Novel bidirectional traction technique for tension-regulated large defect closure: a case report
Weixing Yang, Tao Hao, Xiaowei Tang, Xiaolin Zhong, Hao Li, Muhan Lü

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
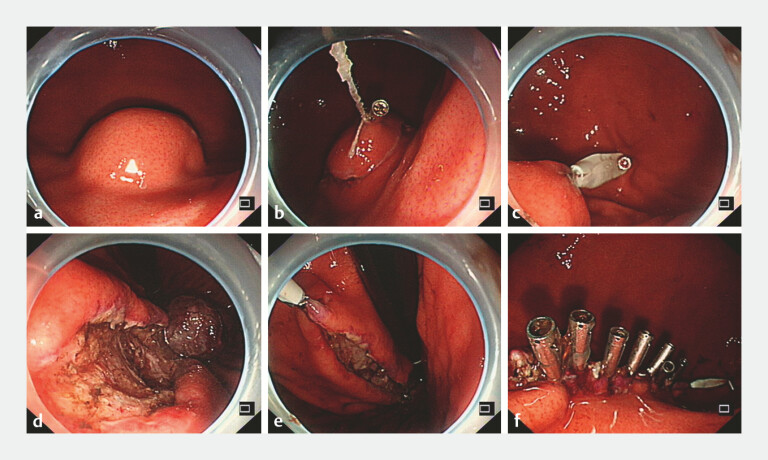 Fig. 1
Fig. 1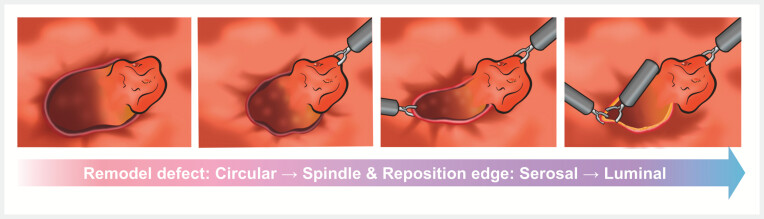 Fig. 2
Fig. 2- —Sichuan Medical Science and Technology Innovation Research Association
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntegrated Circuits and Semiconductor Failure Analysis · Microstructure and mechanical properties · Mechanical Failure Analysis and Simulation
Endoscopic submucosal dissection (ESD) for large mucosal defects presents a critical challenge in achieving secure closure, a factor that significantly influences postoperative recovery and clinical outcomes 1 . Although several techniques have been developed to facilitate defect closure, such as the clip-with-line method and the overstitch endoscopic suturing system, the management of extensive defects remains hampered by technical complexity, substantial financial cost, and notable postoperative risks 2 3 . Herein, a novel traction-assisted technique was designed to achieve reliable mucosal apposition under technically demanding conditions ( Video 1 ).
The steps for defect closure using the novel strategy.Video 1
A 62-year-old woman with a 2.7 × 2.1 cm gastrointestinal stromal tumor located on the posterior gastric wall underwent en bloc ESD. The resulting defect measured approximately 5 × 4 cm with a near-circular configuration ( Fig. 1 a ). Given the extensive size and suspected full-thickness involvement, direct closure using conventional metallic clips was deemed unfeasible. An innovative stepwise closure strategy was therefore employed.
Endoscopic views demonstrating the novel bidirectional traction technique for the closure of a large post-ESD defect. a A 2.7 × 2.1 cm gastrointestinal stromal tumor was located on the posterior gastric wall. b The oral-traction point was established by grasping and anchoring a preserved tumor fragment to the proximal mucosa with a clip. c Anal counter-traction was applied to minimize tissue inversion. d, e The defect was sequentially reconfigured into a spindle shape and closed along the long axis with metallic clips. f The complete linear apposition of the mucosal edges. ESD, endoscopic submucosal dissection.
Step 1: Establishment of the oral traction point: Rather than completing full resection, a portion of the tumor at the oral side was deliberately preserved to serve as a native traction anchor. This was grasped and fixed to normal mucosa oral to the defect using a clip, generating sustained oral-directed vector forces to tension the edge ( Fig. 1 b, c ).
Step 2: Establishment of the anal-traction point: On the anal side of the defect, internal traction was applied by grasping the mucosal edge and exerting a force in the anal and luminal directions. This maneuver generated effective counter-traction, thereby maintaining adequate tissue tension and minimizing undesirable outward inversion (everting towards the serosal side) of the mucosal margin ( Fig. 1 d, e ).
Step 3: Sequential linear closure: Through these bidirectional forces, the originally circular defect was geometrically reconfigured into a spindle-shaped defect with reduced circumference and well-opposed edges, preventing tissue inversion ( Fig. 1 f ). Using metallic clips, sequential closure was performed from one apex along the long axis of the reconfigured defect, resulting in linear apposition without the suture material.
As illustrated in the schematic ( Fig. 2 ), this technique utilizes purposeful traction anchors and controlled bidirectional forces to actively remodel the defect into a geometry amenable to efficient closure. This approach addresses two fundamental issues: (1) linearization reduces the defect circumference and tension, facilitating clips placement; (2) traction-assisted edge alignment minimizes tissue inversion, thereby reducing the risk of improper healing and delayed perforation. Relying solely on conventional metallic clips, this method is both technically accessible and cost-effective. It offers a promising new strategy for managing challenging post-ESD defects.
A schematic diagram of the bidirectional traction technique.
Endoscopy_UCTN_Code_TTT_1AO_2AO
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferlitsch M Hassan C Bisschops R Colorectal polypectomy and endoscopic mucosal resection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2024 Endoscopy 20245651654510.1055/a-2304-321938670139 · doi ↗ · pubmed ↗
- 2Xu J Yang W Wang Z An innovative approach to close large mucosal defects post-endoscopic submucosal sissection: threads combined with endoclips Endoscopy 20255701 E 202E 20340032269 10.1055/a-2535-1748 PMC 11875755 · doi ↗ · pubmed ↗
- 3Masunaga T Sasaki M Murata S Feasibility of modified double-layered suturing for a large mucosal defect after duodenal endoscopic submucosal dissection (origami method)Endoscopy 20255747848310.1055/a-2463-720439510530 · doi ↗ · pubmed ↗