Malignant hilar biliary obstruction with active biliary bleeding: fully covered multi-hole metal stent deployed above papilla
Tsuyoshi Suda, Norihiko Ogawa, Yoshihide Naito, Kenkei Hasatani, Hiroyuki Aoyagi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
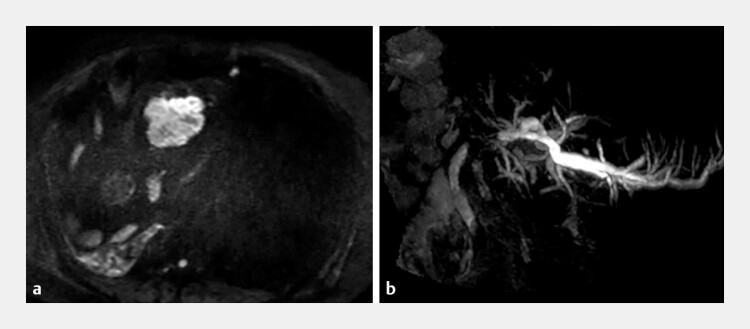 Fig. 1
Fig. 1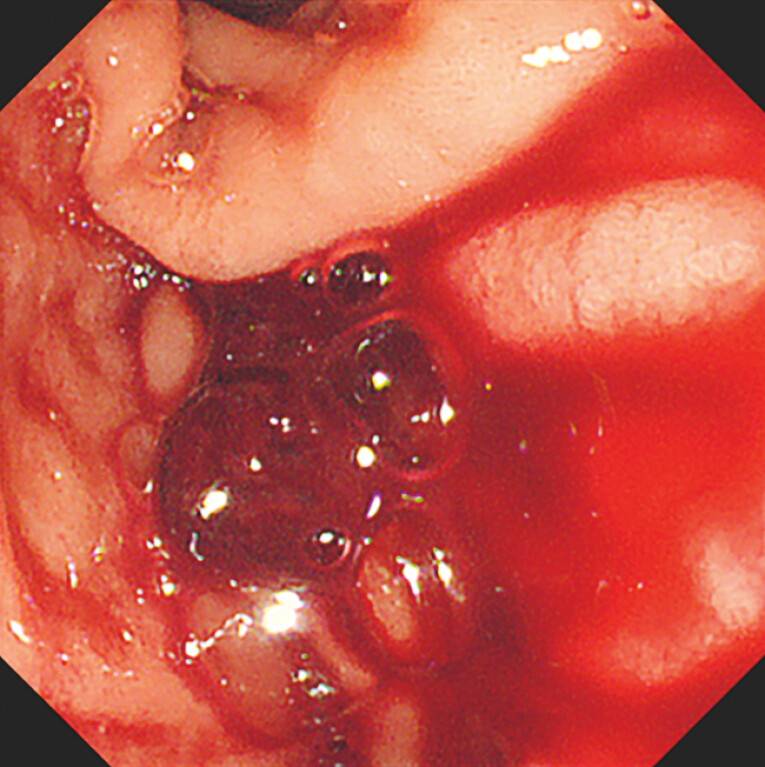 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4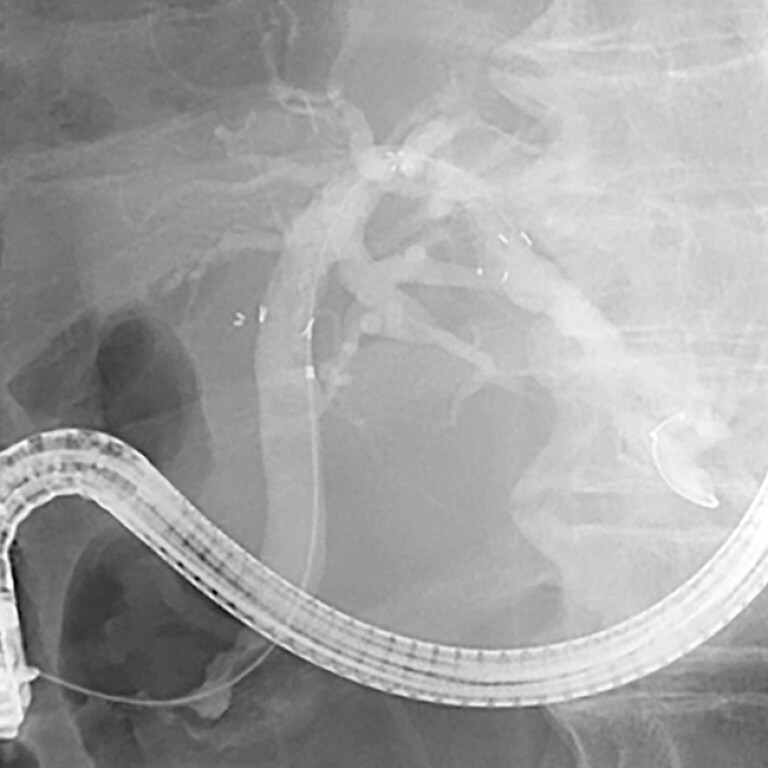 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Cholangiocarcinoma and Gallbladder Cancer Studies · Pediatric Hepatobiliary Diseases and Treatments
In patients with malignant hilar biliary obstruction (MHBO), uncovered self-expandable metal stents (SEMSs) are generally not removable, and fully covered SEMSs (FCSEMSs) have the risk of occluding segmental bile ducts 1 . The newly developed multi-hole FCSEMS reduces this occlusion risk, and an increasing number of reports now support its use for MHBO 2 3 .
A 55-year-old man underwent multidisciplinary treatment for rectal cancer, including right hepatic lobectomy and local resection of multiple liver metastases. Subsequently, he developed left hepatic duct stenosis caused by a segment 1 liver metastasis ( Fig. 1 ), for which a plastic biliary stent was placed. However, the stent became occluded, and an endoscopic retrograde cholangiopancreatography (ERCP) attempt at the referral hospital was unsuccessful; therefore, the patient was transferred to our institution.
MRCP reveals a metastatic liver tumor in segment 1 a and left hepatic duct stenosis b . MRCP, magnetic resonance cholangiopancreatography.
At our hospital, a repeat ERCP revealed active bleeding from the tumor ( Fig. 2 ). Because the patient had renal failure, contrast-enhanced computed tomography and magnetic resonance imaging could not be performed, making the preprocedural identification of bleeding difficult. Endoscopic retrograde cholangiography (ERC) showed malignant stenosis of the left hepatic duct owing to tumor involvement ( Fig. 3 ). To decompress the MHBO and control hemobilia, we planned the placement of an FCSEMS. To avoid occluding the segmental ducts, a 10-mm × 8-cm multi-hole FCSEMS (HANARO Biliary Multi-Hole NEO; M.I. Tech Co., Ltd, Pyeongtaek, South Korea) was deployed above the papilla. After the placement of the multi-hole FCSEMS, ERC revealed the segmental ducts without occlusion ( Fig. 4 and Fig. 5 and Video 1 ).
Hemobilia with active bleeding.
Left hepatic duct stenosis in ERC. ERC, endoscopic retrograde cholangiography.
Multi-hole FCSEMS deployed. FCSEMS, fully covered self-expandable metal stents.
Branches of the bile duct are visualized via multi-hole FCSEMS in ERC. ERC, endoscopic retrograde cholangiography; FCSEMS, fully covered self-expandable metal stents.
Multi-hole FCSEMS reduces the risk of occluding segmental bile ducts in MHBO. FCSEMS, fully covered self-expandable metal stents; MHBO, malignant hilar biliary obstruction.Video 1
Jaundice gradually improved after stent placement. Although hemobilia persisted briefly and necessitated a transfusion, the bleeding resolved upon the complete stent expansion. Approximately 2 weeks after the procedure, the patient was transferred back to the referring hospital.
Successful hemostasis has been reported in a patient with MHBO-related hemobilia through the side-by-side placement of a multi-hole FCSEMS across the papilla 4 . Although there are some concerns regarding the multi-hole design of the FCSEMS, previous studies have reported successful removal 5 .
The multi-hole FCSEMS may therefore serve not only as a novel treatment option for MHBO but also as an effective modality for managing biliary bleeding.
Endoscopy_UCTN_Code_CCL_1AZ_2AC Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Tringali A Papanikolaou IS Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline – Updated October 2017 Endoscopy 20185091093030086596 10.1055/a-0659-9864 · doi ↗ · pubmed ↗
- 2Takahashi S Fujisawa T Takasaki Y Side-by-side placement of a novel slim 6-mm multi-hole covered self-expandable metallic stent for malignant hilar biliary obstruction Endoscopy 202557 E 312E 31310.1055/a-2569-758240233932 PMC 12020676 · doi ↗ · pubmed ↗
- 3Toyonaga H Oka A Takayama T Triple stent-in-stent placement of novel 6-mm multi-hole covered self-expandable metal stents for malignant hilar biliary obstruction Endoscopy 202557 E 808E 81010.1055/a-2641-220440719127 PMC 12302166 · doi ↗ · pubmed ↗
- 4Oishi R Miwa H Maeda S Unique side-by-side technique for malignant hilar biliary obstruction using novel multi-hole self-expandable metallic stents Dig Endosc 202510.1111/den.7001440865927 · doi ↗ · pubmed ↗
- 5Ogura T Uba Y Kanadani T Reintervention for recurrent biliary obstruction after stent-in-stent deployment of multi-hole self-expandable metal stents Endoscopy 202557 E 181E 18210.1055/a-2534-314339978392 PMC 11842147 · doi ↗ · pubmed ↗