kim TJ Choi GW Kim HJ 329733032720193026718410.1007/s 00167-018-5172-3 · doi ↗ · pubmed ↗
- 7Morphology of acute Achilles tendon rupture by intraoperative evaluation J Foot Ankle Surg Kage T Sanada T Iwaso H 119812036020213413491810.1053/j.jfas.2021.05.005 · doi ↗ · pubmed ↗
- 8Core weave versus Krackow technique for Achilles tendon repair: a biomechanical study Foot Ankle Int Hong Y Hermida L White KL Parks BG Camire LM Guyton C 110711103120102118921310.3113/FAI.2010.1107 · doi ↗ · pubmed ↗