An Immigrant With Intestinal Myiasis in the United States: A Case Report and a Review of the Literature
Faris Shweikeh, Jad Kabbara, Colin Fricker, Mohamad Mouchli

TL;DR
A case report describes a rare intestinal myiasis diagnosis in a U.S. patient, emphasizing the importance of considering this condition in patients with chronic gastrointestinal symptoms.
Contribution
This case report highlights intestinal myiasis as a rare but diagnosable condition using endoscopy and emphasizes its relevance in patients with travel or dietary exposure to endemic regions.
Findings
Intestinal myiasis was diagnosed via endoscopic visualization and biopsy in a patient with chronic gastrointestinal symptoms.
The patient's symptoms resolved with mechanical washout and supportive care, avoiding unnecessary invasive procedures.
The case underscores the importance of considering myiasis in patients with unexplained chronic GI symptoms and relevant exposure history.
Abstract
Myiasis is an infestation of human tissue by fly larvae. Intestinal myiasis occurs when fly eggs or larvae in contaminated food or water survive passage through the gastrointestinal tract and are found in the stool or bowel lumen. It is more prevalent in developing countries and can present with nonspecific gastrointestinal symptoms that mimic common conditions. A 55-year-old Nepalese-American woman, with a long history of intermittent abdominal pain, nausea, and vomiting, underwent CT imaging, which demonstrated a 2 cm colonic narrowing with wall thickening of the proximal transverse colon. Colonoscopy revealed larvae in the terminal ileum and transverse colon, with adjacent inflammation, and biopsy showed eosinophilic infiltration. Microbiology identified eggs that could not be speciated, and a working diagnosis of intestinal myiasis was made. The patient received bowel preparation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
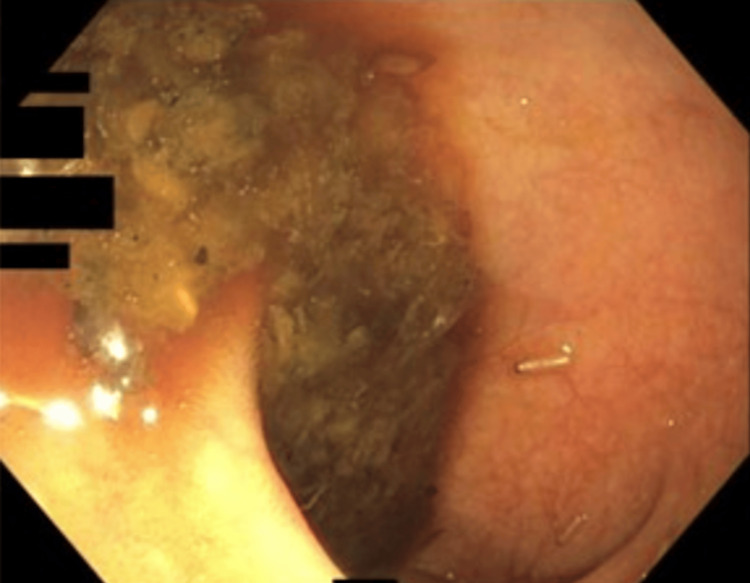 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Entomology and Diptera Studies · Insect Utilization and Effects · Parasitic Diseases Research and Treatment
Introduction
Myiasis is defined as an infestation of human tissue by fly larvae, a phenomenon that commonly involves the skin or natural orifices and is prevalent in tropical regions [1]. There are multiple presentations of myiasis, with the most common being cutaneous myiasis [2]. However, a particularly rare form is intestinal myiasis, which occurs when fly eggs or larvae present in food or water are ingested and survive passage through the gastrointestinal tract.
As stomach acidity is a harsh environment for many pathogens, larvae that cannot endure gastric acidity and perish are termed pseudomyiasis. Due to the harsh nature of the gastrointestinal environment and the unsuitability of humans as a host, true intestinal myiasis is usually accidental; therefore, it is rare for flies to have an ongoing life cycle within the gut mucosa [2]. Clinical manifestations of intestinal myiasis are variable: patients may be entirely asymptomatic, or may have nonspecific gastrointestinal complaints such as abdominal pain, nausea, vomiting, diarrhea, or even rectal bleeding [3]. Because symptoms often mimic other conditions, diagnosis is rarely suspected until larvae are observed in the stool or during endoscopic evaluation.
Fly species implicated in intestinal myiasis span several families, with causative genera including Musca, Sarcophaga, Lucilia, Eristalis, Hermetia, and drain flies [2-4]. Notably, most documented cases occur in individuals from endemic regions with exposure to contaminated food and water, making intestinal myiasis in the United States a diagnosis that can be easily overlooked. To our knowledge, only 13 cases were reported in developed countries between 2000 and 2019. Therefore, to our knowledge, we describe the first reported case in the United States of intestinal myiasis in a Nepalese-American patient with chronic gastrointestinal symptoms, with a discussion of the relevant literature.
This article was previously presented as a meeting abstract at the 2024 ACG EPoster conference on October 28, 2024.
Case presentation
A 55-year-old Nepalese woman who immigrated to the United States over a decade ago, with a past medical history of multinodular thyroid disease and latent tuberculosis, had undergone an extensive workup for chronic intermittent abdominal pain, nausea, and vomiting five years prior, which was inconclusive. She was taking linaclotide, hyoscyamine, docusate sodium, polyethylene glycol, and omeprazole. Her diet consisted of well-cooked meat, rice, yogurt, and vegetables, and she often shopped at a local Nepalese grocery store. Her water at home was purified city water.
After presenting to the Emergency Department for worsening symptoms, she was directed to follow up with her primary care physician and gastroenterologist. CT imaging showed a 2 cm colonic narrowing and wall thickening in the proximal transverse colon. On colonoscopy, larvae of an unknown parasite were found in the terminal ileum and transverse colon (Figures 1-2), along with inflammation and a stricture. She had three previous colonoscopies that were unrevealing. A biopsy of the colon taken near the larvae demonstrated eosinophilic infiltration. Microbiologic identification of collected samples showed saprophagous insect eggs that could not be speciated. Based on these findings, a diagnosis of intestinal myiasis was suggested. She was referred to an infectious disease specialist, and a bowel preparation regimen was initiated over multiple days to wash out the parasites, leading to the resolution of her symptoms.
Low-power endoscopic view of the proximal transverse colon, showing luminal debris and a single translucent, segmented larva adherent to inflamed mucosa.
Higher-magnification endoscopic close-up demonstrating multiple live, translucent, segmented larvae attached to the mucosal surface, with adjacent erythema. A biopsy taken from the nearby mucosa demonstrated eosinophilic infiltration.
Discussion
The Centers for Disease Control and Prevention has linked intestinal myiasis to ingestion of fly-infested food, making it an uncommon manifestation in developed countries and more prevalent in areas with poor sanitation and tropical environments [1]. Synanthropic flies can deposit eggs on fruits or other foods that are then ingested, allowing larvae to pass through the gut and into the colon. Species diversity among implicated flies is broad, ranging from common houseflies (Musca domestica) and flesh flies (Sarcophaga spp.) to drain flies (Clogmia albipunctata), which thrive in indoor environments, such as drains and bathrooms, and deposit larvae that feed on decaying organic matter.
C. albipunctata has been documented in cases of intestinal myiasis, with a recent report emphasizing accidental ingestion of larvae-contaminated food, leading to symptoms such as nausea, vomiting, and abdominal discomfort, similar to those present in our patient [5]. Common symptoms of intestinal myiasis include abdominal pain, nausea, vomiting, diarrhea, and rectal itching, with our patient exhibiting intermittent abdominal pain and vomiting, likely reflecting episodic irritation by the larvae. However, not all cases present with symptoms; a prior case report described an asymptomatic Peruvian child with incidental findings of stool contaminated with larvae of Sarcophaga during examination [3]. Although some patients may be asymptomatic, other reports have noted abdominal discomfort and passage of live larvae in stool, contributing to variability in clinical presentation and delayed diagnosis [6]. Although the patient reported gastrointestinal symptoms for several years, it remains unclear whether intestinal myiasis was a longstanding process, or a more recent, intermittent exposure superimposed on chronic gastrointestinal complaints. This temporal uncertainty represents an important diagnostic challenge and limitation of this case. The transverse colonic stricture and wall thickening observed on imaging raised concern for chronic inflammatory changes; however, in the absence of follow-up endoscopic or radiologic evaluation, a direct causal relationship with larval presence cannot be definitively established.
Diagnosis of intestinal myiasis is often made by direct visualization of larvae in stool or during endoscopy, which was the key finding in our patient, who had live larvae on colonoscopy. To confirm the fly family, morphological identification of the larvae can be performed. It is important to differentiate true intestinal myiasis from pseudomyiasis, in which ingested larvae die in the gut without establishing infestation. True infestation requires larval survival and often implies ongoing presence or multiple larvae. The presence of numerous larvae in consecutive stool samples, or endoscopic findings with symptom relief after removal, supports true myiasis [7].
Management of intestinal myiasis is primarily mechanical and includes bowel lavage, washout, removal when accessible endoscopically, and measures to reduce re-exposure, such as improved food hygiene and sanitation in food preparation environments. Antiparasitic medications are not uniformly recommended or effective for many larvae, and evacuation/washout remains the first-line approach [8].
Conclusions
This case highlights the diagnostic challenges posed by intestinal myiasis, a condition rarely encountered in developed regions, and often identified only when larvae are directly visualized. Our patient’s course illustrates how nonspecific symptoms and limited awareness can prolong diagnosis, with endoscopic detection providing diagnostic clarity. Recognition of potential exposure pathways, even years after migration, remains an important adjunct to diagnosis. Mechanical removal and hygiene counseling remain first-line management and the most effective treatment for intestinal myiasis. Increased clinician awareness is essential to avoid delayed diagnosis and ensure timely, appropriate care. As a single case report, this observation cannot be used to infer incidence, prevalence, or definitive risk factors, but rather serves to highlight a rare diagnostic consideration in patients with unexplained gastrointestinal symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intestinal myiasis MMWR Morb Mortal Wkly Rep Centers for Disease Control and Prevention 503311982 https://www.cdc.gov/mmwr/preview/mmwrhtml/00000503.htm
- 2Intestinal myiasis caused by Clogmia albipunctata in Nepal: a case report J Med Case Rep Chalise BS Gupta SK Pradhan S Khanal A Bajracharya M Bausla Y Chalise SP 1031920254005578910.1186/s 13256-024-04881-w PMC 11887259 · doi ↗ · pubmed ↗
- 3Intestinal myiasis caused by Sarcophaga spp. in Cusco, Peru: a case report and review of the literature Case Rep Infect Dis Ly P Aizenberg A Martin T Lopez M Arturo Saldaña M Hughes GL Cabada MM 3685439201820182997763210.1155/2018/3685439 PMC 5994300 · doi ↗ · pubmed ↗
- 4Persistent pediatric gastro-intestinal myiasis: a case report of fly larval infestation with Musca domestica with review of literature J Glob Infect Dis Kandi V Lal SK Sandhya K 114117520132404936610.4103/0974-777X.116874 PMC 3766333 · doi ↗ · pubmed ↗
- 5A rare case of residual root myiasis caused by Clogmia albipunctata larvae (Diptera: Psychodidae)BMC Infect Dis Chen J Liu J Liu Y Liu Y 3742220223541801710.1186/s 12879-022-07325-2PMC 9009001 · doi ↗ · pubmed ↗
- 6Eristalis tenax intestinal myiasis: an electron microscope study Trop Parasitol Tolba MM 3943102020 https://pmc.ncbi.nlm.nih.gov/articles/PMC 7365507/3277529110.4103/tp.TP_40_19PMC 7365507 · doi ↗ · pubmed ↗
- 7Two cases of enteric myiasis in man. Pseudomyiasis and true intestinal myiasis Am J Clin Pathol Kenney M Eveland LK Yermakov V Kassouny DY 78679166197698398710.1093/ajcp/66.5.786 · doi ↗ · pubmed ↗
- 8Myiasis treatment and management: emergency department care, complications, prevention 2025 https://emedicine.medscape.com/article/1491170-treatment