Validation of performance of Spanish version of PURE-4 questionnaire for early identification of psoriatic arthritis after 1 year of follow-up in patients with psoriasis
R. Queiro-Silva, A. López-Ferrer, M. Ferran i Farrés, R. Rivera-Díaz, D. Vidal-Sarro, L. Rodríguez Fernández-Freire, P. de la Cueva-Dobao, J. Santos-Juanes, V. Rocamora-Duran, L. Gómez-Labrador, I. Belinchón-Romero, Wesam Gouda, Wesam Gouda, Wesam Gouda, Wesam Gouda

TL;DR
This study confirms the Spanish version of the PURE-4 questionnaire is effective for early detection of psoriatic arthritis in psoriasis patients over a one-year period.
Contribution
The study validates the long-term performance of the Spanish PURE-4 questionnaire for early PsA detection in clinical practice.
Findings
The PURE-4 questionnaire showed a sensitivity of 75.0% and specificity of 62.9% for PsA detection.
Patients with PsA had significantly higher PURE-4 scores than those without (p = 0.0016).
One in four PsA cases were detected one year after a positive PURE-4 response.
Abstract
Psoriatic arthritis (PsA) is an inflammatory, chronic and progressive musculoskeletal disease associated with psoriasis. The validation of the Spanish version of the Psoriatic arthritis UnclutteRed screening Evaluation (PURE-4) questionnaire has been published previously. The present analysis studied the performance of the PURE-4 questionnaire for the early detection of PsA one year before its diagnosis. This was an observational multicenter study, including two cross-sectional assessments, with primary data collection in routine clinical practice in Spain. Adult patients with psoriasis and confirmed not having PsA diagnosis during Assessment I completed Assessment II by the rheumatologist one year (±2 months) after answering the PURE-4 questionnaire. This work presents the results of Assessment II, to confirm/rule out the presence of PsA in patients with psoriasis one year after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
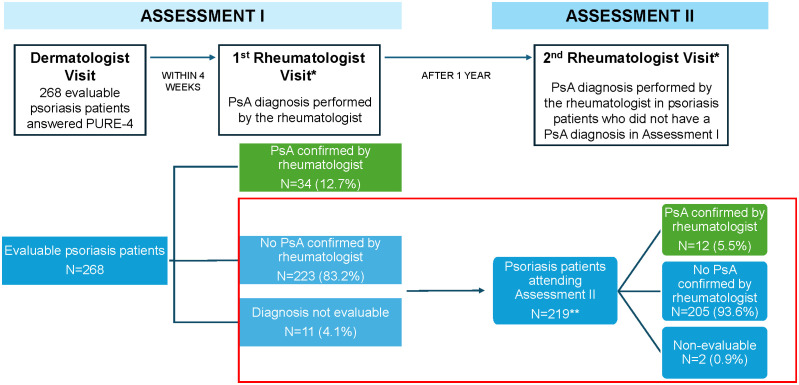 Fig 1
Fig 1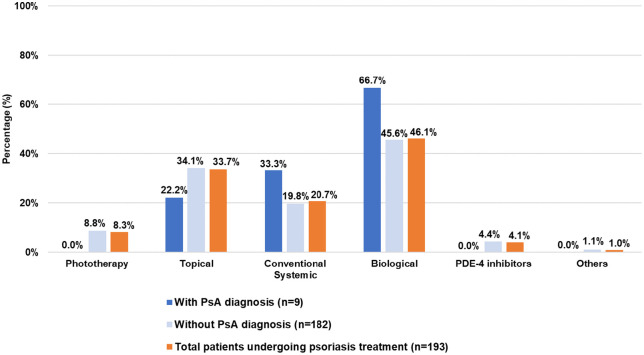 Fig 2
Fig 2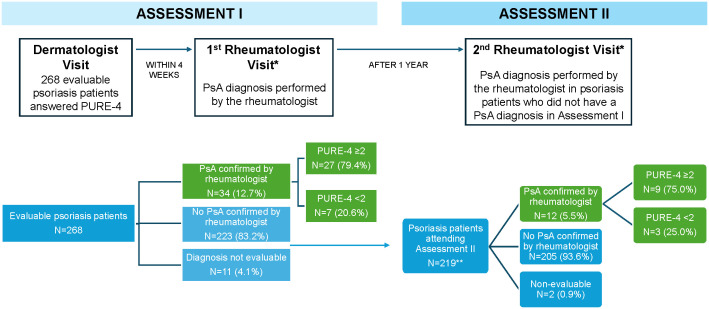 Fig 3
Fig 3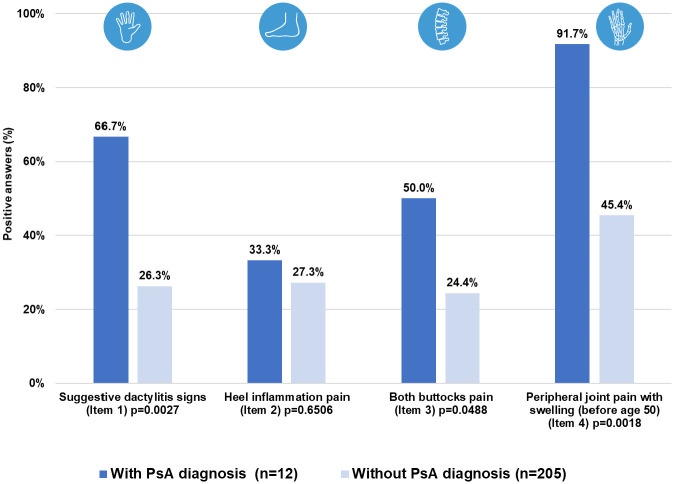 Fig 4
Fig 4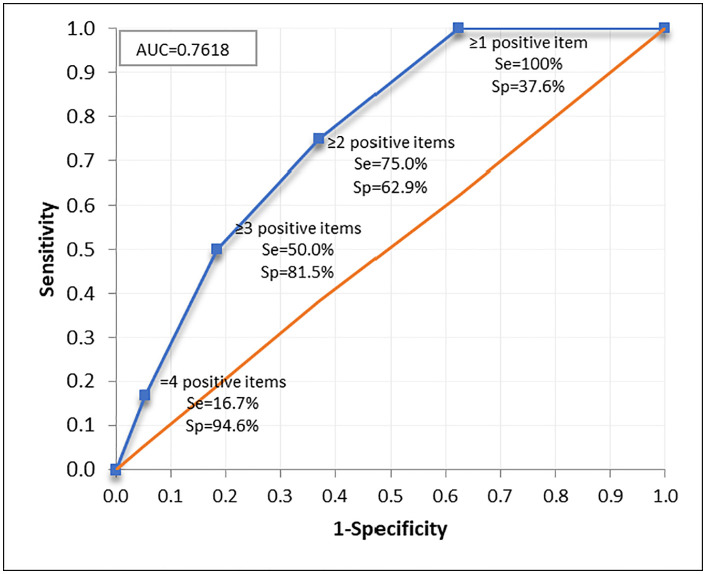 Fig 5
Fig 5- —http://dx.doi.org/10.13039/501100011772Novartis Farmacéutica
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpondyloarthritis Studies and Treatments · Psoriasis: Treatment and Pathogenesis · Rheumatoid Arthritis Research and Therapies
Introduction
Psoriatic arthritis (PsA) is an inflammatory, chronic and progressive musculoskeletal disease of recurrent course, with heterogeneous clinical manifestations and strongly associated with psoriasis, with a variable pattern of joint involvement [1]. According to data from the EPISER 2016 registry, the prevalence of PsA in the adult population in Spain is 0.58% [2], while the prevalence of psoriasis is 2.3% [3]. A study conducted in Canada estimated an annual incidence rate for PsA of 2.7% [4]. In 84% of individuals with psoriasis, the skin condition appears before the development of PsA [5].
PsA is a difficult diagnosis to make, and many cases go underdiagnosed; however, various studies place it between 15% and 40% of patients with psoriasis [5–7]. Delayed diagnosis contributes to the development of peripheral joint erosions and results in poor long-term physical function and health status, while an early diagnosis can help prevent or halt joint damage, thereby improving the clinical and radiological prognosis of the disease [6,8]. Although rheumatologists should ideally diagnose, treat, and monitor the course of PsA, as skin involvement usually precedes joint involvement in up to 84% of cases [9], in most cases, dermatologists are responsible for suspecting and screening for PsA. Dermatologists and primary care physicians must have simple screening tools at their disposal [1,10,11].
Although there are currently various tools for screening for PsA, they have not been culturally and linguistically adapted into Spanish, nor have they been validated through a structured development methodology within routine clinical practice in Spain [12]. The Psoriatic arthritis UnclutteRed screening Evaluation (PURE-4) questionnaire is a simple tool with only four items that evaluates signs suggestive of dactylitis, enthesitis, axial involvement, and peripheral involvement. It has recently been adapted linguistically and culturally for the Spanish population following the standardized methodology [11]. Following this adaptation, and with the aim of implementing the use of the questionnaire in clinical practice in Spain, it was validated and shown to be a sensitive (79.4%), specific (61.4%), and a feasible instrument for identifying patients with psoriasis at risk of developing PsA [13]. Finally, and as a continuation of this validation, this study analyzes for the first time the performance of the PURE-4 questionnaire as a tool for detecting patients at risk of developing PsA (one year after the questionnaire was completed).
Materials and methods
Study design
The cross-sectional, observational multicenter study was conducted in Spain, with primary data collection as per routine clinical practice in 19 public hospitals. Each hospital included a dermatology specialist and a rheumatology specialist who routinely assessed patients with psoriasis and PsA. All study visits were scheduled according to routine clinical practice. The study included adult (≥18 years) patients with psoriasis without a previous diagnosis of PsA who were consecutively enrolled based on clinical practice, as they met all the inclusion criteria and none of the exclusion criteria, and voluntarily agreed to participate [13]. More information about sites and study recruitment data is presented in S1 Table.
Study assessments
The study consisted of two cross-sectional assessments (Fig 1):
*Study design: This paper presents the results of Assessment II (boxed in red).*Rheumatologist was blinded during the two PsA assessments to the PURE-4 results. *15 patients did not attend the second visit to the rheumatologist. PsA, psoriatic arthritis.
Assessment I: From December 22, 2020, to August 17, 2021, patients were assessed by a dermatologist and completed two self-administered versions (in print and online) of the PURE-4 questionnaire. Thereafter, the rheumatologist, blinded to the PURE-4 results, assessed the presence/absence of PsA, being the reference to determine the performance of the PURE-4 questionnaire [13].Assessment II: Until November 17, 2022, psoriasis patients without a confirmed diagnosis of psoriatic arthritis at the initial assessment (Assessment I) were re-evaluated by a rheumatologist approximately one year later (±2 months) to determine the presence of PsA based on clinical judgment.
The results of Assessment I allowed for the validation of the Spanish version of the PURE-4 questionnaire and were previously reported [13]. This paper presents the results of Assessment II, the aim of which was to analyze the performance of the PURE-4 questionnaire as a tool for the early detection of PsA one year after having answered it (in Assessment I) to confirm/rule out the presence of PsA in patients with psoriasis and patients without a diagnosis of PsA after Assessment I.
The study variables included, but were not limited to, the sociodemographic and clinical data of the patients [13]. In Assessment II, the sensitivity and specificity of the PURE-4 questionnaire were studied to confirm the presence/absence of PsA in patients without a diagnosis of PsA after Assessment I one year after answering the PURE-4 questionnaire.
The reporting of this study conforms to STROBE guidelines [14].
Statistical analysis
Two statistical analyses were planned, the first of which was previously reported [13]. The second and final analysis involved the results of Assessment II to assess the performance of the PURE-4 questionnaire for the early detection of potential PsA one year after completing the PURE-4 questionnaire, in terms of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the percentage of patients correctly classified, with a 95% confidence interval (95% CI).
The area under the receiver–operating characteristic (ROC) curve with its 95% CI was calculated to assess the capacity or quality of the PURE-4 questionnaire to identify patients with PsA, considering the final diagnostic confirmation performed by the rheumatologist.
To select optimal cut-off score, the Youden index was calculated. The cut-off score associated with the highest index is considered to indicate the optimal cut-off point. Youden index is the maximum vertical distance or difference between the ROC curve and the diagonal or chance line and occurs at the cut point that optimizes the biomarker’s differentiating ability when equal weight is given to sensitivity and specificity.
In Assessment II, for a specificity ≥0.80 with a precision of 5.2 percentage points and a significance level of 0.05, a subsample of 227 patients without a diagnosis of PsA would be needed. Assuming a 10% loss rate, for the validation of the questionnaire in terms of sensitivity and specificity for the early detection of PsA, the number of patients required would be 205.
The PURE-4 questionnaire scores were obtained only in Assessment I and were compared with the presence or absence of PsA according to the clinical judgment of the rheumatologist in Assessment II (one year later).
A descriptive analysis of the sociodemographic and clinical characteristics was performed. Psoriasis Area and Severity Index (PASI), body surface area (BSA), Physician Global Assessment (PGA), Dermatology Life Quality Index (DLQI), and CASPAR criteria were also described. When the rheumatologist considered necessary, dactylitis, enthesitis, inflammatory back and peripheral joint pain were assessed by complementary tests, according to clinical practice, and also described.
Quantitative data were described using valid N, missing N, mean, standard deviations (SDs), extreme values and quartiles. Categorical variables were described using frequencies and percentages in relation to class level. In both cases, the number of observations and the number of missing data were specified. No imputation of missing values was performed for any variable. Comparisons between patients with and without a diagnosis of PsA were performed using T-tests, Mann-Whitney and Chi-square tests, without taking into account the subgroup with a non-evaluable diagnosis and considering a statistical significance level of 0.05. The statistical software Statistical Analysis System (SAS) Enterprise Guide version 7.15 was used.
Ethical statement
The study was performed in accordance with the ethical principles of the Declaration of Helsinki and the guidelines specified in Order SAS/3470/2009 of the Spanish Agency of Medicines and Medical Devices (AEMPS). The protocol, informed consent, and patient information were approved by the central Ethics Committee (EC) of the Hospital de Bellvitge, as well as by all the ECs and autonomous communities of the participating hospitals, as required. All patients signed written informed consent before enrollment in the study.
Results
In Assessment I, a total of 283 patients were enrolled, of whom 268 (94.7%) were evaluable. Of note, 34 (12.7%) were diagnosed with PsA [13]. In Assessment II, 219 patients with psoriasis and no diagnosis of PsA were included and made a second visit to the rheumatologist.
In Assessment II (n = 219), the diagnosis of PsA was confirmed in 12 (5.5%) patients. Taking into account both study assessments (n = 253), a total of 46 patients (18.2%) with PsA were identified [13].
It was not possible to determine whether or not 15 of the 268 evaluable patients in the study had PsA. Hence, it is considered that in 253 patients (94.4%), the diagnosis of PsA could be confirmed or ruled out.
Baseline characteristics of patients included in Assessment II
At Assessment II, the mean (SD) age was 43.4 (12.5) years for patients with a diagnosis of PsA and 47.0 (12.5) years for those without a diagnosis of PsA. Of the patients with and without a diagnosis of PsA, 66.7% and 56.1%, respectively, were male. The mean time from the first diagnosis of psoriasis to inclusion in the study was longer in patients with a diagnosis of PsA than in those without PsA (21.0 vs. 18.7 years). Overall, patients with PsA had a higher percentage of dactylitis (8.3%), enthesitis (16.7%), inflammatory back pain (16.7%), and peripheral joint pain (58.3%) than patients without PsA (0%, 0%, 1.0%, and 3.4%, respectively) (Table 1).
Table 1: Baseline clinical and sociodemographic characteristics of evaluable psoriasis patients who attended Assessment II (variables collected in Assessment I).
A total of 88.1% of patients included in Assessment II were on treatment for psoriasis, mainly with biologic drugs (46.1%) (Fig 2).
Baseline treatment of patients undergoing psoriasis treatment included in Assessment II.PDE-4, phosphodiesterase 4; PsA, psoriatic arthritis.
More information on the overall results of the study is presented in S2 Table and S1 Fig.
Assessment II: Performance of the PURE-4 questionnaire in early PsA identification
Throughout the study, 78.2% of patients diagnosed with PsA scored ≥2 on the PURE-4 questionnaire at baseline, with 79.4% being those diagnosed in Assessment I [13] and 75.0% in Assessment II (Fig 3).
*Flowchart of study population (Assessment I and Assessment II).*Rheumatologist was blinded during the two PsA assessments to the PURE-4 results. *15 patients did not attend the second visit to the rheumatologist. PsA, psoriatic arthritis.
In Assessment I, the rheumatologist was unable to confirm the diagnosis of PsA in 14 patients, responding “currently no, but presents signs and/or symptoms suggestive of early stage PsA.” Two of these 14 patients did not attend the second visit to the rheumatologist, and of those patients who attended, 4 (33.3%) were diagnosed with PsA.
In Assessment II, the mean (SD) PURE-4 score was 2.4 (1.1) among patients with PsA and 1.2 (1.2) among patients without a diagnosis of PsA (Table 2). Regarding the questionnaire items, patients with PsA showed greater presence of all of the items than patients without PsA, with peripheral joint pain with swelling before the age of 50 years (item 4) being the most prevalent symptom, and inflammatory heel pain (item 2) being the only one that did not show significant differences between patients with and without PsA (Fig 4).
Table 2: Results of PURE-4 questionnaire in Assessment II.
Results of PURE-4 questionnaire by item in Assessment II.n, number of patients; PsA, psoriatic arthritis.
Items 2 and 4 of the questionnaire showed the greatest difference among patients with a diagnosis of PsA in the two assessments (S2 Fig).
Sensitivity and specificity
The sensitivity and specificity of the questionnaire were evaluated considering those patients with psoriasis in whom the presence/absence of PsA was confirmed by a rheumatologist in Assessment II (n = 217), showing that the area under the ROC curve was 0.7618 (95% CI: 0.6530–0.8706), indicating the good performance of the questionnaire in the identification of early PsA (Fig 5).
Area under ROC curve in Assessment II.AUC, area under the curve; ROC, receiver-operating characteristic; Se, sensitivity; Sp, specificity.
At one-year follow-up after answering the PURE-4 questionnaire, sensitivity was 75.0% and specificity 62.9%. In 63.6% of the cases, the PURE-4 questionnaire classified the patients in the same way as the rheumatologist, with an NPV of 97.7% (Table 3).
Table 3: Sensitivity and specificity results for Assessment II.
Using the Youden index, it was determined, as in Assessment I, that a score ≥2 was the optimal cut-off point that allowed screening for the presence of potential PsA [13]. In Assessment II, the Youden index was very similar between the scores of 1 and 2 but, if score 1 was chosen, the specificity was much lower, with only 37.6% of patients who did not actually have a diagnosis of PsA being classified as not having a diagnosis of PsA (Table 3).
Discussion
The identification of the patients with psoriasis at an increased risk of developing PsA, together with the early diagnosis of PsA, is of considerable scientific and clinical interest, as early diagnosis and treatment of PsA have been shown to delay and/or prevent permanent disability [15,16]. The role of dermatologists is crucial for the early detection and prompt referral of the patient with psoriasis at risk of PsA or with suspected PsA, and ultimately, early intervention by rheumatologists to prevent the progression of PsA, as well as the associated disability and associated comorbidities [1,16].
Recently, a group of the European Alliance of Associations for Rheumatology (EULAR) developed a guideline to define the suspected features of psoriasis progression to PsA and the clinical management of these patients [15]. This guideline includes three relevant stages for the progression of PsA: patients with psoriasis at increased risk of developing PsA, subclinical PsA, and clinical PsA [15]. All people with psoriasis are at risk of developing PsA, highlighting arthralgia as a key element of subclinical PsA that can be used as a possible short-term predictor of the development of PsA [15]. The present study was designed to validate the PURE-4 questionnaire for the early screening for PsA in patients with psoriasis receiving routine dermatologic care in Spain (assessment I) [13], and to validate, for the first time, its potential as a tool for the detection of early PsA (Assessment II) one year after answering the PURE-4 questionnaire, demonstrating its good screening properties with an optimal cut-off point of ≥2. Furthermore, peripheral joint pain with swelling before the age of 50 (item 4) was observed to be the most prevalent symptom, in line with what EULAR indicates for the detection of subclinical PsA [15].
Some studies show that more than half of patients with PsA are diagnosed with years of delay [17], which is especially significant in Spain, with a mean of 4.0 ± 1.4 years [18]. Therefore, it is imperative to include a PsA screening tool that enables early detection in patients with psoriasis in clinical practice.
In addition to the points to be taken into account recommended by the EULAR group [15], the capacity for early detection of PsA was evaluated with the Early Arthritis for Psoriatic Patients (EARP) questionnaire [19], which concluded that it was effective with a specificity of 62%. However, a subsequent external validation of the EARP questionnaire showed a particularly low specificity (34%) [20]. Taking these results into account, PURE-4 seems to be a suitable screening questionnaire to detect PsA early, with a score ≥2 as optimal cut-off point, and both for its sensitivity (75.0%) and specificity (62.9%), which is especially relevant for a potentially disabling disease where the musculoskeletal health of patients is not only affected by aging, but also by the persistent increase or chronification of the inflammatory state [21,22]. Audureau E, et al, in a publication whose objective was to describe the development and internal validation of the PURE-4 questionnaire in a single center (not in a multicenter manner as in the case of the present manuscript) and which did not validate the performance of the tool 1 year before the diagnosis of PsA, obtained results aligned with our results, although slightly higher, where development and first validation of the PURE-4 scale showed a sensitivity of 85.7% and a specificity of 83.6% at the threshold of ≥1 positive item [12].
In these patients, early diagnosis can lead to prompt medical treatment and early lifestyle modifications, with a potential role in preventing joint deterioration, pain management, and quality of life [15,21,22]. Furthermore, although not analyzed in the present study, it is worth noting that some studies show a significant decrease in the risk of developing PsA in patients with psoriasis who receive biological treatments, concluding that the use of biological drugs should be considered at an earlier stage of treatment in patients who have significant risk factors for PsA [23,24].
The cumulative incidence of PsA in psoriasis patients ranges from 5.1% at 20 years to 20.5% at 30 years after the onset of psoriasis, being the annual incidence rate of PsA of 2.7% (95% CI: 2.1–3.6) in Canada, while the annual incidence rate of PsA in psoriasis patients without baseline arthritis was 1.87% in a prospective cohort study [4]. In the present study, an additional 5.5% of patients with PsA were identified one year after answering the PURE-4 questionnaire, in line with previous studies [19,25]. These percentages are higher than those detected in a previous epidemiologic survey, with around 10% of patients after a decade of follow-up [26].
The usefulness of the PURE-4 questionnaire in identifying PsA, even early, could be explained, in part, by its specific PsA items, including, among others, the age component (peripheral joint pain with swelling in patients <50 years), and it is one of the two questionnaires that include bilateral buttock pain [27].
The good performance of the PURE-4 questionnaire in its Spanish version in terms of sensitivity and specificity [13], as well as the fact that it includes four key questions on the identification of PsA, makes this questionnaire a tool that is easy to apply and viable in routine clinical practice considering the optimal cut-off point of ≥2 [27]. Furthermore, it is a quick questionnaire to use, and considering its high sensitivity, it could be useful to encourage its use at different time points (e.g., annually or in case of clinical doubt) to increase the identification of possible cases of PsA.
This study has some limitations inherent to the methodology used. The fact that the PURE-4 questionnaire was completed only at the beginning of the study (Assessment I) did not allow us to extend the initial objectives of the study by also assessing sensitivity to change or test-retest reliability. Consequently, administering the questionnaire only once limits the ability to evaluate the reproducibility of the score over time. This is the first time the performance of the PURE-4 questionnaire has been tested for detecting PsA with a one-year interval between its administration and diagnosis. This fact is significant because it is recommended to screen psoriasis patients once a year (ideally, every six months), and the PURE-4 serves as a screening aid for PsA, although it does not absolve the responsibility of evaluating the patient, including their risk factors. Finally, given the small number of PsA cases at one year (n = 12), 95% CI are wide, and results should be interpreted with caution.
Conclusions
The PURE-4 screening questionnaire has been shown to be a sensitive, specific, and feasible instrument to identify the risk of developing PsA in patients with psoriasis and, therefore, valid for application in Spanish dermatologic clinical practice. Its implementation is expected to reduce the rates of underdiagnosis of PsA by allowing dermatologists to refer patients early for early rheumatologic care. The data collected in our study allowed us to detect 46 (18.2%) patients with a diagnosis of PsA in one year: 34 (73.9%) at baseline and 12 (26.1%) after one year, which reinforces the recommendation to assess the presence of PsA annually [11], as well as to identify those patients at a higher risk of developing PsA for closer follow-up, as this could help to prevent irreversible joint damage in the context of this disease.
Supporting information
S1 TableSites and study recruitment data.FPFV, First Patient First Visit; LPLV, Last Patient Last Visit; SIV, Site Initiation Visit.(DOCX)
S2 TableBaseline clinical and sociodemographic characteristics of all evaluable psoriasis patients enrolled in Assessment I and Assessment II (variables collected in Assessment I).BSA, body surface area; DLQI, Dermatology Life Quality Index; n, number of patients (unless otherwise specified); PASI, Psoriasis Area and Severity Index; PGA, Physician Global Assessment; PsA, psoriatic arthritis; SD, standard deviation.(DOCX)
S1 FigBaseline treatment of patients with psoriasis enrolled in study*.*Only those patients for whom treatment was indicated are included (treatment was not indicated in 29 patients, of whom 6 were diagnosed with PsA). **Total patients on treatment for psoriasis does not include 2 patients in whom the diagnosis of PsA was not evaluable. PDE-4, phosphodiesterase 4; PsA, psoriatic arthritis.(TIFF)
S2 FigComparative analysis of PURE-4 questionnaire scores by item in patients with PsA at Assessment I and Assessment II.n, number of patients; PsA, psoriatic arthritis.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Torre Alonso JC, Díaz Del Campo Fontecha P, Almodóvar R, Cañete JD, Montilla Morales C, Moreno M, et al. Recommendations of the Spanish Society of Rheumatology on treatment and use of systemic biological and non-biological therapies in psoriatic arthritis. Reumatol Clin (Engl Ed). 2018;14(5):254–68. doi: 10.1016/j.reuma.2017.08.007 29111261 · doi ↗ · pubmed ↗
- 2Seoane-Mato D, Sánchez-Piedra C, Silva-Fernández L, Sivera F, Blanco FJ, Pérez Ruiz F, et al. Prevalence of rheumatic diseases in adult population in Spain (EPISER 2016 study): Aims and methodology. Reumatol Clin (Engl Ed). 2019;15(2):90–6. doi: 10.1016/j.reuma.2017.06.009 28774657 · doi ↗ · pubmed ↗
- 3Ferrándiz C, Carrascosa JM, Toro M. Prevalence of psoriasis in Spain in the age of biologics. Actas Dermosifiliogr. 2014;105(5):504–9. doi: 10.1016/j.ad.2013.12.008 24569109 · doi ↗ · pubmed ↗
- 4Eder L, Haddad A, Rosen CF, Lee K-A, Chandran V, Cook R, et al. The Incidence and Risk Factors for Psoriatic Arthritis in Patients With Psoriasis: A Prospective Cohort Study. Arthritis Rheumatol. 2016;68(4):915–23. doi: 10.1002/art.39494 26555117 · doi ↗ · pubmed ↗
- 5Villani AP, Rouzaud M, Sevrain M, Barnetche T, Paul C, Richard M-A, et al. Prevalence of undiagnosed psoriatic arthritis among psoriasis patients: Systematic review and meta-analysis. J Am Acad Dermatol. 2015;73(2):242–8. doi: 10.1016/j.jaad.2015.05.001 26054432 · doi ↗ · pubmed ↗
- 6Haroon M, Gallagher P, Fitz Gerald O. Diagnostic delay of more than 6 months contributes to poor radiographic and functional outcome in psoriatic arthritis. Ann Rheum Dis. 2015;74(6):1045–50. doi: 10.1136/annrheumdis-2013-204858 24525911 · doi ↗ · pubmed ↗
- 7Mease PJ, Gladman DD, Papp KA, Khraishi MM, Thaçi D, Behrens F, et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. 2013;69(5):729–35. doi: 10.1016/j.jaad.2013.07.023 23981683 · doi ↗ · pubmed ↗
- 8Giovannini I, Bosch P, Dejaco C, De Marco G, Mc Gonagle D, Quartuccio L, et al. The Digital Way to Intercept Psoriatic Arthritis. Front Med (Lausanne). 2021;8:792972. doi: 10.3389/fmed.2021.792972 34888334 PMC 8650082 · doi ↗ · pubmed ↗