Risk Factor Control in a Portuguese Vascular Risk Clinic: A 16-Month Retrospective Cohort Study
Cristiano Gante, Stanislav Tsisar, Ana Catarina Reis, Mario Rodrigues, Mariana Salvado de Morais, Luís R Almeida, Luis Dias

TL;DR
A Portuguese vascular risk clinic showed improved blood pressure and diabetes control in high-risk patients over 16 months.
Contribution
The study provides updated insights into cardiovascular risk factor management in a specialized clinic compared to earlier data.
Findings
76% of patients achieved blood pressure control according to European Society of Cardiology targets.
Glycated hemoglobin levels improved compared to a decade earlier, with increased use of newer antidiabetic agents.
Statin-based therapies were the mainstay for dyslipidemia, often combined with ezetimibe.
Abstract
Background Cardiovascular diseases (CVDs) are the leading cause of morbidity and mortality worldwide and in Portugal. Stroke remains one of the principal causes of death in Portugal, increasing the urgency of efficient primary and secondary preventive strategies. Methods A retrospective cohort study was conducted, including 229 patients followed at a specialized vascular risk clinic between January 2022 and April 2023, corresponding to 820 outpatient visits. Electronic medical records were retrospectively reviewed, and an anonymized database was created to collect demographic data, referral origin, cardiovascular risk factors, therapeutic management, and risk factor control. Recorded variables included age, sex, number of consultations, blood pressure, body mass index, lipid profile, fasting glucose, and glycated hemoglobin. Patients were classified into primary or secondary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
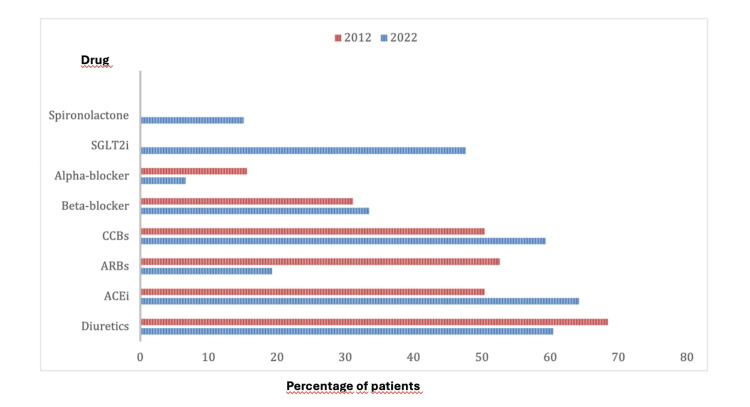 Figure 1
Figure 1| Categories | Values |
| Total patients | 229 (57% male) |
| Mean age | 70.5 (38-103) years |
| Secondary prevention | 76% (n=175) |
| High/very high CV risk | 96% |
| Risk factors | Values |
| Dyslipidemia | 93.9% |
| Hypertension | 92.6% |
| Diabetes mellitus | 63.3% |
| ≥3 risk factors | 68.9% |
| Parameters | Values |
| Essential hypertension | 97.6% |
| Mean BP | SBP: 131.7 mmHg/DBP: 69.5 mmHg |
| BP controlled | 76% |
| ≥3 antihypertensives | 55% |
| Parameters | Values |
| Type 2 diabetes | 94% |
| Mean HbA1c | 6.6% |
| HbA1c ≤7% | 65% |
| Insulin therapy | 33% |
| Metformin use | 91% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLipoproteins and Cardiovascular Health · Blood Pressure and Hypertension Studies · Acute Ischemic Stroke Management
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death globally, responsible for an estimated 19.8 million deaths in 2022, approximately 32% of all global mortality, with heart attacks and strokes accounting for 85% of these deaths [1]. In Europe, CVDs account for about 42.5% of all deaths, representing the highest regional burden globally [2]. Stroke and ischemic events contribute substantially to this mortality.
In Portugal, CVD continues to be a primary cause of mortality, particularly among older adults, with stroke among the principal contributors to death. National cardiology societies and health authorities emphasize the need for strengthened risk stratification and management as part of a national cardiovascular health strategy [3].
The main behavioral risk factors, unhealthy diet, physical inactivity, tobacco use, and harmful alcohol consumption, typically lead to intermediate risk factors, including hypertension, hyperglycemia, dyslipidemia, overweight, and obesity. These factors are measurable in primary care and strongly predict future cardiovascular events [1]. In accordance with these contributors, the pathophysiology of atherosclerotic disease involves endothelial dysfunction, chronic inflammation, lipid accumulation within the arterial intima, and plaque formation. Subsequent plaque instability or rupture can precipitate ischemic events in both the heart and cerebral circulation [4].
Despite substantial advances in cardiovascular risk stratification and pharmacological management over the past decade, real‑world data describing contemporary patterns of risk factor control and their evolution in high‑risk outpatient populations remain limited. This study aimed to characterize current cardiovascular risk profiles, management strategies, and risk factor control in a specialized vascular risk clinic and to compare these findings with institutional data from a decade earlier.
Materials and methods
Study design
This was a retrospective cohort study conducted at a specialized vascular risk outpatient clinic. Clinical data were obtained through the retrospective review of electronic medical records of patients attending the clinic between January 2022 and April 2023. During this period, a total of 229 patients were evaluated, accounting for 820 outpatient visits. A dedicated database was created for the purpose of this study to systematically record and analyze the collected variables.
Patient recruitment
All consecutive adult patients who attended the vascular risk clinic during the study period were eligible for inclusion. Patients were followed within the context of routine clinical care, either referred from primary care or other hospital specialties. No additional interventions or visits were performed for research purposes. Patients were subsequently classified into primary or secondary cardiovascular prevention groups based on the presence or absence of established cardiovascular disease, according to standard clinical definitions.
Data collection
Clinical records were reviewed retrospectively, and a structured Microsoft Excel (Redmond, WA: Microsoft Corp.) database was developed to collect anonymized patient-level data. Variables recorded included demographic characteristics (age and sex), healthcare utilization data (number of consultations per year and number of vascular risk clinic visits), and referral origin.
Cardiovascular risk factors were systematically assessed, with a specific focus on hypertension, diabetes mellitus, dyslipidemia, obesity, and smoking status. For each risk factor, information regarding targeted pharmacological therapy and adequacy of control was recorded. Blood pressure measurements obtained during clinic visits were used to assess hypertension control. Anthropometric data, including weight and body mass index (BMI), were collected when available.
Laboratory parameters were retrieved from electronic records, including low-density lipoprotein cholesterol (LDL-C), triglycerides, fasting plasma glucose, and glycated hemoglobin (HbA1c). These values were used to evaluate metabolic control according to contemporary clinical practice standards.
Patients classified under primary prevention were further stratified using cardiovascular risk estimation tools. Systematic Coronary Risk Evaluation 2 (SCORE2) was applied to patients aged 70 years or younger, while Systematic Coronary Risk Evaluation 2-Older Persons (SCORE2-OP) was used for patients aged 70 years or older [5,6]. These risk calculators are freely accessible tools, and the original validation studies will be cited accordingly.
Statistical analysis
The statistical analysis was primarily descriptive, aimed at characterizing the study population and current patterns of cardiovascular risk factor management. Continuous variables were summarized using means and standard deviations or medians and interquartile ranges, as appropriate, while categorical variables were presented as absolute numbers and percentages.
To contextualize the findings within an evolutionary perspective, selected variables were compared with data from an internal institutional study conducted between 2011 and 2012. This comparison focused on patterns of antihypertensive therapy use and on glycemic control, assessed by glycated hemoglobin (HbA1c) levels, to evaluate changes in clinical practice and risk factor management over the past decade.
Results
A total of 229 patients were included in the study, of whom 131 (57%) were male, and 98 (43%) were female (Table 1). The mean age of the study population was 70.5 years (range: 38-103 years). Most patients were referred from inpatient hospitalization (35%) or other outpatient specialty clinics (31%), with additional referrals from primary healthcare services (22%) and the emergency department (12%).
The primary reasons for referral to the vascular risk clinic were major cardiovascular risk factors and established target organ damage. Most patients (n=175, 76%) were evaluated in the context of secondary prevention, with cerebrovascular events (stroke or transient ischemic attack) accounting for 108 cases and ischemic heart disease (acute myocardial infarction or angina) in 30 patients. Chronic kidney disease (CKD) and peripheral arterial disease contributed to 73 and four referrals, respectively, while multiple concomitant risk factors were the main reason for referral in 20 patients. On primary prevention grounds, diabetes was the most frequent cause (37 referrals), followed by hypertension (17 referrals) and dyslipidemia (eight referrals). The overall prevalence of risk factors is described in Table 2.
Arterial hypertension
A total of 212 patients had hypertension, including five cases (2%) of secondary hypertension due to primary hyperaldosteronism. The majority of patients required combination therapy, most commonly three antihypertensive drugs. Mean systolic and diastolic blood pressures were 131.7 mmHg (range: 85-190 mmHg) and 69.5 mmHg (range: 44-100 mmHg), respectively (Table 3). According to the European Society of Cardiology (ESC) criteria, 162 patients (76%) achieved blood pressure control, whereas 98 patients (46%) met the American Heart Association definition [7]. Among the 24% of patients not achieving ESC targets, many were older than 75 years (n=25), had advanced CKD (estimated glomerular filtration rate {eGFR} <30 mL/min/1.73 m^2^), or demonstrated intolerance to antihypertensive therapy.
Comparing 2012 and 2022 prescribing patterns (Figure 1), ACE inhibitors increased from 50% to 64%, diuretics decreased from 68% to 60%, calcium channel blockers increased from 50% to 59%, angiotensin receptor blockers (ARBs) decreased from 53% to 19%, alpha-blockers declined from 16% to 7%, and beta-blocker use remained stable (31-34%). Notably, SGLT2 inhibitors and spironolactone were introduced more recently, reaching 48% and 15% of patients, respectively, by 2022.
Evolution of antihypertensive therapy prescribing patterns from 2012 to 2022.This bar chart compares the proportion of patients receiving different classes of antihypertensive medications in 2012 (first bar for each drug) and 2022 (second bar for each drug) among the study population. The y-axis lists the drug classes, including ACE inhibitors, diuretics, calcium channel blockers, angiotensin receptor blockers (ARBs), alpha-blockers, beta-blockers, SGLT2 inhibitors, and spironolactone. The x-axis represents the percentage of patients receiving each therapy. Results show an increase in ACE inhibitors (50% → 64%) and calcium channel blockers (50% → 59%), a decrease in ARBs (53% → 19%) and alpha-blockers (16% → 7%), a slight increase in beta-blockers (31% → 34%), and a reduction in diuretics (68% → 60%). Notably, newer agents such as SGLT2 inhibitors and spironolactone were introduced in 2022, used in 48% and 15% of patients, respectively. Data were collected retrospectively from electronic medical records, and the chart provides a descriptive comparison of prescribing trends over the past decade.
Diabetes mellitus
Diabetes was present in 145 patients (63%), 94% of whom had type 2 diabetes (Table 2). Most patients had comorbid conditions as follows: 130 with hypertension, 123 with dyslipidemia, and 112 were overweight. Thirty-eight patients were over 80 years, limiting intensive glycemic control due to hypoglycemia risk. The mean HbA1c was 6.6%, improved from 7.4% a decade earlier. Eleven patients (8%) had HbA1c between 8% and 9%, with only four under 65 years of age. Regarding therapy, 48 patients (33%) were on insulin (Table 4). Among oral agents, metformin was used in 91%, dapagliflozin in 47%, DPP-4 inhibitors in 43%, sulfonylureas in 32%, and GLP-1 receptor agonists in 29%, reflecting expanding use of newer agents despite prescription restrictions in Portugal.
Dyslipidemia
Dyslipidemia was present in 215 patients (94%), with 45 (21%) exhibiting mixed dyslipidemia with hypertriglyceridemia. Statin monotherapy was used in 107 patients (47%), predominantly rosuvastatin (63%) and atorvastatin (36%). Combination therapy with statin and ezetimibe was used in 87 patients (38%), triple therapy including fenofibrate in nine patients (4%), and statin plus fenofibrate in four patients (2%). Three patients (1%) were treated with ezetimibe alone. Five patients (2%) achieved targets through lifestyle alone or received bempedoic acid (0.4%) or PCSK9 inhibitors (0.8%) due to intolerance to oral agents.
Obesity and tobacco use
Overweight and obesity were common as follows: 72 patients (31%) were overweight (BMI: 25-29.9 kg/m^2^), 41 patients (18%) had class I obesity (BMI: 30-34.9 kg/m^2^), 21 patients (9%) had class II obesity (BMI: 35-39.9 kg/m^2^), and three patients (1%) had class III obesity (BMI: ≥40 kg/m^2^). Seventeen patients (7%) were current smokers, and 65 patients (28%) were former smokers. The mean smoking history was 45.9 pack-years.
Target organ damage
Target organ damage was frequent, influencing treatment strategies. Cerebrovascular disease affected 108 patients (47%), with 87% strokes and 13% transient ischemic attack (TIA). CKD was present in 73 patients (32%), including 30 patients (13%) with stage ≥3a according to the Kidney Disease: Improving Global Outcomes (KDIGO). Cardiac disease occurred in 30 patients (13%), with 77% of whom had experienced an acute myocardial infarction and 23% reporting angina.
Discussion
This cohort demonstrates a high burden of multiple cardiovascular risk factors, consistent with epidemiological data showing that nearly all patients with hypertension and diabetes present with concomitant risk factors, such as dyslipidemia, obesity, and hypertension [8,9]. The advanced mean age of 70.5 years underscores the importance of frailty, multimorbidity, and age‑related physiological changes in influencing treatment goals and tolerability.
Hypertension remains a key modifiable risk factor, with 76% of patients achieving ESC‑recommended targets. Nonetheless, individualized blood pressure goals are critical in older adults and frail patients to balance cardiovascular protection with the risk of hypotension and adverse events [10]. Changes in antihypertensive prescribing over the past decade, particularly the increased use of ACE inhibitors, CCBs, SGLT2 inhibitors, and spironolactone, reflect evolving guideline recommendations and emerging evidence for cardiovascular and renal protection [11].
Diabetes management shows improved glycemic control over the last decade (mean HbA1c 6.6%), despite the challenges of comorbidities, advanced age, and CKD. The increasing use of SGLT2 inhibitors and GLP‑1 receptor agonists highlights their role in high‑risk populations with multiple cardiometabolic comorbidities [12].
Dyslipidemia remains prevalent and challenging, with only a minority achieving low-density lipoprotein (LDL) targets due to older age, comorbidities, statin intolerance, and complex pharmacotherapy needs. The recent introduction of PCSK9 inhibitors and bempedoic acid offers additional options for high‑risk patients but remains limited by cost and regulatory constraints [13]. Obesity and overweight were highly prevalent, consistent with national trends, and contribute to multimorbidity and cardiovascular risk [14]. Tobacco exposure, although less common, remains relevant, particularly in those with long smoking histories [15].
Target organ damage, including cerebrovascular, renal, and cardiac disease, was frequent and necessitated ongoing adjustments in therapy, emphasizing the dynamic nature of risk management in older, high‑risk populations [8,9]. CKD, in particular, requires careful consideration of pharmacological interventions, as renal impairment alters drug metabolism and increases susceptibility to adverse effects [6]. Overall, these findings underscore the importance of patient‑centered, individualized care in high‑risk populations, balancing guideline‑based targets with age, frailty, comorbidities, and functional status to optimize cardiovascular outcomes and safety [10,13].
Limitations
Despite its clinical relevance, this study has several limitations. First, as a retrospective cohort, it relies on existing clinical records, which may lack complete data on patient adherence, frailty indices, functional status, and longitudinal outcomes beyond clinic visits. Second, the study was conducted in a specialized tertiary outpatient clinic, which may limit the generalizability of findings to broader primary care populations or to healthcare systems with different referral patterns. Third, although risk factor control was quantified, this design cannot establish causality between risk factor modification and clinical outcomes, such as cardiovascular events or mortality. Finally, we did not systematically assess patient-centered outcomes such as quality of life, which are increasingly recognized as important determinants of treatment tolerability and benefit in older adults.
Conclusions
This cohort demonstrates a high prevalence of multiple modifiable cardiovascular risk factors, underscoring the complexity of managing high-risk, aging populations in Portugal. Optimizing risk factor control requires continuous monitoring, individualized medication adjustments, patient education, and lifestyle interventions. Long-term follow-up in a specialized vascular risk clinic offers the advantage of maintaining patients' engagement with hospital care, ensuring adherence to pharmacotherapy, and achieving reasonable control of blood pressure, glycemia, and lipids despite challenges such as advanced age, multimorbidity, and treatment intolerance. Strengthening preventive strategies and implementing guideline-driven, patient-centered care remain essential to reduce acute cardiovascular events and their associated burden.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cardiovascular diseases (CV Ds) World Health Organization.(2025 July 31) 2025 https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-%28cvds%29
- 2Cardiovascular diseases 1720242024 https://www.who.int/europe/news-room/fact-sheets/item/cardiovascular-diseases
- 3Cardiovascular Disease Scorecards - Portugal World Heart Federation.(2023 2023 https://world-heart-federation.org/wp-content/uploads/WHF_SCORECARD-2024-Portugal.pdf
- 4Pathophysiology of coronary artery disease Circulation Libby P Theroux P 3481348811120051598326210.1161/CIRCULATIONAHA.105.537878 · doi ↗ · pubmed ↗
- 5SCORE 2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe Eur Heart J 243924544220213412017710.1093/eurheartj/ehab 309PMC 8248998 · doi ↗ · pubmed ↗
- 6SCORE 2-OP risk prediction algorithms: estimating incident cardiovascular event risk in older persons in four geographical risk regions Eur Heart J 24552467422021 https://doi.org/10.1093/eurheartj/ehab 3123412018510.1093/eurheartj/ehab 312PMC 8248997 · doi ↗ · pubmed ↗
- 72024 ESC guidelines for the management of elevated blood pressure and hypertension: developed by the task force on the management of elevated blood pressure and hypertension of the European Society of Cardiology (ESC) and endorsed by the European Society of Endocrinology (ESE) and the European Stroke Organisation (ESO)Eur Heart J Mc Evoy JW Mc Carthy CP Bruno RM 39124018452024
- 8Prevalence of cardiovascular risk factors and other comorbidities in patients with hypertension in Portuguese primary health care populations: the PRECISE study Rev Port Cardiol (Engl Ed) da Silva PM Lima MJ Neves PM de Macedo ME 4274373820193130772710.1016/j.repc.2018.09.011 · doi ↗ · pubmed ↗